
Author: Erica Simon, DO, MHA (@E_M_Simon, EM Chief Resident at SAUSHEC, USAF) // Edited by: Jennifer Robertson, MD, MSEd and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Case 1:
A nine month-old female presents to the emergency department (ED) with an increased work of breathing. The patient’s mother states that she developed a cough three days prior. Her past medical history is unremarkable and the patient’s immunizations are up to date.
Initial vital signs (VS) in the ED: Heart rate (HR) 166 beats per minute (bpm), respiratory rate (RR) 42/minute (min), Oxygen saturation 96% on room air (RA), Temperature (T) of 103.1° Fahrenheit (F). As you walk into the room, you note the patient exhibiting generalized tonic-clonic motions, which resolve approximately one minute after onset. After rechecking the patient’s airway, breathing and circulation (ABCs), you verify that the patient is stable and you quickly move on to the next patient.
Case 2:
The nurse is triaging a well-appearing three week-old infant. The baby’s VS are within normal limits. However, the nurse pulls you aside to express her concern regarding the patient’s repetitive tongue movements and directional eye motions she witnessed prior to your arrival.
If you are scanning your memory bank for information regarding the evaluation and treatment of these pediatric seizures, look no further. This post will discuss the epidemiology of pediatric seizures, and offer a review of the evaluation and treatment of seizures occurring within the first year of life.
Epidemiology of Pediatric Seizures
Seizures are the most common neurologic emergency of childhood, representing approximately 1.5% of pediatric emergency department (ED) visits annually.1-3 Each year, nearly 150,000 children in the United States experience new onset seizure activity and an estimated 25,000 to 40,000 of these are afebrile. In addition, up to 10% of these patients suffer from status epilepticus.1-5 Among individuals with unprovoked afebrile seizures, approximately 70% are idiopathic and nearly 88% experience a recurrence within two years of the initial event.5
Evaluation & Treatment
In all patients presenting with a chief complaint of seizure, a comprehensive history and physical examination should be performed. The patient history should center on events immediately prior to seizure onset (cyanosis, LOC), length of the seizure, a description of seizure activity, the presence of bowel or bladder incontinence, evidence of a postictal period, and the presence or absence of a family history of seizure disorder.
Important historical information should be obtained in patients under the age of one year. This includes birth history (pre-term/term, maternal infection), immunizations, change in diet or formula (change in preparation), any time spent unsupervised (accidental ingestions), and home remedies or medications utilized to treat maladies.1,2,5
If the patient has a known seizure disorder, details should be obtained regarding seizure frequency, any alterations in medication regimens such as missed doses, and changes in seizure pattern (s).5,6
Physical examination in infants should focus on:
Neurologic: developmental stages appropriate for age (milestones: 2 months = social smile, coos, tracks faces; 4 months = babbles, reaches for toy, holds head unsupported, etc)7
HEENT: head circumference, bulging or sunken fontanelles, retinal hemorrhages (may indicate increased intracranial pressure (ICP) +/- non-accidental trauma (NAT) versus volume depletion
Cardiac: capillary refill >2 seconds (sec)
Abdominal: hepatosplenomegaly => metabolic derangement/glycogen storage disease
Integumentary: café-au-lait spots => neurofibromatosis; vitiliginous lesions => tuberous sclerosis; port-wine stains => Sturge-Weber Syndrome; excessive bruising => NAT5
The evaluation and treatment of pediatric seizures within the first year of life varies according to seizure classification.
Febrile Seizures
The American Academy of Pediatrics defines a febrile seizure as seizure activity associated with a temperature ≥ 100.4 °F or 38 °C, occurring in patients 6 through 60 months of age, in the absence of central nervous system (CNS) infection, metabolic abnormalities or a history of afebrile seizure.1-4 The incidence of simple febrile seizures peaks at 18 months of age.1
Risk Factors for Febrile Seizures
While the pathophysiology of seizures occurring in the setting of elevated core temperatures is poorly understood, several risk factors have been identified:
- Family history of febrile seizures (no susceptibility gene identified, but family history reported in 25-40% of patients).1,8
- Viral infections: human herpes virus (HHV) 6 and influenza.1,8
- Vaccinations: diphtheria, tetanus toxoids, and whole cell pertussis (DTP), and measles, mumps, and rubella (MMR)1,8
To help aid in physician decision-making regarding the need for diagnostic testing and treatment, febrile seizures are identified as simple versus complex.
