Welcome back to Small Talk; a new monthly section from emDOCs. Every first Wednesday of the month we will release high yield PEM content written by PEM talent from around the country. We hope you enjoy these reviews. Comments, questions, accolades or concerns: feel free to reach out to Joe Ravera, MD (pemgemspod@gmail.com).
Authors: Nathaniel White, MD (Pediatric Resident Physician, Instructor of Pediatrics, University of Vermont Children’s Hospital); Michele McDaniel, MD, FAAEM (Associate Fellowship Director, HS Clinical Assistant Professor of Pediatrics and Emergency Medicine, University of San Diego, California); Joe Ravera, MD (@pemuvm1, Director of Pediatric Emergency Medicine, Assistant Professor of Surgery, Division of Emergency Medicine, University of Vermont Medical Center) // Reviewed by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 45-day-old, full-term male infant presents to your ED with fever for the past 6 hours. The patient’s mom and dad checked his temperature, which was 101F (38.3C). He has not had rhinorrhea, cough, vomiting, diarrhea, or rash. He is tolerating feeds well, with good urine and stool output, though he’s a bit more fussy than usual. There are no sick contacts at home. The baby has no medical history and received VitK and HepB in the hospital. Mom and baby were home two days after an uncomplicated vaginal delivery. Mom had group B strep (GBS) on prenatal screening and was treated. She had negative screens for all other infectious diseases in her pregnancy.
On examination, the child is fussy but easily consoled. Pertinent findings include soft, flat fontanelle; normal color; two second capillary refill; no conjunctival injection or eye discharge; normal oropharyngeal and tympanic membrane exam; regular heart rate and rhythm without murmurs, gallops or rubs; clear lungs; soft abdomen; no rash; and normal, uncircumcised male genitalia.
Vital signs are as follows: T 38.1℃, HR 145, RR 35, BP 72/50, SpO2 99%RA.
The parents ask how you’re going to make sure there’s nothing wrong with their baby.
The Problem: Finding the Sick Needle in a Well Haystack
Nothing sparks fear into the heart of a seasoned pediatric or emergency medicine clinician like a febrile infant. While ill-appearing babies can be even more terrifying, their workups thankfully require little thinking: full septic evaluation, antibiotics, admit, next patient. But what about well-appearing infants with a fever? Approximately 500,000 febrile infants are evaluated in EDs annually. While the vast majority of these infections are either suspected or confirmed viral, approximately 8-13% of these patients have a serious bacterial infection (SBI) that requires urgent diagnosis and treatment. SBIs are generally defined as urinary tract infections (UTI), bacteremia, and meningitis; the latter two comprise a more severe subset of infections referred to as invasive bacterial infections (IBI). The most common source of SBIs are UTIs which are found in approximately 5-15% of febrile infants. Occult bacteremia and bacterial meningitis are rare, but it is notable that the incidence of these IBIs is approximately twofold higher among the most young (<28 days) when compared to infants in the second month of life. Bacteremia and meningitis are found in approximately 3% and 1%, respectively, of febrile neonates compared to 1.7% and 0.4% of febrile infants between 28-60 days of life.1,2
Several studies have also looked at the predictive value of experienced provider clinical assessment and structured clinical assessment tools such as the Yale Observation Score (YOS) and found that they were unreliable in detecting SBI in this population.3,4 This data underscores the old adage “you can’t trust a neonate.”
