Authors: Alex Bonilla, MD (Emergency Medicine Resident, Icahn School of Medicine at Mount Sinai); Summer Chavez, DO, MPH, MPM (Attending Physician, The University of Texas Health Science Center at Houston) // Reviewed by: Alex Koyfman, MD (@EMHighAK)
What is the issue?
On December 27, 2020, President Trump signed the Consolidated Appropriations Act, 2021 (H.R. 133), a $2.3 trillion package consisting of the COVID relief bill and other crucial healthcare funding, into law.1 This legislation continues to fund the fight against the COVID-19 pandemic, addresses Surprise Medical Billing and expands Medicare & Medicaid funding. All of which benefits patients, physicians and the medical system at large.
The $900 billion COVID Relief Bill builds on previous legislation, including the Coronavirus Preparedness and Response Supplemental Appropriations Act and the Coronavirus Aid, Relief, and Economic Security (CARES) Act1,2,3. The bill directs funding for:
- Vaccine development, procurement and distribution
- COVID-19 testing and contact tracing
- NIH funding for COVID-19 related research and clinical trials
- Centers for Disease Control and Prevention (CDC) to coordinate coronavirus vaccine distribution and access
- The Provider Relief Fund
- Paycheck Protection Program
- Student loan payments deferred until 1/31/2021
Among other things, the Appropriations Act also includes several Medicare & Medicaid provisions1,2:
- $3 billion to the Medicare Physician Fee Schedule (PFS) – increases fee schedules by 3.75%
- 3-year delay for the CMS G2211 complex patient visits add-on code – initially accounted for 3% of PFS conversion factor cut
- 2% cuts from Medicare sequestration delayed until 3/31/2021
- Adds 1,000 new physician GME slots starting in 2023 – prioritizes teaching hospitals in rural and underserved areas
- Nixes Medicaid Disproportionate Share Hospital (DSH) cuts for FY 21-23
- Option for Critical Access Hospitals and rural hospitals to convert to Rural Emergency Hospitals
In terms of Surprise Medical Billing, which will go into effect in 2022, the legislation includes1,3,4:
- An accessible independent dispute resolution (IDR) between providers and insurers
