
Introduction
History
- Synthetic cannabinoids were first designed after the structure of the primary psychoactive compound in marijuana, 9-tetrahydrocannabinol (9-THC), was figured out in the 1960s.
- Synthetic cannabinoids have been used as a tool to study endocannabinoid biochemistry and also to design cannabinoid derivatives for medicinal use, for example in appetite stimulants and pain medications.
- In the late 1990s, The John W. Huffman research group at Clemson University began to synthesize over 450 cannabinoids. JWH-018 was one such synthetic cannabinoid that his group created for research purposes but in 2004 it first appeared in Europe in recreational smoke blends under the marketed name “Spice” or “K2.”

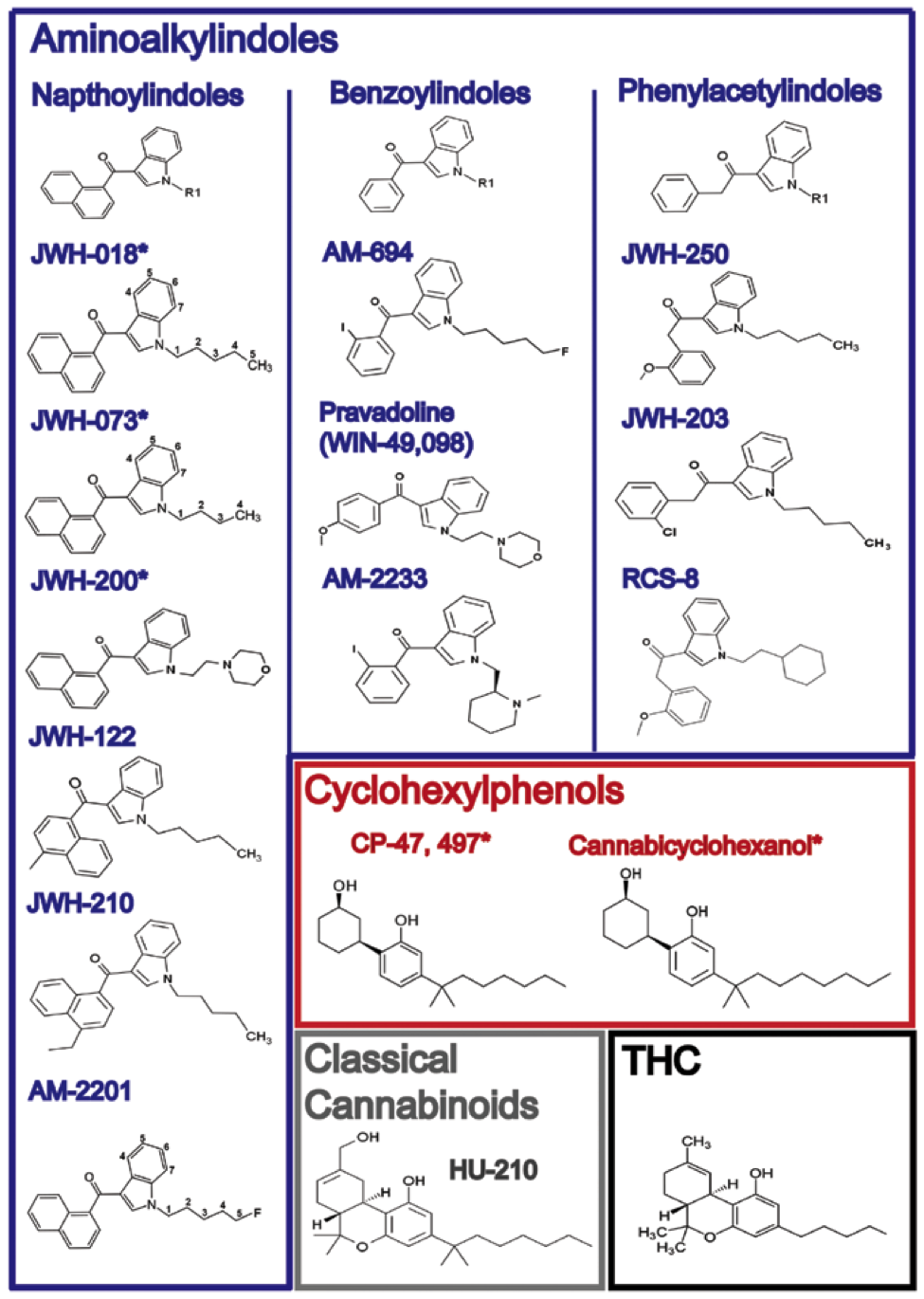
Synthetic Cannabinoid Types
- There are many types of synthetic cannabinoids. More and more continue to be created to either produce a “better high” or evade detection in drug screens. Each has their own distinct binding affinity to the cannabinoid receptor subtypes (CB1 and CB2).