Table 1 summarizes the characteristics of simple and complex seizures.
| Seizure Type | ||
| Simple | Complex | |
| Duration | < 15 minutes | ≥15 minutes |
| Motion | Generalized, Tonic-Clonic | Focal |
| Mental Status | Return to baseline | Persistent alteration in mental status |
| Episodes | 1 episode within 24 hours | > 1 episode within 24 hours |
Neonatal seizures can be subtle and difficult to detect. Generalized tonic-clonic and myoclonic activity is rarely seen in patients of this age group given their premature central nervous systems.1 Much more commonly, patients under 28 days of age present with motor automatisms (ocular deviations, repetitive limb movements, repetitive oral movements) or changes in heart rate, and/or respiratory rate (apneic episodes).6
Evaluation and Treatment of Simple Febrile Seizures
In 2011, the American Academy of Pediatrics (AAP) released an updated guideline for the management of simple febrile seizures. In the setting of a simple febrile seizure, the AAP recommends the following:10
- A lumbar puncture (LP) should be performed in pediatric patients presenting with meningeal signs or in any child whose history and/or examination suggest meningitis or intracranial infection (Level B recommendation based on overwhelming evidence from observational studies).
- In infants 6-12 months of age who presents with a seizure and fever, a LP is an option when the child is deficient in Haemophilus influenza type b (Hib) or Streptococcus pneumoniae immunizations, or when immunization status is unknown (Level D recommendation that is based on expert opinion and case reports).
- A LP is an option in a pediatric patient pre-treated with antibiotics, as antibiotics may mask signs and symptoms of meningitis (Level D recommendation based on expert opinion and case reports).
- An electroencephalogram (EEG) should not be performed in a neurologically healthy child with a simple febrile seizure (Level B recommendation based on overwhelming evidence from observational studies).
- Routine laboratory studies should not be routinely performed for the sole purpose of identifying the cause of a simple febrile seizure (Level B recommendation based on overwhelming evidence from observational studies).
- Neuroimaging should not be performed in the setting of a simple febrile seizure (Level B recommendation based on overwhelming evidence from observational studies).
Note: The AAP’s recommendations are based on an academic review of literature published from 1996-2009. Perhaps the most commonly cited studies include:
Green SM, Rothrock SG, Clem KJ, Zurcher RF, Mellick L. Can seizures be the sole manifestation of meningitis in febrile children? Pediatrics. 1993;92(4):527–534.
This is a retrospective review of 503 consecutive cases of meningitis in pediatric patients aged 2 months to 15 years seen at two referral hospitals over a 20 year period. None of the 503 patients noted to have meningitis manifested with seizure as a sole symptom.
Kimia AA, Capraro AJ, Hummel D, Johnston P, Harper MB. Utility of lumbar puncture for first simple febrile seizure among children 6 to 18 months of age. Pediatrics. 2009;123(1):6–12.
- Retrospective cohort review of patients aged 6 to 18 months who were evaluated for first simple febrile seizure in a pediatric emergency department between October 1995 and October 2006: no patient was diagnosed as having bacterial meningitis (number undergoing LP: 360)
Ultimately, evaluation of a febrile patient experiencing a simple febrile seizure should focus on identifying the underlying etiology of the fever. Laboratory studies and imaging should be ordered at physician discretion and according to institutional policy. Please review the Philadelphia, Rochester, & Boston criteria for further information on how to identify febrile infants who are at risk for serious bacterial infections. Despite thorough evaluation, approximately 30% of patients experiencing a simple febrile seizure will leave the ED without an identified etiology.11
Evaluation of Complex Febrile Seizures
Given the heterogeneity of patient presentations and relatively little knowledge regarding their etiologies, no standard algorithm or clinical practice guideline exist for the evaluation and management of complex febrile seizures.1,4
However, a recent retrospective, cohort review by Kimia et al. did present data on this patient population:
- From 1995 to 2008, 526 pediatric ED patients aged 6 to 60 months (median age 17 months) were evaluated for a first complex febrile seizure. Of the 526 patients, 340 underwent LP. Ultimately, 3 patients were discovered to have acute bacterial meningitis (0.5% of patients experiencing a complex febrile seizure). An additional patient was hospitalized and treated with antibiotics based upon a positive blood culture result.