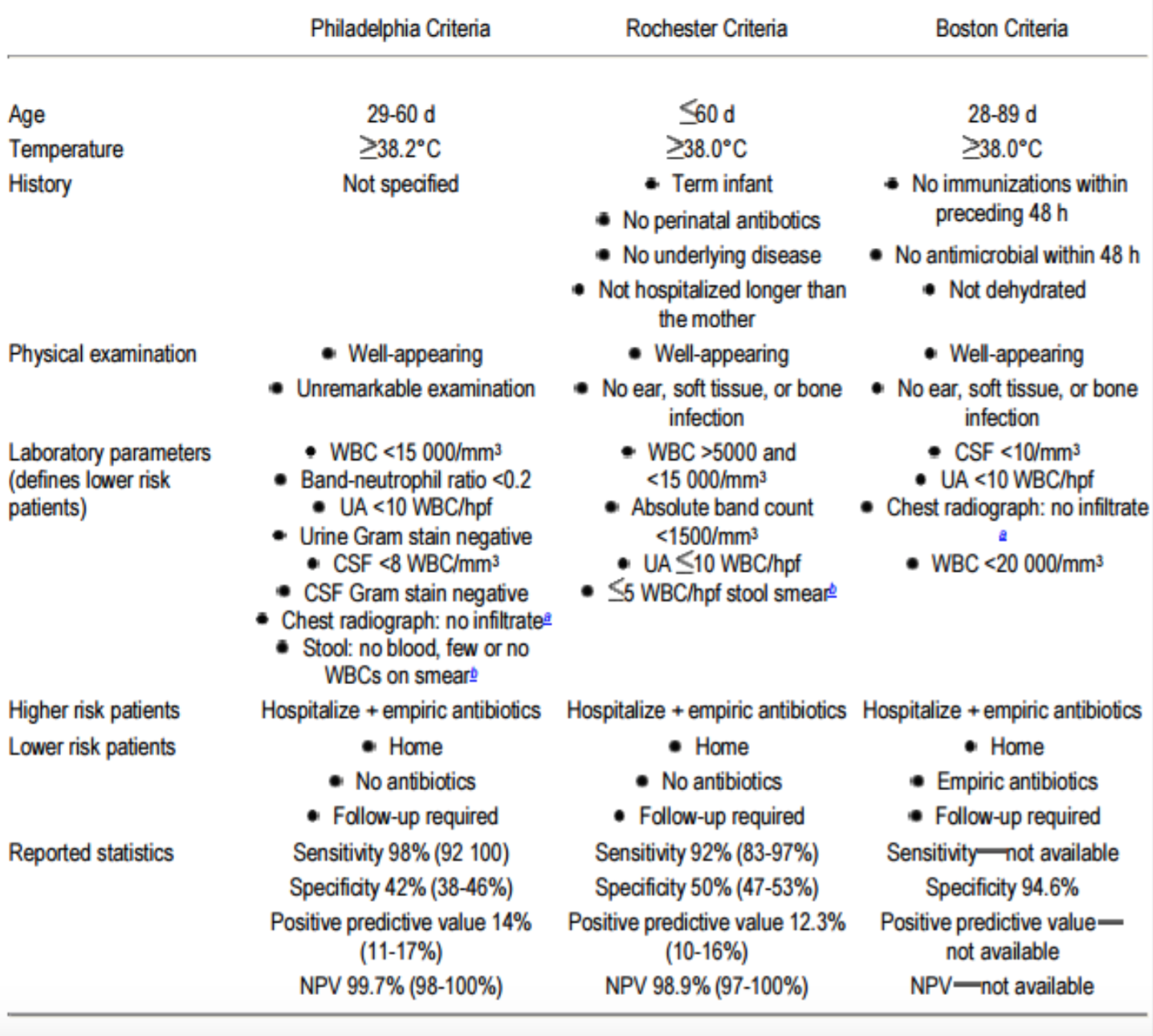
Given the limitations of clinical gestalt and the poor outcome associated with a missed SBI/IBI, the temptation may be to perform a full septic work up in all neonates. However, a complete sepsis work-up involving urine, blood and CSF studies is also associated with morbidity and cost. Over the past four decades, there has been a search for a methodology to categorize neonates as “low risk.” The first three widely accepted published criteria used to risk stratify infants were named after the cities in which they were derived; most EM physicians are familiar with the Boston, Rochester and Philadelphia criteria (Figure 1). While these have been reported in some papers to have high sensitivity, it is important to note that these risk stratification systems were developed pre-vaccination for both Streptococcus pneumoniae and Haemophilus influenzae. Additionally, several novel inflammatory markers (such as CRP and Procalcitonin) and the rapid availability of viral testing were not available when these criteria were developed. Despite our many advances, as of yet, no single biomarker with the degree of sensitivity necessary to be clinically useful has been identified that reliably predicts the risk of SBI in febrile infants.
Figure 1: Comparing the Philadelphia, Boston, and Rochester Criteria
This is the historical context in which emergency physicians and pediatricians have struggled to evaluate and manage febrile neonates. Hoping to provide some clarity, AAP has recently released consensus guidelines; the full article with flowchart algorithms can be found here.5
The Recommendations: To Whom They Apply and How to Use Them
These recommendations only apply to well-appearing, otherwise healthy, full term (>37 weeks) neonates. Children with obvious sources of bacterial infection (e.g., cellulitis), those who received perinatal antibiotics, those with documented or suspected immune compromise, and those with congenital or chromosomal abnormalities are also excluded from these algorithms. While there are four distinct age groups, we can really break the management down to three ranges with variation in work up based on age (see age range below).
