
Authors: Evelyn Huang, MD (@EvelynHuangMD, EM Resident Physician, Northwestern University, Chicago, Illinois) and Kelly Williamson, MD (Assistant Program Director, Associate Professor, Northwestern University, Chicago, Illinois) // Reviewed by: Arianne Chavez-Frazier, MD (Dermatologist and Mohs Surgeon, Dermatology SouthEast, St. Johns, FL); Summer Chavez, DO, MPH, MPM, (UT Houston); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)
Case
A 75-year-old male with a past medical history of hypertension, hyperlipidemia, and type 2 diabetes mellitus is brought in by his daughter for headache and weakness on his left side. He states that his symptoms have been slowly progressive. He is having a hard time walking because of leg weakness. The patient states he has been dropping items from his left hand. He has had persistent headaches for the past 2 weeks. They seem to be worse in the mornings and are only slightly relieved by Tylenol. He has not fallen or hit his head. He presented to the ED today because his headache was much worse this morning. On exam, the patient is not in acute distress. He has 4/5 weakness in his left arm and leg with slightly decreased sensation. CN II-XII are intact. As you palpate his head for any deformity, you notice this lesion behind his left ear:
What is on your differential? What is your next step?
Skin conditions are incredibly common. In 2013, 1 in 4 Americans (85 million people) were seen by a physician for at least one skin disease. This led to a healthcare cost of $75 billion [1]. Approximately 3.3% of ED visits are for skin conditions [2]. Since the emergency department may be the only interaction that a patient has with the healthcare system, it is essential that emergency physicians are able to recognize and manage skin cancers.
History Questions
Important questions to ask your patient if you notice a suspicious lesion concerning for skin cancer:
-Personal or family history of skin cancer?
-Use of tanning beds, excessive sun exposure, or sunburns?
-Chronicity of changes to lesion?
-Immunosuppressed?
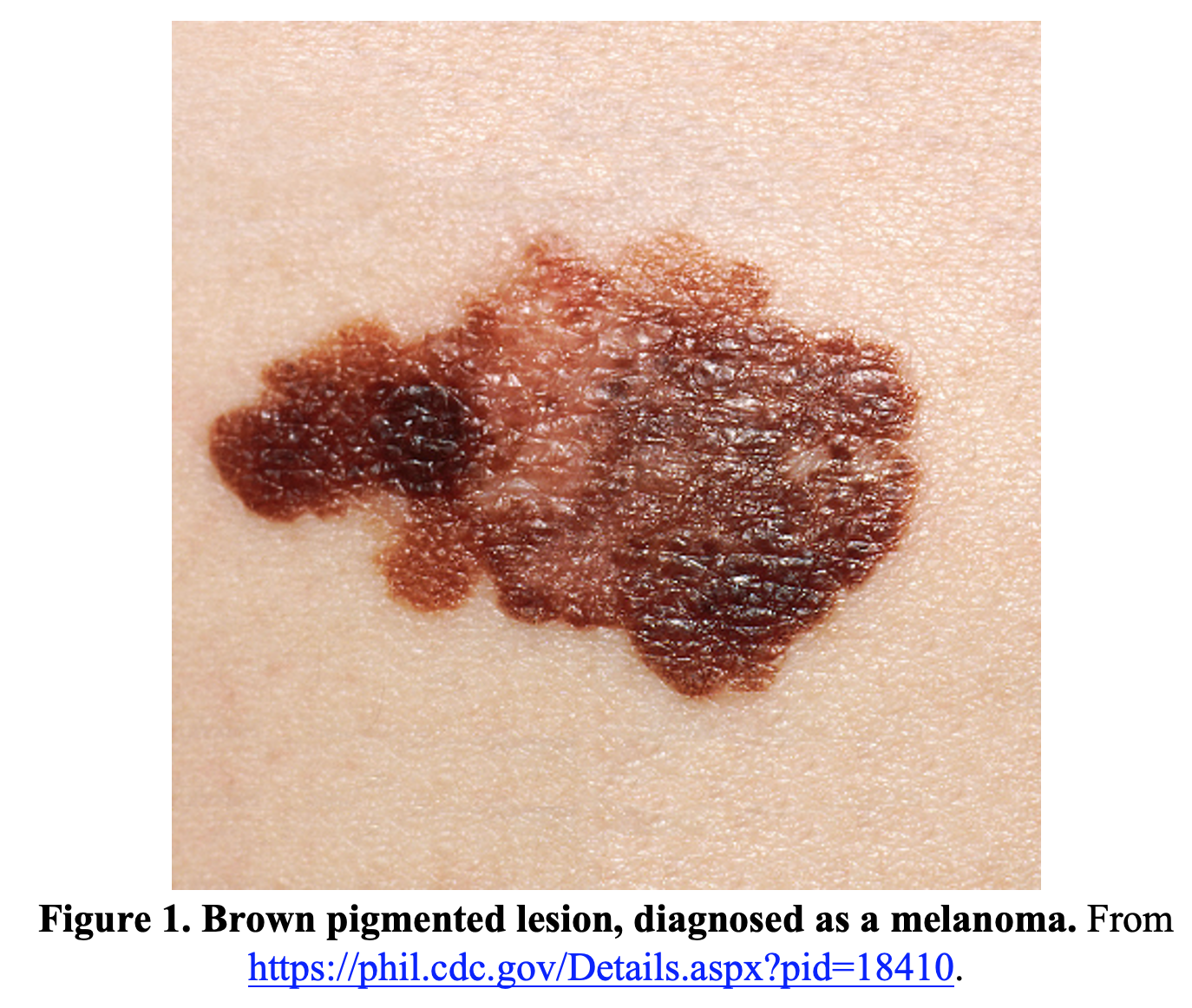
Melanoma
