Spinal Epidural Hematoma
By Seth Lotterman MD
(Assistant Professor of EM / Assistant Residency Director, University of Connecticut School of Medicine)
Edited by Alex Koyfman MD (@EMHighAK) and Stephen Alerhand MD (@SAlerhand)
Patient Case
After scanning the tracker for the next patient to evaluate, you click on yet another patient with back pain. You have already seen a few patients with back pain that you were able to discharge, so you figure this one should not be too difficult. You enter the room and meet an 83 year-old female describing a sudden onset of back pain that started several hours earlier after she bent over to let her dog out. She was able to walk back to bed, but since then has felt decreased movement of her legs, along with some numbness of waxing and waning intensity. The patient does not recall any specific trauma and denies fevers. Her past medical history includes an abdominal aortic aneurysm, hypertension, chronic renal insufficiency, and atrial fibrillation for which she is anticoagulated with Warfarin.
On exam, the patient is afebrile with stable vital signs and overall well appearing. Her exam is significant for bilateral lower extremity weakness, with 2/5 strength in both legs. She also has decreased sensation, decreased rectal tone, and decreased bilateral lower extremity reflexes. Her upper extremity strength, sensation, and reflexes are normal.
You quickly realize this is not going to be a simple discharge home with an NSAID and muscle relaxant. You order labs and an MRI of her thoracic and lumbar spine. Other than an INR of 2.6, her labs are unremarkable. The MRI shows a focal epidural hematoma at T11 with marked cord displacement, mass effect, and edema of the cord at T11. The patient receives FFP to reverse her coagulopathy as well as intravenous steroids to reduce inflammation. After discussing the case with the neurosurgeon, the patient is transferred emergently to the operating room for surgery.
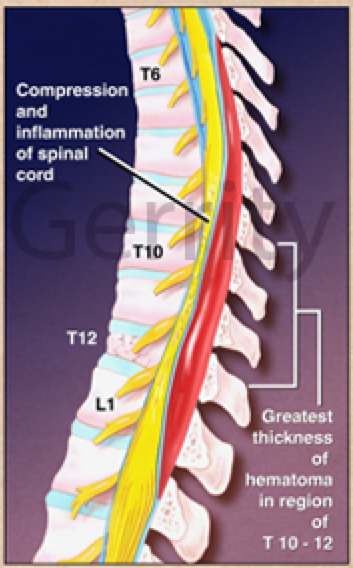
(http://www.medillsb.com/ArtistPortfolioLarge.aspx?AID=286&IID=138308)
Debrief
This patient had a spinal epidural hematoma, which is defined as a spontaneous collection of blood in the spinal epidural space.1 Initially reported in the 17th century, this neurosurgical emergency is a rare condition – reported occurrence is 0.1 patients/100,000 people (i.e. 1 in a million).2,3 It is a difficult diagnosis to make and can be initially misdiagnosed as other serious conditions such as ischemic heart disease, stroke, or aortic dissection.4 Just over one-third of cases have an unknown etiology and slightly more than 25% are associated with coagulation disorders and 1/3 of patients are on anticoagulant therapy. Vascular malformations and a wide variety of traumatic etiologies have also been described, including competitive swimming, sit-up exercises, weight lifting, trumpet and piano playing.2,3,5 It is thought that the epidural venous plexus at the dorsal aspect of the cervical and thoracic spinal canal is the source of the bleeding. These are thin walled veins and could be injured with activities that increase intrathoracic and intra-abdominal pressure.1,6 In some cases, arterial bleeding could also be an etiology, possibly the result of extreme movements.6 Neurologic deficits may result from direct compression of the hematoma on the lateral columns or compromise of vascular flow.1
Patients often present with acute radicular pain and neurological deficits that progress over hours to days. Neurologic findings vary widely and are related to the spinal level involved and size of the hematoma.3 Pain may occur prior to neurologic deficits making diagnosis more difficult.3 Maneuvers that increase intraspinal pressure, such as coughing, sneezing, or straining may worsen the pain. On exam, percussion over the spine may elicit tenderness as well.3 MRI, specifically sagittal (which determines anterior-posterior location and superior-inferior borders), is the diagnostic test of choice.3


Journal of the AAOS (http://www.jaaos.org/content/18/8/494/F1.expansion)
Treatment is surgical decompression, unless the deficit is minimal or is spontaneously improving, which has been described in case reports.7,8 The outcome is primarily dependent on the preoperative spinal cord injury, but the time to decompressive surgery also influences the outcome.1,2 There is an 8% overall mortality rate.3
Final Words
Though an extremely rare diagnosis, spinal epidural hematoma is very important to consider due to its potentially devastating effects, especially in elderly patients on anticoagulation who report sudden pain and neurological deficits. As in the above case, it is important to remember that time to decompressive surgery is an important prognostic factor.2
References / Further Reading
- Estaitieh N, Alam S, Sawaya Atypical presentations of spontaneous spinal epidural hematomas. Clin Neurol Neurosurg. 2014 Jul;122:13506.
- Dziedzic T et al. Management and neurological outcome of spontaneous spinal epidural hematoma. J Clin Neurosci (2015).
- Marx J, Hockberger R, Walls R Rosen’s Emergency Medicine Concepts and Clinical Practice, 8th 2014.
- Saritas A, Guneysu F, Guneysu S, Buyukkaya R, Kandis H. “An unusual presentation of spontaneous spinal epidural hematoma” The Journal of Emergency Medicine, Vol. 47, No. 6, pp. 689–691, 2014.
- Chang HJ, Su FJ MD, Huang YC, Chen SH. “Spontaneous spinal epidural hemorrhage from intense piano playing” American Journal of Emergency Medicine 32 (2014) 688.e3–e5
- Kulkarni AG, Nag K, Shah S. “Cervical epidural haematoma causing Brown-
- Sequard syndrome: a case report” Journal of Orthopaedic Surgery 2013;21(3):372-4
- Buyukkay R, Aydin O, Hakyemez B, Seref D “Spontaneous recovery after development of a spinal epidural hematoma: a case report” American Journal of Emergency Medicine. 32 (2014) 291.e1–e3
- Iwashita K, Shigematsu K, Higa K, Nitahara K. “Spontaneous Recovery of Paraplegia Caused by Spinal Epidural Hematoma after Removal of Epidural Catheter” Case Reports in Anesthesiology Volume 2014 (2014)
- http://www.ncbi.nlm.nih.gov/pubmed/23380090
- http://www.ncbi.nlm.nih.gov/pubmed/20466256
- http://www.ncbi.nlm.nih.gov/pubmed/19857440