Risk Stratification: What Makes a Baby High Risk According to AAP
For nearly 40 years we have searched for some combination of clinical and inflammatory markers that stratify neonatal SBI risk. Whether it’s the historical criteria (see above) or the newer Step by Step, PECARN, or Roseville (see below), there is a large volume of literature trying to delineate which features identify high risk infants. Drawing from both historical and contemporary data, the AAP has defined high risk inflammatory markers as:
Temperature >38.5
C-Reactive Protein (CRP) > 20 mg/L
Absolute Neutrophil Count (ANC) > 4000 mm3
Procalcitonin > 0.5 ng/ml
Risk Stratification by Age
Group 1: Never trust a neonate. Full septic workup, evaluate for HSV, administer IV antibiotics, and admit.
Age 0-7 days: The AAP recommendations exclude children under 7-days-old. While there are several inpatient sepsis calculators that have been utilized in this population6, it should be noted these are for inpatients and not babies presenting to the ED after discharge. While the guidelines are silent on work up, these authors suggest a full septic work up and admission with antibiotics.
Age 8-21 Days: From the EM perspective, this group remains easy. Every neonate in this age group should have urinalysis, blood culture, and LP for CSF studies sent; be started on parenteral antibiotics; and admitted. They should also be evaluated for HSV with a detailed birth history for high risk exposures, a skin evaluation for legion, and if appropriate swabs and HSV PCR from the CSF. An elevated ALT can also be a subtle clue to HSV. If there is any concern for HSV the baby should be started on acyclovir.7 Inflammatory markers including CRP, ANC, and procalcitonin can be sent but are not necessary for ED management.