In terms of complex febrile seizures, further studies are warranted. Determining the need for neuroimaging, lumbar puncture, laboratory studies, and EEG must be determined on a case-by-case basis.4 CT can be considered if there is a concern for increased ICP or a mass, while MRI may demonstrate hippocampal injury or temporal sclerosis in the setting of febrile seizures. A neurology consultation and admission are likely in the best interest of any of these patients.
Afebrile Seizures
The differential diagnosis for new onset afebrile seizures within the first year of life is broad (Table 2). The emergency physician primarily plays a role in stabilizing patients and in initiating preliminary evaluation.
| Etiologies of New-Onset Afebrile Seizures | ||
| Time of Onset | ||
| 24 Hours | Direct Drug Effects | Intraventricular Hemorrhage |
| Hypoxic-ischemic Encephalopathy | Laceration of Tentorium or Falx | |
| Intrauterine Infection | Pyridoxine Dependency | |
| Subarachnoid Hemorrhage (SAH) | ||
| 24-72 Hours | Cerebral Contusion/Subdural | Glycogen Synthase Deficiency |
| Cerebral Dysgenesis | Glycine Encephalopathy | |
| Cerebral Infarction | Pyridoxine Dependency | |
| Drug Withdrawal | SAH | |
| Hypoparathyroidism | Tuberous Sclerosis | |
| Intracranial Hemorrhage (ICH) | Urea-cycle Disturbances | |
| Intraventricular Hemorrhage | Electrolyte Disturbances | |
| 72 Hours – 1 Week | Familial Neonatal Seizures | Kernicterus |
| Cerebral Dysgenesis | Methylmalonic Acidemia | |
| Cerebral Infarction | Nutritional Hypocalcemia | |
| Hypoparathyroidism | Propionic Acidemia | |
| ICH | Tuberous Sclerosis | |
| Urea-cycle Disturbances | Electrolyte Disturbances | |
| > 1 Week | Adrenoleukodystrophy | Gm1 Gangliosidosis Type 1 |
| Cerebral Dysgenesis | HSV Encephalitis | |
| Fructose Dysmetabolism | Ketotic Hyperglycinemias | |
| Gaucher Type 2 | Maple Syrup Urine Disease | |
| Tuberous Sclerosis | Urea-cycle Disturbances | |
| Electrolyte Disturbances | ||
New-Onset Neonatal Afebrile Seizures5,6
Based upon patient presentation and a comprehensive history and physical examination, the following laboratory studies/imaging may or may not be warranted:6
- Inborn errors of metabolism: accucheck, ammonia levels, serum organic acids, urine organic acids, metabolic panel, lactate, pyruvate
- NAT/cerebral anomalies: Cerebral US vs. CT vs. MRI, skeletal survey
- Meningitis/meningoencephalitis: LP
- Toxic ingestions: serum heavy metal screen, serum toxicology levels
It is important to note that experts recommend emergent neuroimaging in the following patient populations:13,14
- Patients with a prolonged seizure (> 15 minutes)
- Focal seizure in patients < 33 months
- Patients with a persistent postictal focal deficit
- Patients with alterations in baseline mental status post seizure activity
- Patients with conditions pre-disposing to intracranial pathology (sickle cell, bleeding diathesis, neurocutaneous disorder, HIV, hydrocephalus, VP shunt, or closed head injury)
Ultimately, the decision between outpatient and inpatient evaluation should be based upon the clinical scenario and in consultation with a neurologist. In general, stable, well-appearing children who have experienced a first unprovoked seizure and are in the low risk category (not requiring emergent neuroimaging as detailed above), may undergo outpatient evaluation if expedited follow-up for EEG is arranged.1,5
All patients experiencing a new-onset afebrile seizure should undergo EEG evaluation as soon as possible because EEG abnormalities may predict seizure recurrence.5 Overall, the recurrent seizure rate in this group is 54% and the majority of seizures recur within two years of the initial event.1 Patients with developmental delays or those with an abnormal EEG are more likely to eventually develop an epileptiform disorder.15