Melanoma is the most concerning skin cancer and the 5th most common cancer in the United States [3]. There are three clinical prediction rules to use when evaluating a possible melanoma: ABCDE criteria, the “ugly duckling” sign, and the Glasgow checklist.
- ABCDE [4]: Asymmetry, Border irregularity, Color variation, Diameter >6 mm, Evolving
- “Ugly duckling” sign [5]: helpful in patients with multiple nevi, the ugly duckling sign is a nevus that looks different from all the others
- Glasgow seven-point checklist [6]: One major and at least three minor features warrant a referral
- Major features
- Change in size of lesion
- Irregular pigmentation
- Irregular border
- Minor features
- Inflammation
- Itch or altered sensation
- Larger than other lesions (diameter >7mm)
- Oozing/crusting of lesion
- Major features
While all of these clinical prediction rules have varying sensitivities and specificities, it is prudent to incorporate them all into your decision-making process when determining whether a patient needs a referral [4-6]. Since all of this information is based on the history and visual examination of the lesion, no extra time is needed to add these prediction rules to your practice.
It is also important to consider different presentations of melanoma.
- Subungual melanomas (melanoma of the nail unit) [7]: An updated rule of ABCDEF can help to help detect subungual melanoma
- A: Age (5th-7th decade of lie), African American, Asian, Native American
- B: Brown or Black band with Breadth of >3 mm
- C: Change in nail band
- D: Digit most commonly involved (thumb and great toe)
- E: Extension of pigment onto nailfold (Hutchinson’s sign)
- F: Family or personal history

- Melanoma in children: evolution of nevi and new nevi can be normal in children, which means that the E for evolution criteria may not be useful. A new ABCD criteria in addition to the traditional ABCDE criteria for children has been suggested [8]:
- A: Amelanotic
- B: Bleeding, Bump
- C: Color uniformity
- D: De novo, any Diameter
- Nodular melanoma: lesions that are pink or have no pigmentation, which can lead to delays in diagnosis. These lesions are often symmetric, uniform in color, and elevated [9].