Group 2: A Big Hedge for One Week of Life
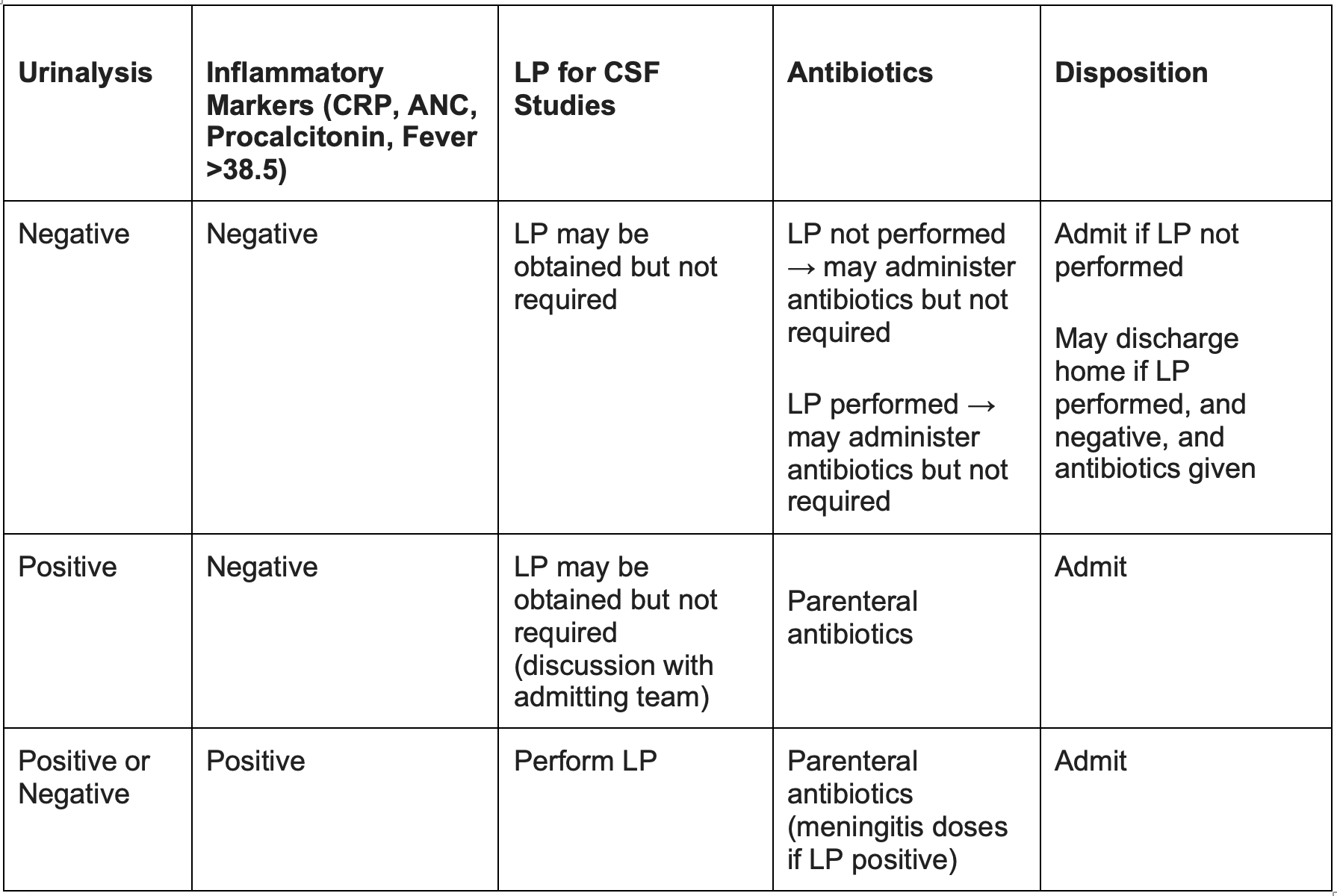
Age 22-28 Days: In this narrow age range, the guidelines provide some room for informed decision making between the clinical team and parents, taking into account levels of risk tolerance and family values regarding the need for a lumbar puncture, antibiotics and hospital admission. Although most roads in this guideline lead to a full septic workup, admission, and antibiotics, there are unique circumstances where it may be reasonable to modify these recommendations. All infants in this group should, at a minimum, have a urinalysis, blood culture, and inflammatory markers (CRP, ANC and Procalcitonin if available) sent for analysis. If any of the inflammatory markers are positive those babies should undergo an LP, be given IV antibiotics, and be admitted. If the urinalysis is positive and ALL inflammatory markers are negative, a lumbar puncture for CSF studies may be obtained but is not required. These patients should still receive IV antibiotics and admission for observation. If the UA and inflammatory markers are negative there are two potential options: if a lumbar puncture is obtained and negative, the septic work up is complete and these patients may be discharged after a dose of parenteral antibiotics with close outpatient follow up in 24 hours. Another option would be to defer the LP and admit the children off antibiotics for inpatient monitoring. (Figure 2)
Figure 2: A Matrix for the Evaluation of the 22-28 Day Old