Seizure Treatment
Addressing the patient’s airway and providing benzodiazepines are the mainstays of ED management. The authors Abend and Loddenkemper provide an excellent example of a protocol created for the management of pediatric seizures:16
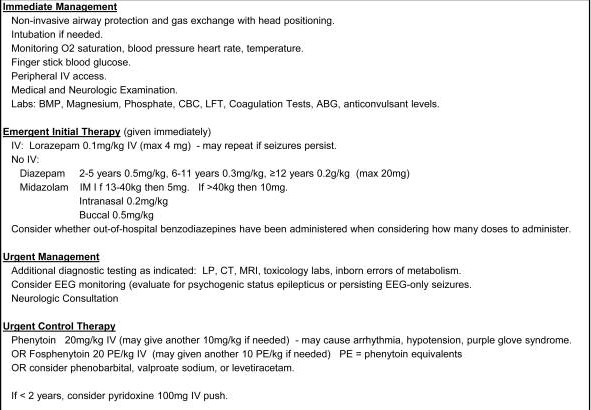
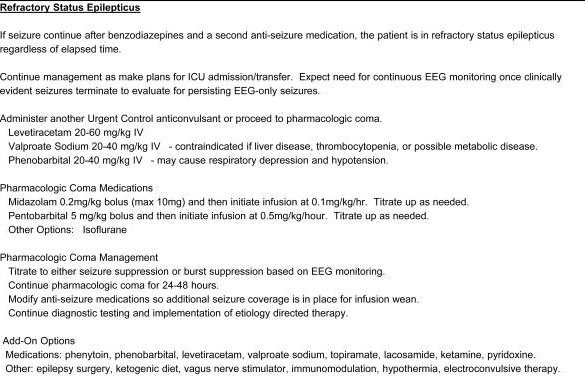
A quick word on status epilepticus: As mentioned previously, nearly 10% of all pediatric patients with new-onset seizure activity present to the ED in status epilepticus, which is defined as seizure activity > 5 minutes without return to mental status baseline.1 Unlike adults in which cerebral vascular accidents (CVAs) are the most common etiology of status epilepticus, febrile seizures are the most common etiology in pediatric patients, representing 1/3 of all episodes.17
Seizure Mimics
There are a number of seizure mimics that can present during the first year of life:
- Neonatal reflexes – the startle reflex can often be misinterpreted as seizure activity.1
- Benign sleep myoclonus – migrating myoclonic movements that do not wake the child.18
- Shuddering attacks – rapid shivering of the head, shoulders, and trunk.19
- Sandifer syndrome – arching of the back, crying, and writhing secondary to severe gastroesophageal reflux.1
- Breath holding spells – seen in 5% of pediatric patients 6 months – 5 years of age (presentation variable but often times mistaken for a seizure or brief resolved unexplained event).1
These seizure mimics are diagnoses of exclusion. Every effort should be made to obtain an accurate history of events to aid in clinical decision-making.
Seizure Syndromes Unique to Patients in the First Year of Life
The differential diagnosis of a patient experiencing an unprovoked afebrile seizure in the first year of life should include the following:
| Syndrome | Onset | Characteristics |
| Benign Convulsions Associated with Gastroenteritis | 6-60 months | Generalized seizures accompanying gastroenteritis, in the absence of electrolyte derangements. Often associated with Shigella and rotavirus infection.20 |
| Benign Familial Neonatal Convulsions | First days of life; self-resolves within 1 year. | Behavioral arrest, eye deviation, tonic stiffening, myoclonic jerks. Associated with a positive family history.9 |
| Benign Idiopathic Neonatal Convulsions | First days of life; self-resolves within 15 days. | “Fifth day fits” – clonic movements, apnea, positive family history. May represent 5% of all seizures in term infants.21 |
| Infantile Spasms | 4-18 months | Jerking of extremities, head, neck and trunk; typically in clusters. Associated with neurologic conditions (95% have developmental delay). Spontaneously resolve, however the majority develop new seizures.22 |
Seizure Syndromes Unique to Pediatric Patients1
Summary
The emergency physician’s role in addressing seizures in the first year of life is to stabilize the patient and initiate an appropriate evaluation based upon an accurate history and physical examination. While decision rules exist for simple febrile seizures, the evaluation of a complex febrile seizure and a new onset afebrile seizure must be weighed carefully. While seizure mimics do exist, the emergency physician must always rule out any life threatening conditions first.
Key Pearls
- Simple febrile seizure = Fever evaluation.
- Meningeal symptoms => LP
- 6-12 months of age with no immunization record/concern for meningitis => LP
- Received antibiotics and concern that treatment is masking symptoms => LP
- Complex febrile seizure = No clinical decision rules.
- Some evidence to suggest that, although rare, we may be missing acute bacterial meningitis (3 of 340 patients in the Kimia, et al.12 study)
- Further studies required; evaluation should be catered to the clinical scenario.