- Limits to deductibles for out of network emergency care and air ambulance services
- Improves health care transparency
- Requires insurers disclose policyholder’s deductibles (in-network and out-of-network) on their insurance card
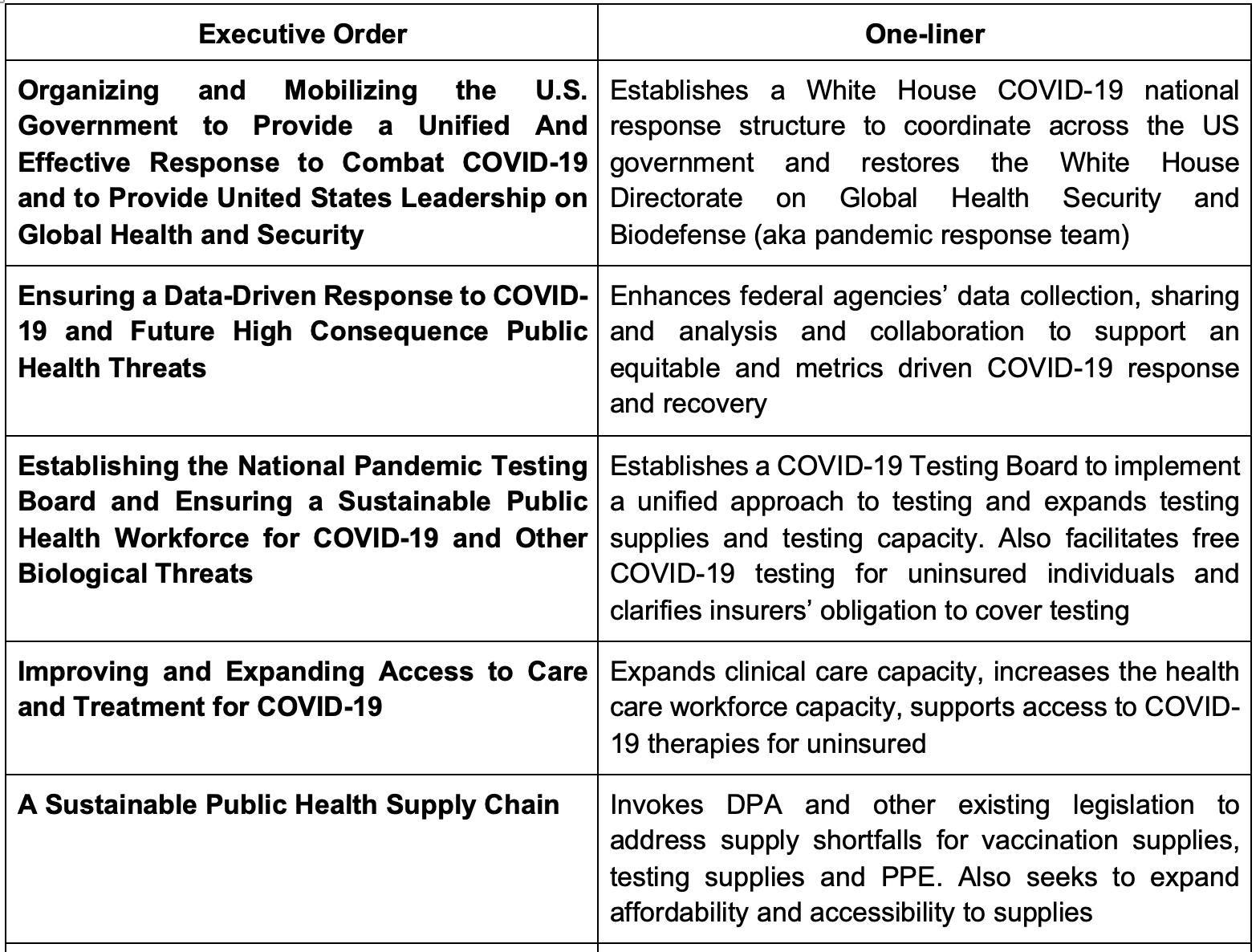
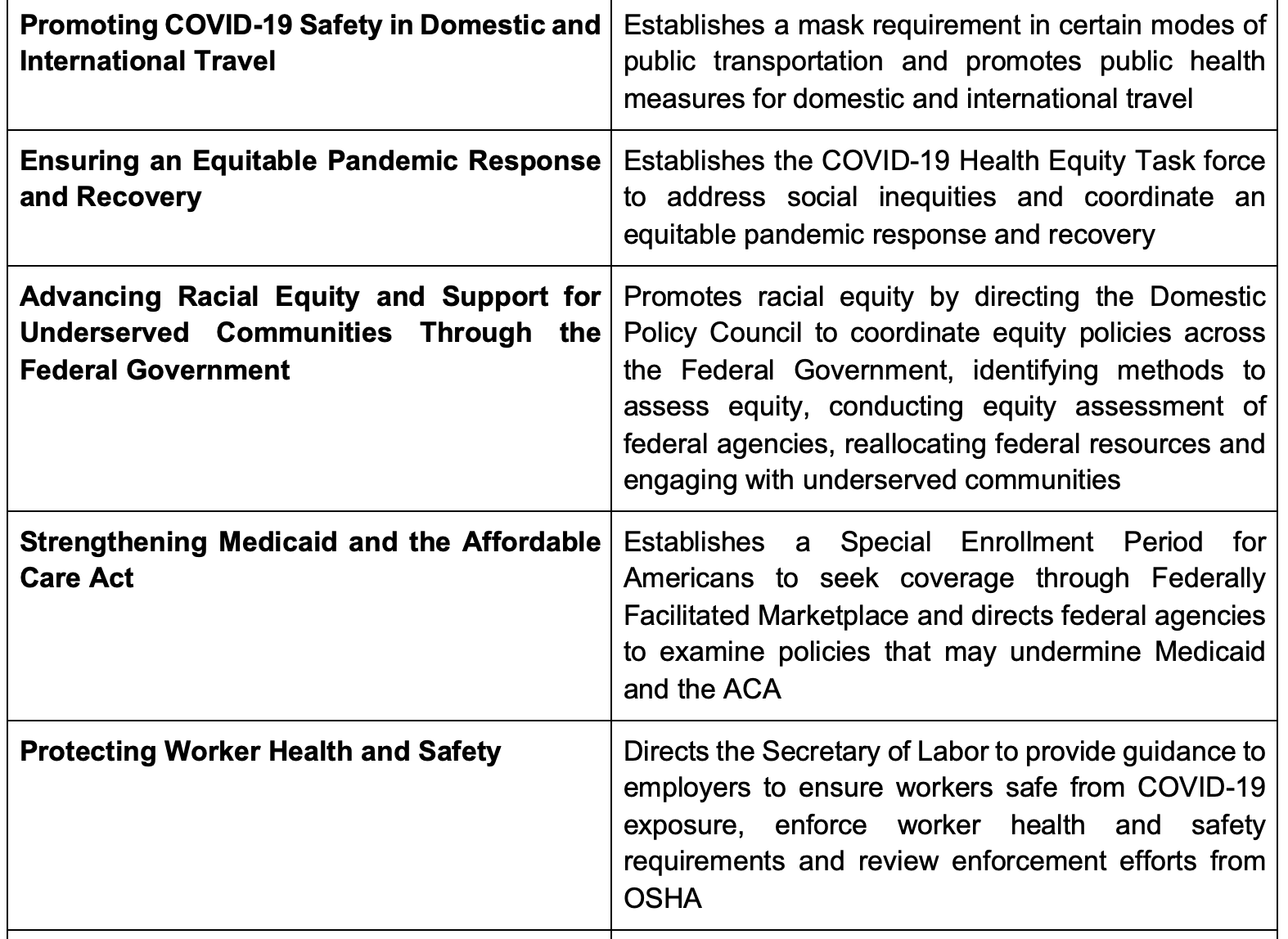
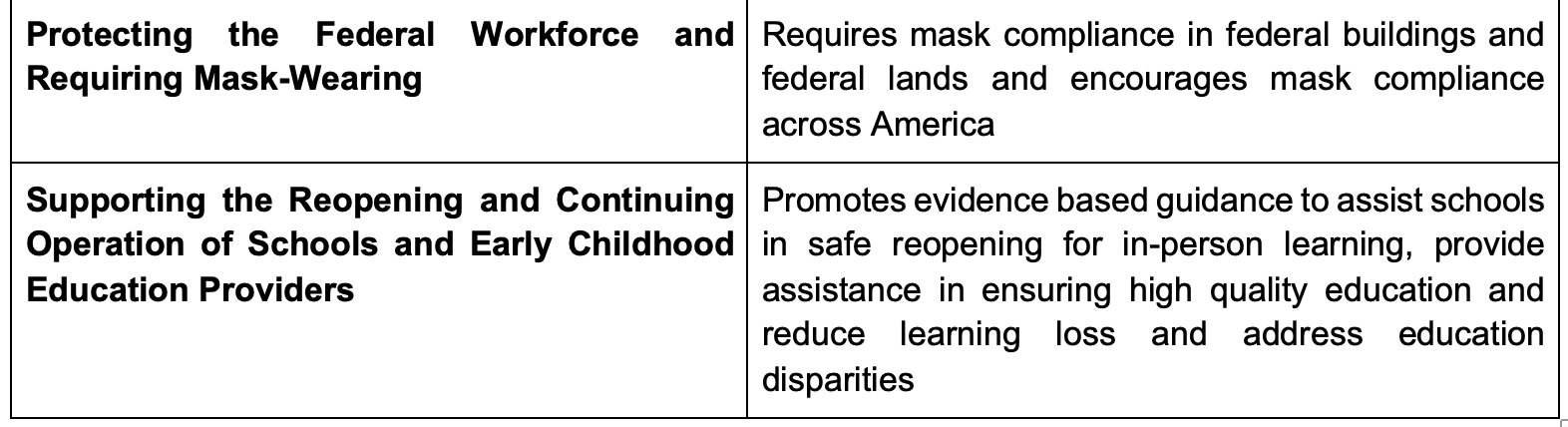
President Biden has also signed several Executive Orders (EO) to combat the COVID-19 pandemic6. Here are the highlights:
Why does this matter?
The COVID-19 pandemic has had a devastating toll on the U.S. with approximately 25.2 million cases and 420,000 deaths to date and an estimated $3.2-4.8 trillion net loss in a 2-year period 7,8. The pandemic has strained health care resources and capacity, which in turn has caused financial losses for both patients, physicians and healthcare institutions8. Additionally, healthcare disparities were brought to the forefront as the pandemic disproportionately affected communities of color and rural and underserved communities7,9,10.