Group 3: The Personalized Medicine Group
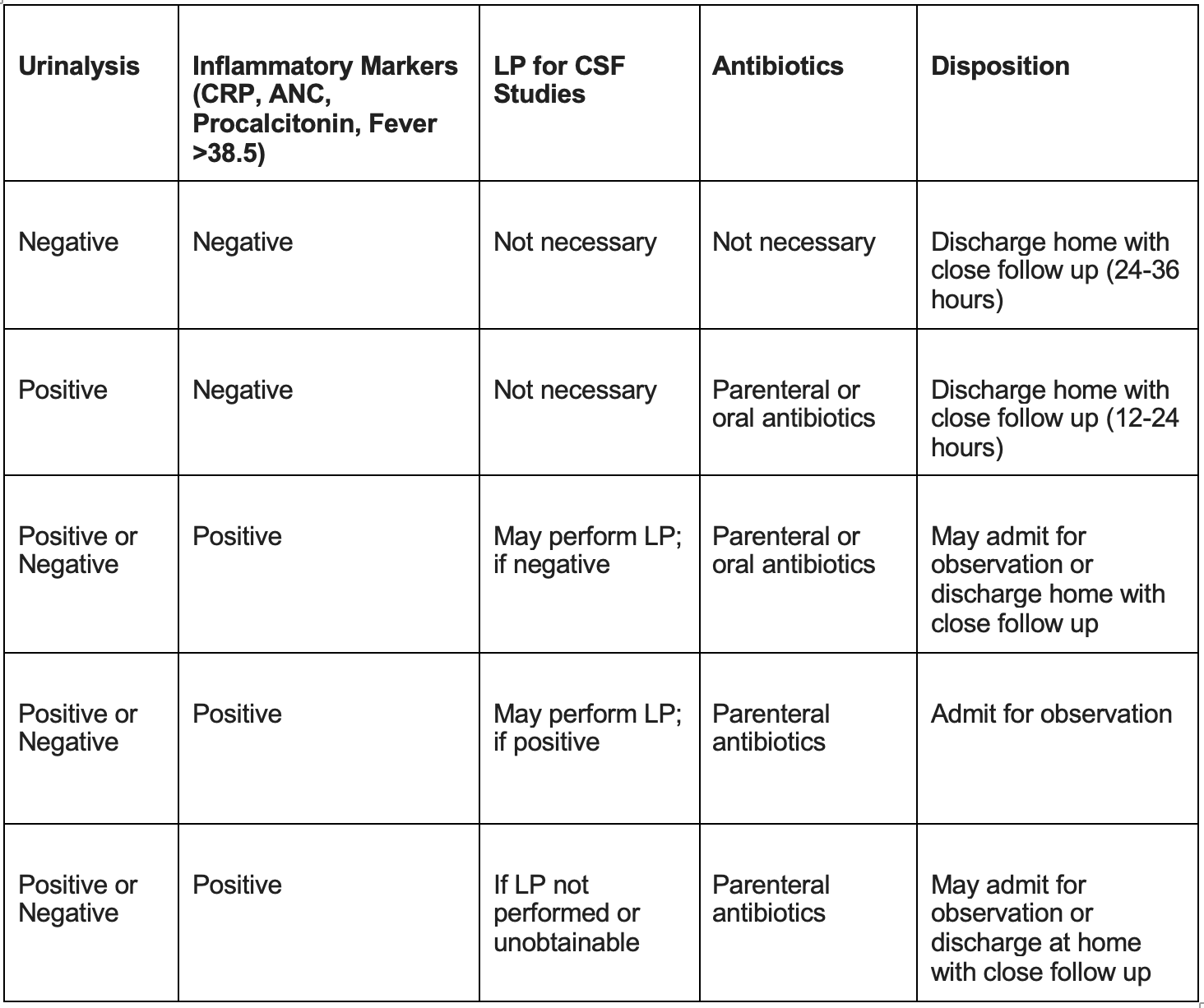
Age 29-60 Days: The guidelines acknowledge that, given changes in bacteriology, advancements in laboratory studies and the growing body of epidemiological data, this group can be readily risk stratified using available diagnostic studies and that management can be tailored accordingly. Each infant in this group should have a urinalysis, blood culture, and inflammatory markers (CRP, ANC, and Procalcitonin) sent for analysis. While the decision algorithm is discussed below, in short, if the initial work up is negative, infants may be discharged home without antibiotics and with close follow-up. Infants with a positive urinalysis and negative inflammatory markers may be treated just like infants >60 days of age with a UTI, started on oral antibiotics, and discharged. The nuances of the decision tree revolve around infants with positive inflammatory markers.
The guidelines recommend that if inflammatory markers are positive, the clinical team may decide to perform or defer the lumbar puncture. If the lumbar puncture is deferred or uninterpretable, parenteral antibiotics should be administered, and the infant may be observed in the hospital or at home with close follow up. If the lumbar puncture is performed and is negative but the urinalysis is positive, the patient may be initiated on either parenteral or oral antibiotics and then either admitted for observation or discharged home with close follow up. Finally, if the lumbar puncture is performed and is positive, the patient should be started on parental antibiotics and admitted to the hospital (Figure 3).