- Afebrile seizure = No clinical decision rules, again cater to clinical scenario.
- Focal seizure < 33 months, prolonged seizure duration, prolonged neuro deficit or co-morbidities => emergent neuroimaging.
- All patients get an EEG (expedited outpatient if well-appearing and no focal neuro).
- Up to 54% have recurrent seizures.
- Seizure treatment = ABCs, benzos => fosphenytoin => sedation with continuous EEG +/- anticonvulsant
- Seizure mimics exist, but so do seizure syndromes.
- Your history and physical examination are vital.
References / Further Reading
- Agarwal M, and Fox S. Pediatric seizures. Emerg Med Clin N Am 31 (2013):733-754.
- Taylor C, Piantino J, Hageman J, Lyons E, Janies K, Leonard D, Kelley K, Fuchs S. Emergency department management of pediatric unprovoked seizures and status epilepticus in the state of Illinois. J Child Neurol. 2015; 30(11):1414-1427.
- Carapetian S, Hageman J, Lyons E, Leonard D, Janies K, Kelley K, Fuchs S. Emergency department evaluation and management of children with simple febrile seizures. Clin Pediatr. 2014; 54(10):992-998.
- Patel A, and Vidaurre J. Complex febrile seizures: a practical guide to evaluation and treatment. J Child Neurol. 2013; 28(6):762-767.
- Sharieff G, Hendry P. Afebrile pediatric seizures. Emerg Med Clin N Am 29 (2011); 95-108.
- Granelli S, and McGrath J. Neonatal seizures: diagnosis, pharmacologic interventions, and outcomes. J Perinat Neonat Nurs. 2004; 18(3):275-287.
- Learn the Signs. Act Early: Developmental milestones. Centers for Disease Control and Prevention. 2016. Available from: http://www.cdc.gov/ncbddd/actearly/index.html
- Graves R, Oehler K, Tingle L. Febrile seizures: risks, evaluation, and prognosis. Am Fam Physician. 2012; 85(2):149-153.
- Zupanc M. Neonatal seizures. Pediatr Clin North Am. 2004; 51:961-978.
- Clinical practice guideline – febrile seizures: guideline for the neurodiagnostic evaluation of the child with a simple febrile seizure. American Academy of Pediatrics. Pediatrics. 2011; 127(2):389-394.
- Colvin J, Jaffe D, Muenzer J. Evaluation of the precision of emergency department diagnoses in young children with fever. Clin Pediatr. 2012; 156:469-472.
- Kimia A, Ben-Joseph EP, Rudloe T, et al. Yield of lumbar puncture among children who present with their first complex febrile seizure. Pediatrics. 2010;126(1):62–69.
- Sharma S, Riviello J, Harper M, et al. The role of emergent neuroimaging in children with new-onset afebrile seizures. Pediatrics. 2003; 111:1-5.
- Warden C, Brownstein E, Del Beccaro M. Predictors of abnormal findings of computed tomography of the head in pediatric patients presenting with seizures. Ann Emerg Med. 1997; 29: 518-523.
- Shinnar S, Berg A, Moshe S, et al. The risk of seizure recurrence after a first unprovoked afebrile seizure in childhood: an extended follow-up. Pediatrics. 1996; 98:216-225.
- Abend N, Loddenkemper T. Pediatric status epilepticus management. Curr Opin Pediatr. 2014; 26(6): 668-674.
- Stafstrom C. Neonatal seizures. Pediatr Rev. 1995; 16:248-255.
- Alam S, Lux A. Epilepsies in infancy. Arch Dis Child. 2012; 97:985-992.
- Tibussek D, Karenfort M, Mayatepek E, et al. Clinical reasoning: shuddering attacks in infancy. Neurology. 2008; 70:338-41.
- Verrotti A, Nanni G, Agostinelli S, et al. Benign convulsions associated with mild gastroenteritis: a multicenter clinical study. Epilepsy Res. 2011; 93:107-114.
- Vining E. Pediatric seizures. Emerg Med Clin North Am 1994; 12:973-988.
- Hancock E, Osborne J, Edwards S. Treatment of infantile spasms. Cochrane Database Syst Rev. 2008; (4):CD001770





1 thought on “Seizures in the First Year of Life”
Pingback: REBEL Core Cast 9.0 - Pediatric Status Epilepticus - REBEL EM - Emergency Medicine Blog