
Originally published at R.E.B.E.L. EM on July 13, 2017. Reposted with permission.
Follow Salim R. Rezaie at @srrezaie, and Dr. Anand Swaminathan at @EMSwami.
 Intro: Vasoactive substances are powerful therapeutic medications that can boost a patient’s blood pressure and perfusion to target organs. They are often used in resuscitation to support tissue perfusion though their benefits are mostly unproven and may be harmful in certain circumstances (i.e. hypovolemia, hemorrhage). The cognitive response to hypotension should not be reaching for a pressor. The primary therapy for any sick hypotensive patient is treatment of the underlying pathology.
Intro: Vasoactive substances are powerful therapeutic medications that can boost a patient’s blood pressure and perfusion to target organs. They are often used in resuscitation to support tissue perfusion though their benefits are mostly unproven and may be harmful in certain circumstances (i.e. hypovolemia, hemorrhage). The cognitive response to hypotension should not be reaching for a pressor. The primary therapy for any sick hypotensive patient is treatment of the underlying pathology.
While many patients will respond to these medications, we occasionally encounter non-responder-patients who despite substantial doses do not show hemodynamic parameter improvements. Absence of response can result from a number of causes including misidentification of the underlying pathology (i.e. I missed the massive PE or pericardial tamponade thinking the patient was in septic shock). Premature diagnostic closure can lead us to simply push on with higher doses of pressors and adding additional pressors. However, there should be a cognitive pause at this point where the clinician reassesses the situation, considers alternate causes and therapeutics. Below is a list of pathologic conditions that complicate other diagnoses and are frequently missed as causes of non-response to vasopressors. This is the list I consider during my cognitive pause.
Acidosis
- Diagnostic: Blood gas, basic metabolic panel
- Therapeutic
- Reverse underlying cause if possible.
- Sodium bicarbonate is unlikely to be helpful thought it may be used as a drip as a bridge to continuous veno-venous hemodialysis (CVVHD)
- CVVHD may be an option
Hypothyroidism
- Diagnostic
- Clinical diagnosis
- TSH with T3/T4 reflex
- Results often delayed
- May be false negative in acute decompensation
- Therapeutic: Levothyroxine (may need to give empirically if labs delayed)
Anaphylaxis
- Can present as hypotension alone
- Diagnostic: History
- Therapeutic: Epinephrine, Methylene blue, ECMO (in refractory cases)
Adrenal Insufficiency/Failure
- Diagnostic
- Clinical
- Depressed cortisol level
- Hyperkalemia with hyponatremia
- Therapeutic
- Stress dose steroids (hydrocortisone 100-200 mg IV)
- Empiric treatment often necessary
Hypocalcemia
- Diagnostic
- Ionized serum calcium (iCa2+)
- Prolonged QTc interval
- Therapeutic: Calcium salts (CaCl or CaGluconate)
Occult or Ongoing Blood Loss
- Occult Sources: GI Hemorrhage, Retroperitoneal bleed
- Therapeutic
- Operative or interventional control if source amenable
- Reverse anticoagulation if relevant,
- Transfuse to buy time to locate bleeding
Toxicologic
- Occult causes: Beta blocker overdose, calcium channel blocker overdose, TCA overdose
- Therapeutic: Hyperinsulinemia Euglycemia Therapy (HIET), ECMO, bicarbonate (for TCA overdose)
Second Cause of Shock
- Patients can have multiple concurrent causes of shock (Hickum’s dictum)
- Make sure to search for a secondary cause of shock
- Rapid Ultrasound for Shock and Hypotension (RUSH) protocol extremely useful when considering multiple causes of shock
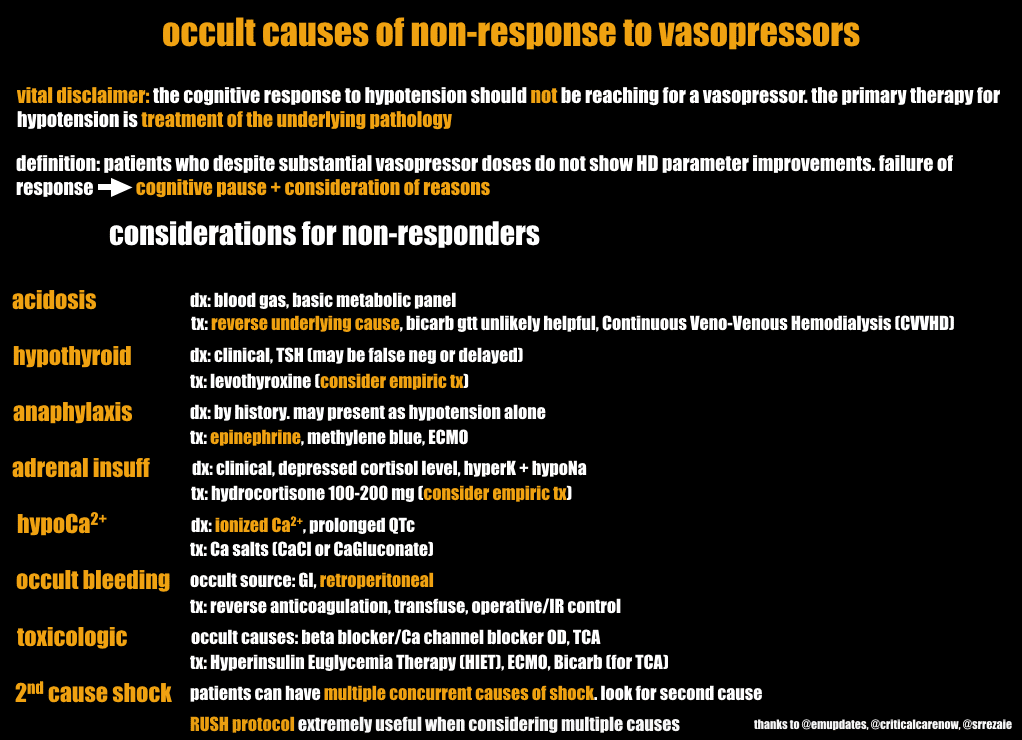
Thank you to Reuben Strayer (Twitter: @emupdates), Haney Mallemat (Twitter: @CriticalCareNow) and Salim Rezaie (Twitter: @srrezaie) for helping develop this post.
Read More:
- EM Updates: Hypotension: Differential Diagnosis
- EMCrit: RUSH Exam
- EMCrit: Podcast 87 – Mind of the Resuscitationist: Stop Points





2 thoughts on “R.E.B.E.L. EM – Occult Causes of Non-Response to Vasopressors”
Great post! I would add:
– hypothermia
– tox: digoxin, alpha2 agonists (clonidine, guanfacine); treatment for BB/CCB – glucagon as well
Really helpful! ! Thanks