Figure 3: A Matrix for the Evaluation of the 29-60 Day Old
The Data Behind Risk Stratification: Recent Publications
As mentioned in the introduction, the search for a method to stratify risk in febrile neonates has been going on for the better part of four decades. While the combination of inflammatory markers recommended by new guidelines have not been prospectively validated, they are rooted in several recent studies which are presented below:
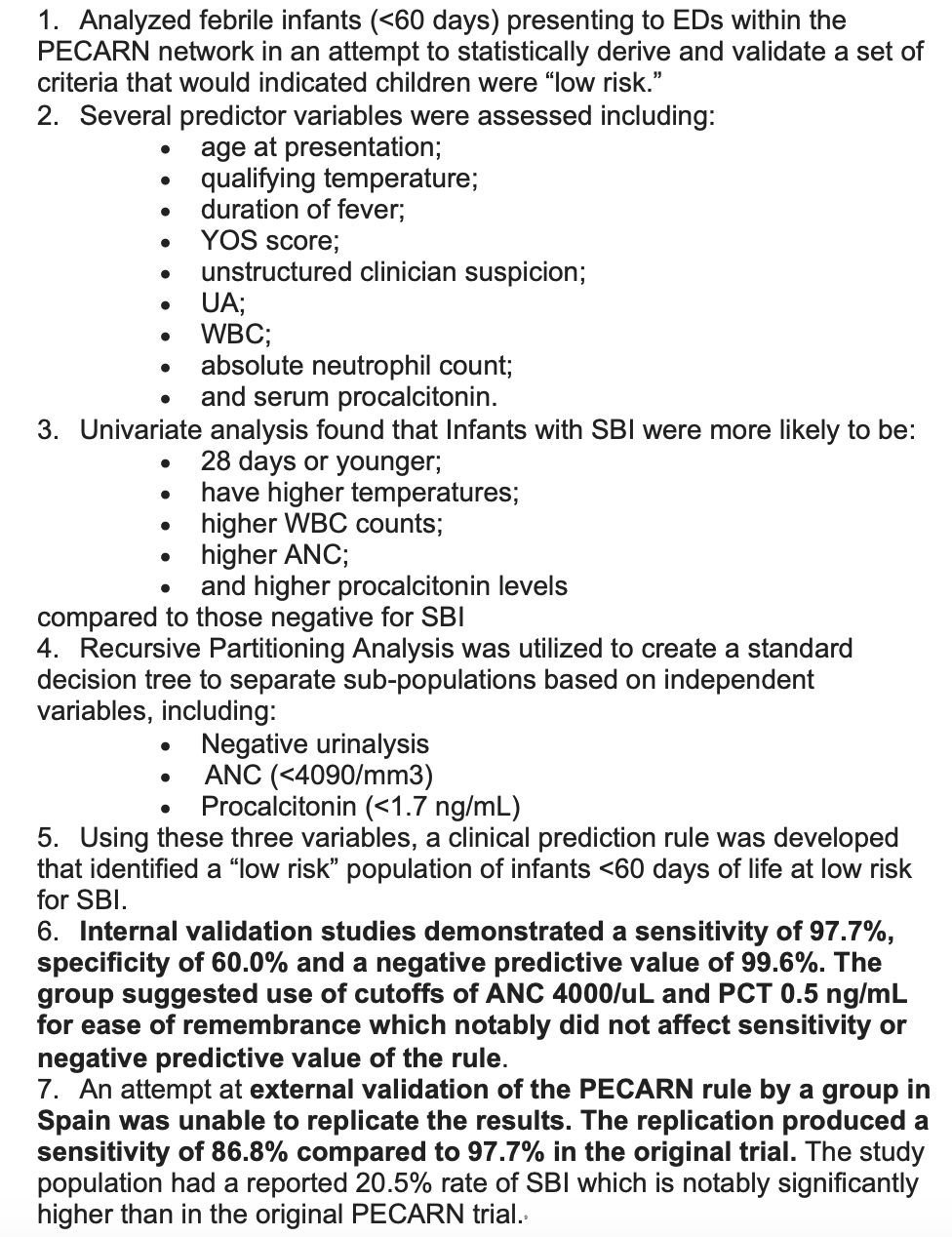
PECARN8
Step by Step10

The Roseville Criteria12

Caveats and Controversies: Frequently Asked Questions
What About Well Appearing, Vaccinated Children Over 3 months?
Current literature would suggest the rate of bacteremia and meningitis is extremely low in this age group and, as such, routine surveillance cultures and CSF are not necessary. Urine testing may be appropriate based on several clinical factors such as age, sex, circumcised vs. uncircumcised and symptomatology.14
How Should Prematurity Affect the Work Up?
Incidence of SBI in premature infants <48 weeks postconceptional age is similar to that of full-term infants. Premature infants should be corrected to 40 weeks and analyzed in the subgroup to which they then belong.15
What do I do when the parents say the child had a fever at home, but the child is afebrile in the ED?