It is critical to remember that melanomas can metastasize, with the most common site of regional metastasis being the surrounding skin/tissue and lymph nodes [10]. The most common sites of distant metastases are the skin, lung, brain, liver, bone, and intestine [10]. Lung metastases are often the first clinically detected, with bone and intestine occurring later in the disease process [10].
When diagnosed at an early stage, surgical excision can be curative [10]. When melanoma is suspected and the patient is determined to be stable to go home, the most important step for the emergency physician is to refer the patient for urgent follow-up with a dermatologist to facilitate biopsy of the lesion [10].
Basal Cell Carcinoma
Basal cell carcinoma (BCC) is the most common type of skin cancer [11]. While it does have a low metastatic potential, BCC can be locally aggressive and cosmetically destructive [11].
BCC commonly develops on the sun and UV exposed parts of the body, such as the face and trunk [11]. Nodular BCC is typically a pearly pink or flesh-colored papule [11]. They may be associated with telangiectasias and rolled border where the sides are raised higher than the center of the lesion [11]. These lesions can also ulcerate or bleed [11].

Superficial BCC is more commonly found in younger adults. These lesions present as scaly macules or plaques with irregular or rolled borders [11].

Diagnosis for BCC is confirmed with biopsy and complete excision is curative [11]. Other treatments include cryotherapy, photodynamic therapy, radiotherapy, imiquimod cream, and fluorouracil cream [11]. It is important to refer the patients that you suspect have BCC to dermatology to have these lesions evaluated and either removed or treated [11].
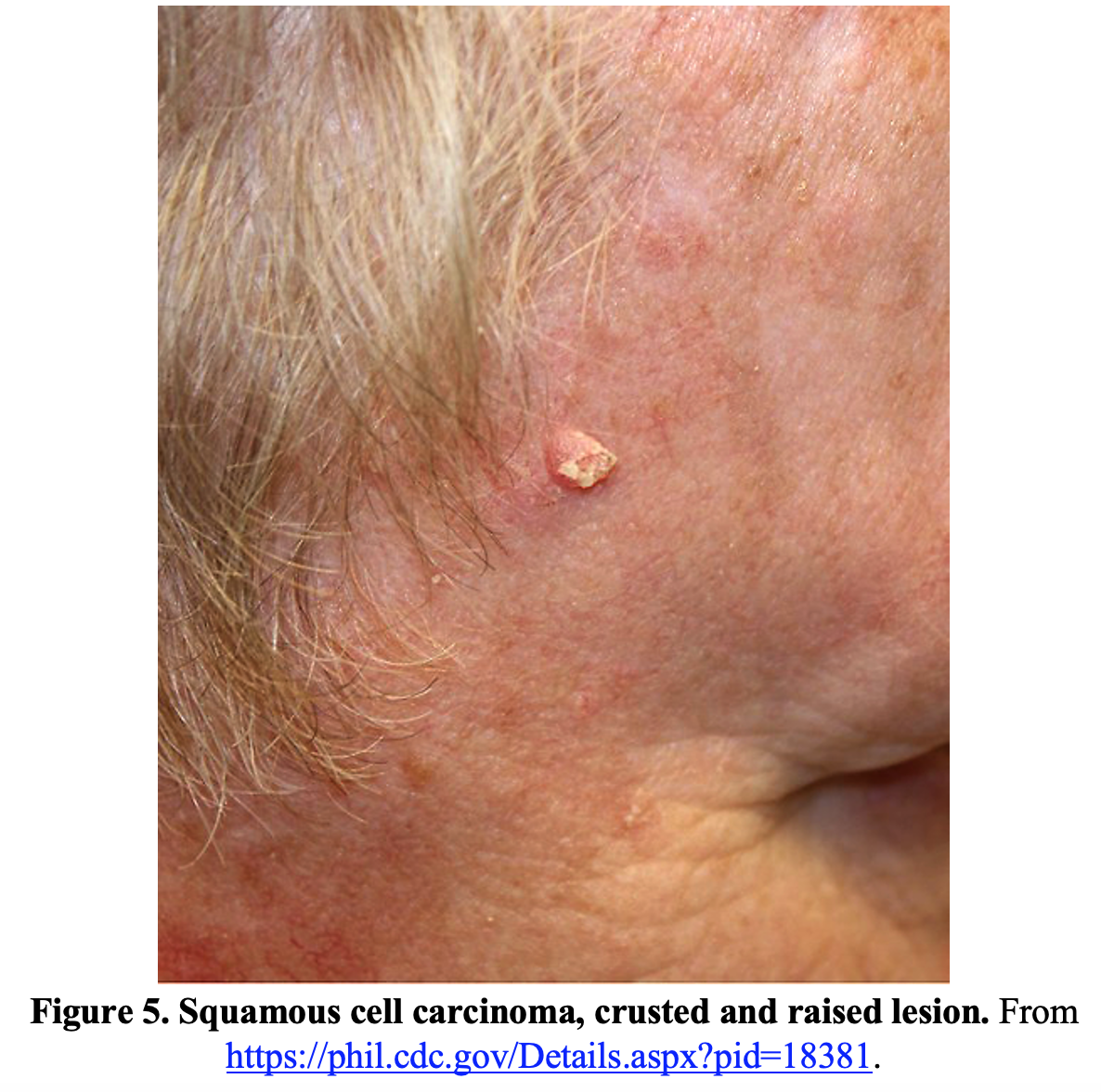
Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) is composed of keratinocytes and commonly occur in sun exposed areas of fair-skinned patients [12]. In darker-skinned patients, SCC commonly occurs in non-sun-exposed areas such as scars, lower legs, and the genital region [12].