The COVID relief bill and President Biden’s EOs seek to address the pandemic by strengthening public health efforts, expanding public health infrastructure, providing financial resources to physicians and expanding vaccination capacity. The latter will be critical given the need for vaccination coverage and the potential for vaccines to help end the pandemic11. President Biden’s EOs especially seek to bring a robust, equitable response to the COVID-19 to protect our communities by emphasizing metrics and improving coordination in the US government. These EOs also fortify public health infrastructure and take a proactive approach for future pandemics.
Replenishing the Provider Relief Fund and expanding eligibility for the Paycheck Protection Program will mitigate the financial costs to healthcare systems and providers so that they can continue to provide needed health care to our communities2,. Moreover, the Provider Relief Fund clarifies that parent organizations can now transfer provider relief funds to eligible providers in the parent organization’s subsidiaries12. Health care providers now have better guidance on how to calculate lost revenues. These revisions serve to make funds more accessible and will mitigate health care institutions financial costs’ to continue to provide patient care.
The addition of Medicare and Medicaid provisions will further ameliorate the healthcare costs of the pandemic. Specifically, the 3.75% increase in Medicare PFS Payments and the 3-year delay for the CMS G2211 complex E/M patient visits add-on code will positively affect EM reimbursement1,2,3. The PFS conversion factor was originally scheduled for a 10.2% cut under the 2021 Medicare PFS final regulation, however, the increase in PFS payments and delayed implementation of G2211 ultimately yields just a 3.3% reduction in the conversion factor13. Fortunately, increases to the ED E/M code values may actually offset the conversion factor cuts and lead to a net positive reimbursement for ED E/M level 3-5 services or, worse case scenario, a 2% reduction in reimbursement1,2. There will be an expected 9.8% increase for ED E/M level 3, 1.6% for ED E/M level 4 and 2% for ED E/M level 513. Although the 2% cuts from Medicare sequestration are suspended during the COVID pandemic, the cuts are in fact scheduled to go into effect on April 1, 2021, unless new legislation is enacted. The cuts do have the potential to offset the reimbursement gains.
The Medicare and Medicaid provisions also allocate funding for rural communities by offering greater flexibility for rural and urban hospitals to participate in the Medicare GME Rural Training Tracks program, which are designed to promote rural training and ultimately rural practice14. The addition of 1,000 new physician GME slots, preferentially going to rural and underserved areas, comes at a crucial time given that the pandemic strained the health care workforce and rural and underserved areas10. Rural Emergency Hospitals (REH) is a new Medicare reimbursement type that allows eligible Critical Access hospitals and rural hospitals to provide certain emergency department services and observation care without providing inpatient care1,2,15. This also includes higher Medicare reimbursement rates than is typically provided. The exact requirements for operating as an REH and eligibility criteria are yet to be determined. These provisions have the potential to reinforce the physician workforce and increase access to care in rural and underserved areas in the long term.
Surprise Medical Billing was, and remains, a highly contested policy issue that is finally addressed in some form. Starting in 2022, patients will be protected against balance-billing unexpected bills from out of network providers providing care at in-network facilities and air ambulance costs2,3,4. However, ground ambulance transportation costs are not included in the legislation.
Under the new terms, out of network deductibles will be the same as the in-network terms of the patient’s insurance plan. Physicians will no longer be able to balance bill patients beyond the in-network costs. Instead, insurers are required to either provide reimbursement or issue a denial within 30 days of services provided. The insurer’s payment is subject to state laws and policies, thus the Surprise Medical Billing terms only apply to federally regulated plans if there are already state mandated surprise billing laws2.
Physicians then have 30 days to negotiate the payment (if they’re not satisfied) and settle with insurers1,2. If a negotiation cannot be reached, then the insurer or provider can enter an IDR process within 4 days of the conclusion of the negotiation period. The IDR is conducted through an arbiter approved by the federal government2. The arbiter will consider multiple factors, such as median in-network rates, complexity of care, provider’s experience, etc. Fortunately, there is no minimum threshold to initiate an IDR process and similar claims may be submitted in batches. This IDR process will be completed within 30 days, and thereafter, the losing party will be responsible for the fees to participate in the IDR.
Despite these anticipated changes, there is some flexibility for patients to consent to entering into balance billing with out-of-network physicians if they seek treatment from out-of-network physicians. Regardless, physicians are required to provide “good faith” cost estimates of services provided. Insurers are also obligated to increase transparency by providing patients with the policy out-of-network and in-network deductibles, an updated in-network provider directory and an Advanced Explanation of Benefits of the costs charged and paid by stakeholders (policyholder, insurer, provider)2.