This can be particularly tough, especially when you are looking at very well appearing afebrile neonate. It can be tempting to ignore or “re-check” away a fever that was documented at home. Several studies have examined this exact question and, while there does appear to be a slightly lower rate of SBI in afebrile neonates compared to febrile neonates in the ED (~8% vs. ~12%), the risk of SBI is generally considered high enough that an age-appropriate septic work up is recommended regardless of current temperature.16,17,18 In short, an objective fever at home should be considered a fever in the ED. It is worth noting that there is no concrete data on subjective fever with afebrile children. It is our expert recommendation that if there is no documented fever and the child appears well, then a reasonable management strategy would be a brief period of observation followed by a recheck of temperature in the ED. If the child remains afebrile and well appearing, they can be discharged home with close clinical follow up.
What do I do if the kid has an obvious viral syndrome like Influenza or RSV?
This question really boils down to what is the chance a child has a viral illness AND an SBI? Several studies have analyzed this, and the rates of UTI vary from 2-13%, bacteremia occurs in around 0.8%, and meningitis in about 0-0.4%.19-22 While the risk of IBI is reduced, the majority of the risk reduction comes from infants >28 days. Febrile children under 28 days old should have the same workup regardless of the presence of a viral source. In children older than 28 days, the presence of a viral infection can be a rationale to abridge the work up and manage patient care according to the viral infection. It should be noted that these studies look at swab-positive viral illness; if the child has a “viral syndrome” without a documented source, there is no data that supports abridging the septic work up.
What if the child has fever post vaccination?
The recent AAP guidelines excluded neonates with fever post-vaccination, as there is literature indicating that up to 40% of babies can have a transient fever after immunization.23 Oftentimes, these children have just received their 2-month immunization for pneumococcal disease, which puts them on the older end of the spectrum for these guidelines. Thus, these authors recommend that neonates who are otherwise well appearing with a transient fever post vaccination can likely be managed expectantly with close clinical follow up.
Pearls and Pitfalls:
- These guidelines only apply to neonates who are otherwise healthy, well appearing, full term, received no perinatal antibiotics and have no clear source of bacterial infection.
- Children should be risk stratified according to age — all children under 21 days (and most children under 28 days) should receive a full septic work up.
- Children 1-2 months can be managed based on the results of the inflammatory markers and urinalysis.
- Children 1-2 months with fever from a documented viral source or vaccinations can be managed according to their clinical presentation and can go outside the algorithm.
Case Continued:
The 45-day old received an age appropriate work-up per the guidelines. Urinalysis was negative. The child did not have any elevated inflammatory markers and never had a temperature over 38.5. The baby remained well in the ED, no LP was performed, and the parents followed up with their pediatrician the next where a viral swab sent from the ED was positive for rhinovirus. Turns out the baby just had a cold.
References/Further Reading:
1) Biondi EA, Lee B, Ralston SL, et al. Prevalence of Bacteremia and Bacterial Meningitis in Febrile Neonates and Infants in the Second Month of Life: A Systematic Review and Meta-analysis. JAMA Network Open. 2019 Mar; 2(3): e190874.
2) Bonilla L, Gomez B, Pintos C, et. al. Prevalence of bacterial infection in febrile infants 61-90 days old compared to younger infants. The Pediatric Infectious Disease Journal. 2019 Dec; 38(12):1163-1167.
3) Baker MD, Avner JR, Bell LM. Failure of infant observation scales in detecting serious illness in febrile, 4- to 8-week-old infants. The Journal of Pediatrics. 1990 Jun; 85(6):1040-1043.
4) Nigrovic LE, Mahajan PV, Blumberg SM, et al. (2017). The Yale Observation Scale score and the risk of serious bacterial infections in febrile infants. The Journal of Pediatrics. 2017 Jul; 140(1):e20170695
5) Pantell RH, Roberts KB, Adams WG, et al; Subcommittee On Febrile Infants. Evaluation and Management of Well-Appearing Febrile Infants 8 to 60 Days Old. Pediatrics. 2021 Jul 19.
6) Kuzniewicz MW, Puopolo KM, Fischer A, et al. A Quantitative, Risk-Based Approach to the Management of Neonatal Early-Onset Sepsis. JAMA Pediatr. 2017 Apr 1;171(4):365-371.