Cutaneous SCC often appears as a scaly or crusted lesion that grows over time and may ulcerate or become painful [13]. Actinic keratosis, which often appears as a scaly plaque, is a precursor lesion to SCC [13].

Concerning features for SCC lesions with a high risk of recurrence and metastasis include lesions that are greater than 2 cm, those in the elderly or immunocompromised patients, and those located on the face, lip, hands, feet, or genitalia [13].
Similar to the other skin cancers, diagnosis is confirmed with biopsy [13]. High risk patients may need staging to determine whether there is spread to lymph nodes. Treatment includes excision, cryotherapy, radiotherapy, or immune-modulators [13].
Merkel Cell Carcinoma
Merkel cell carcinoma is a rare and highly aggressive skin cancer with a mortality of approximately 33% at 3 years. Consider using the AEIOU Criteria [14]:
- A: Asymptomatic/lack of tenderness
- E: Expanding
- I: Immune suppression
- O: Older than 50 years old
- U: Ultraviolet exposed site on a person with fair skin
This cancer is rare, with approximately 0.7 cases per 100,000 people in the United States in 2013 [15]. However, with the advancing age of the population, the prevalence may continue to grow. Lesions are typically irregular red nodules that are solitary and grow rapidly [16]. The lesions may appear similar to BCC but grow at a much faster rate [16].
Treatment includes excision with or without radiotherapy [16]. Lymph nodes may also be removed or irradiated. Metastatic Merkel cell carcinoma may also be treated with chemotherapy [16]. As with all the skin cancers, follow-up with dermatology for biopsy and treatment is essential [16].
Case Resolution
Due to the patient’s new focal neurologic deficits and skin lesion concerning for melanoma, CT imaging of the brain was ordered. The scan was concerning for metastasis to the brain. In the setting of the new brain mass and persistent falls at home, the patient was admitted to the hospital for further evaluation by the neurosurgery service, physical therapy and occupational therapy.