What can I do about it?
Become familiar with the COVID Relief Bill
Determine eligibility for the Provider Relief Fund and Paycheck Protection Program
Determine eligibility to convert to a Rural Emergency Hospital
Determine whether your institution’s residency program qualifies for new GME slots
Prepare a system and protocol to enter IDR with insurers
Helpful resources and links
Summary of Emergency Medicine-related Provisions in 2020 Year-end Congressional Package
CARES Act Provider Relief Fund: General Information
Johns Hopkins Coronavirus Resource Center
This post was a collaboration between emDocs and the EMRA Health Policy Committee.

References:
- Summary of Emergency Medicine-related Provisions in 2020 Year-end Congressional Package. American College of Emergency Physicians. December 31, 2021. Accessed January 24, 2021. https://www.acep.org/globalassets/new-pdfs/advocacy/2020-omnibus-acep-detailed-summary.pdf
- Detailed Summary of Health Provisions in Consolidated Appropriations Act, 2021. American Hospital Association. December 22, 2020. Accessed January 24, 2021. https://www.aha.org/system/files/media/file/2020/12/detailed-summary-health-provisions-consolidated-appropriations-act-2021-bulletin-12-22-20.pdf
- AAMC Statement on the Consolidated Appropriations Act, 2021. Association of American Medical Colleges. December 22, 2020. Accessed January 1, 2021. https://www.aamc.org/news-insights/press-releases/aamc-statement-consolidated-appropriations-act-2021
- Appleby J. Congress acts to spare consumers from costly surprise medical bills. National Public Radio. December 22, 2020. Accessed January 24, 2021. https://www.npr.org/sections/health-shots/2020/12/22/949047358/congress-acts-to-spare-consumers-from-costly-surprise-medical-bills
- National Strategy for the COVID-19 Response and Pandemic Preparedness. The White House. January 21, 2021. Accessed January 24,2021. https://www.whitehouse.gov/wp-content/uploads/2021/01/National-Strategy-for-the-COVID-19-Response-and-Pandemic-Preparedness.pdf
- Federal Register. Executive Office of the President. Accessed February 5, 2021. https://www.federalregister.gov/agencies/executive-office-of-the-president#documents
- Johns Hopkins Coronavirus Resource Center. Johns Hopkins University. January 25, 2021. Accessed January 25, 2021. https://coronavirus.jhu.edu/
- Walmsley T, Rose A, Wei D. The Impacts of the Coronavirus on the Economy of the United States. Econ Disaster Clim Chang. 2020. doi:10.1007/s41885-020-00080-1
- Health Equity Considerations and Racial and Ethnic Minority Groups. Centers for Disease Control and Prevention. July 24, 2020. Accessed January 24, 2021. https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html
- Mueller J, McConnell K, Burow P, Pofahl K, Merdjanoff A, Farrell J. Impacts of the COVID-19 pandemic on rural America. Proceedings of the National Academy of Sciences. 2020;118(1):2019378118. doi:10.1073/pnas.2019378118
- Dolgin E. COVID-19 vaccines poised for launch, but impact on pandemic unclear. Nature. November 30, 2020. Accessed January 24, 2021. https://www.nature.com/articles/d41587-020-00022-y
- Department of Health and Human Services. CARES Act Provider Relief Fund: General Information. January 21, 2021. Accessed January 24, 2021. https://www.hhs.gov/coronavirus/cares-act-provider-relief-fund/general-information/index.html
- Davis J. Major Crisis Averted(for Now): Rather than Medicare Payment Reductions, a Raise May be Coming Your Way in 2021. American College of Emergency Physicians. January 7, 2021. Accessed February 5, 2021.
- Rural Training Track Programs: A guide to the Medicare Requirements, Association of American Medical Colleges. 2017. Accessed January 24, 2021. https://store.aamc.org/downloadable/download/sample/sample_id/204/
- Cook EJ, DiVarco SM. Congress Established New Medicare Provider Category and Reimbursement for Rural Emergency Hospitals. The National Law Review. January 5, 2021. Accessed February 5, 2021. https://www.natlawreview.com/article/congress-establishes-new-medicare-provider-category-and-reimbursement-rural