7) Kimberlin D. When should you initiate acyclovir therapy in a neonate? The Journal of Pediatrics. 2008 Aug;153(2):155
8) Kuppermann N, Dayan PS, Levine DA, et al. A clinical prediction rule to identify febrile infants 60 days and younger at low risk for serious bacterial infections. JAMA Pediatrics. 2019 Apr; 173(4): 342-351.
9) Velasco R, Gomez B, Benito J, et al. Accuracy of PECARN rule for predicting serious bacterial infection in infants with fever without a source. Archives of Disease in Childhood. 2021 Feb;106(2):143-148.
10) Mintegi S, Bressan S, Gomez B, et al. Accuracy of a sequential approach to identify young febrile infants at low risk for invasive bacterial infection. Emergency Medicine Journal. 2014 Oct;31(e1):e19-24.
11) Gomez B, Mintegi S, Bressan S, et al. Validation of the “Step-by-Step” approach in the management of young febrile infants. The Journal of Pediatrics. 2016 Aug; 138(2):e20154381.
12) Nguyen THP, Young BR, Poggel LE, et al. Roseville Protocol for the Management of Febrile Infants 7-60 Days. Hosp Pediatr. 2020 Dec 17:hpeds.2020-0187. doi: 10.1542/hpeds.2020-0187.
13) Cruz AT, Mahajan P, Bonsu BK et. al Febrile Infant Working Group of the Pediatric Emergency Care Applied Research Network. Accuracy of Complete Blood Cell Counts to Identify Febrile Infants 60 Days or Younger With Invasive Bacterial Infections. JAMA Pediatr. 2017 Nov 6;171(11):e172927.
14) Cioffredi LA, Jhaveri R. Evaluation and management of febrile children a review. JAMA Pediatrics. 2016 Aug; 170(8):794-800.
15) Inoue N, Kim TY, Birbeck-Garcia AM, et al. Incidence of serious bacterial infections in ex-premature infants with a postconceptional age less than 48 weeks presenting to a pediatric emergency department. The Western Journal of Emergency Medicine. 2009 Feb; 10(1): 37-40.
16) Brown L, Shaw T, Moynihan JA, et al. Investigation of afebrile neonates with a history of fever. CJEM. 2004 Sep;6(5):343-8.
17) Ramgopal S, Janofsky S, Zuckerbraun NS, et al. Risk of Serious Bacterial Infection in Infants Aged ≤60 Days Presenting to Emergency Departments with a History of Fever Only. J Pediatr. 2019 Jan;204:191-195.
18) Yarden-Bilavsky H, Bilavsky E, Amir J, et al. Serious bacterial infections in neonates with fever by history only versus documented fever. Scand J Infect Dis. 2010;42: 812-816
19) Krief WI, Levine DA, Platt SL, et al. Influenza virus infection and the risk of serious bacterial infections in young febrile infants. The Journal of Pediatrics. 2009 Jul; 124(1): 30-39.
20) Mahajan P, Browne LR, Levine DA et al. Risk of bacterial coinfections in febrile infants 60 days old and younger with documented viral infections. The Journal of Pediatrics. 2018 Dec; 203:86-91 e82.
21) Bonadio W, Huang F, Nateson S, et al. Meta-analysis to Determine Risk for Serious Bacterial Infection in Febrile Outpatient Neonates With RSV Infection. Pediatr Emerg Care. 2016 May;32(5):286-9.
22) Levine DA, Platt SL, Dayan PS, et al; Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics. 2004 Jun;113(6):1728-34.
23) Prymula R, Siegrist CA, Chlibek R, et al. Effect of prophylactic paracetamol administration at time of vaccination on febrile reactions and antibody responses in children: two open-label, randomised controlled trials. Lancet. 2009 Oct 17;374(9698).





3 thoughts on “Small Talk – Hot Off The Presses: The Latest AAP Guidelines for the Febrile Neonate”
Thanks for the comprehensive review – one question about temperature as an “IM”. It appears that if a temp >38.5 is a positive IM — than for those kids you don’t even need the results of the other IMs? IE – if they present with 38.6 – they get the next layer of work up – no matter what their cRP, PCT or ANC is???
Dr. Ravera – Yes, AAP used height of the fever in the same way they used blood inflammatory markers. This was likely based out of the Roseville criteria published earlier this year which also used a temperature above 38.5 as a marker of higher risk.
Pingback: Christmas in July: New Guidelines for Managing Well-appearing Febrile Infants from the American Academy of Pediatrics - First10EM