Conclusion and Take-Home Points
In the emergency department, you will see many skin lesions that may or may not relate to the patient’s presenting complaint. As seen in the presenting case of melanoma with metastasis to the brain, a thorough skin exam may even help with the diagnosis. Since the emergency department may be the only interaction that a patient has with the healthcare system, it is incredibly important to offer referrals and consultations when discovering lesions concerning for skin cancer. Do not forget to risk stratify your patients by asking pertinent history questions such as sun/UV exposure, family history, and immunosuppression.
References/Further Reading:
- Lim HW, Collins SAB, Resneck JS Jr, et al. The burden of skin disease in the United States. J Am Acad Dermatol. 2017;76(5):958-972.e2. doi:10.1016/j.jaad.2016.12.043
- Nadkarni A, Domeisen N, Hill D, Feldman SR. The most common dermatology diagnoses in the emergency department. J Am Acad Dermatol. 2016;75(6):1261-1262. doi:10.1016/j.jaad.2016.07.054
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7-34. doi:10.3322/caac.21551
- Abbasi NR, Shaw HM, Rigel DS, et al. Early Diagnosis of Cutaneous Melanoma: Revisiting the ABCD Criteria. 2004;292(22):2771–2776. doi:10.1001/jama.292.22.2771
- Grob JJ, Bonerandi JJ. The ‘ugly duckling’ sign: identification of the common characteristics of nevi in an individual as a basis for melanoma screening. Arch Dermatol. 1998;134(1):103-104. doi:10.1001/archderm.134.1.103-a
- Healsmith MF, Bourke JF, Osborne JE, Graham-Brown RA. An evaluation of the revised seven-point checklist for the early diagnosis of cutaneous malignant melanoma. Br J Dermatol. 1994;130(1):48-50. doi:10.1111/j.1365-2133.1994.tb06881.x
- Levit EK, Kagen MH, Scher RK, Grossman M, Altman E. The ABC rule for clinical detection of subungual melanoma. J Am Acad Dermatol. 2000;42(2 Pt 1):269-274. doi:10.1016/S0190-9622(00)90137-3
- Cordoro KM, Gupta D, Frieden IJ, McCalmont T, Kashani-Sabet M. Pediatric melanoma: results of a large cohort study and proposal for modified ABCD detection criteria for children. J Am Acad Dermatol. 2013;68(6):913-925. doi:10.1016/j.jaad.2012.12.953
- Chamberlain AJ, Fritschi L, Kelly JW. Nodular melanoma: patients’ perceptions of presenting features and implications for earlier detection. J Am Acad Dermatol. 2003;48(5):694-701. doi:10.1067/mjd.2003.216
- Damsky WE, Rosenbaum LE, Bosenberg M. Decoding melanoma metastasis. Cancers (Basel). 2010;3(1):126-163. Published 2010 Dec 30. doi:10.3390/cancers3010126
- Oakley A. Basal cell carcinoma. DermNet NZ. https://dermnetnz.org/topics/basal-cell-carcinoma/. Published 2015. Accessed August 29, 2020.
- Mora RG, Perniciaro C. Cancer of the skin in blacks. I. A review of 163 black patients with cutaneous squamous cell carcinoma. J Am Acad Dermatol. 1981;5(5):535-543. doi:10.1016/s0190-9622(81)70113-0
- Oakley A. Cutaneous squamous cell carcinoma. DermNet NZ. https://dermnetnz.org/topics/cutaneous-squamous-cell-carcinoma/. Published 2015. Accessed August 29, 2020.
- Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58(3):375-381. doi:10.1016/j.jaad.2007.11.020
- Paulson KG, Park SY, Vandeven NA, et al. Merkel cell carcinoma: Current US incidence and projected increases based on changing demographics. J Am Acad Dermatol. 2018;78(3):457-463.e2. doi:10.1016/j.jaad.2017.10.028
- Ludgate M, Oakley A. Merkel cell carcinoma. DermNet NZ. https://dermnetnz.org/topics/merkel-cell-carcinoma/. Published 2014. Accessed August 29, 2020.