- For example, HU210 is reported to bind to the CB1 and CB2 receptors with 100 times the affinity of 9-THC.
- Blends of K2 contain JWH-018 (a full agonist at the CB1 and CB2 receptor), JWH-073 (somewhat selective for CB1), and JWH-250 (CB1 and CB2 agonist).
- First generation synthetic cannabinoids are believed to be more benign than the newer generation cannabinoids, which are more likely to cause cardiotoxicity and neurotoxicity. One such newer generation synthetic cannabinoid is ADB-PINACA (N-[1-amino-3,3-dimethy-1-oxobutan-2-yl]-1-pentyl-1H-indazole-3-carboxamide), the compound identified in the recent Colorado outbreak known locally as Black Mamba.
Street Names
- K2, Spice, Black Mamba, Blaze, Bliss, Bombay Blue, Fake Weed, Genie, Moon Rocks, Mr. Nice Guy, Skunk, Yucatan Fire and Zohai.
Legal Status
- In July 2012, the Synthetic Drug Abuse Prevention Act of 2012 was signed into law, which banned 26 substances commonly found in synthetic marijuana, placing them under Schedule I of the Controlled Substances Act.
- Despite legislation banning its use, synthetic cannabinoid use is becoming increasingly popular and is still readily available. Synthetic cannabinoids have been found in smoke shops, gas stations, and can be found for sale on the internet. They can be found in legal retail stores and packaged as incense or potpourri and may be labeled “not for human consumption.”
Growing Popularity and Media Attention
- In 2010, the DEA reported that 30–35% of specimens submitted by juvenile probation departments tested positive for synthetic cannabinoids.
- According to the 2011 National Institutes of Drug Abuse (NIDA)-sponsored Monitoring the Future survey, 11% of high school seniors reported smoking synthetic marijuana, making it one of the most commonly abused drugs in this population — second only to marijuana.
- 4.5% of urine specimens collected from 5,956 U.S. athletes tested positive for synthetic cannabinoids, the highest of all drug classes detected.
- A recent NEJM letter to the editor described an outbreak in Colorado where a total of 263 cases of possible synthetic cannabinoid exposure were identified during August 21-September 19 2013, however only 15 of these cases were reported to the state poison control center. Of the 263 cases, 76 sought medical attention in emergency departments and 7 were admitted to intensive care units. Colorado health officials identified a novel synthetic cannabinoid, ADB-PINACA, which was associated with neurotoxicity and cardiotoxicity.
Clinical Highlights
Route of Ingestion
- Synthetic cannabinoids can be smoked, insufflated, or orally ingested.
Symptoms
- The psychoactive effects are similar to 9-THC and include altered time perception, anxiety, changes in mood, confusion, hallucinations, and psychomotor agitation. There have been case reports of induced psychoses, unmasking of underlying psychiatric disease, and suicidal attempts especially in individuals with a personal or family history of psychiatric conditions. Additional undesirable effects include dry mouth, nausea, vomiting, tachycardia, palpitations.
- Life-threatening neurotoxic effects, like seizures or ischemic stroke, and cardiotoxic effects, like arrhythmia or acute coronary syndrome / myocardial infarction, rarely occur with synthetic cannabinoid intoxication and likely occur more often with the newer synthetic cannabinoids presumably due increased potency to the cannabinoid receptors.
Treatment
- Similar to marijuana intoxication, patients typically do not need measures other than symptomatic or supportive treatment. No antidote exists for synthetic cannabinoid poisoning. Seizure control and agitation can be treated with benzodiazepines. Gastrointestinal decontamination typically has no role in patients using synthetic cannabinoids, but it may be considered in large-quantity ingestions.
- For severe intoxication, especially with the newer generation synthetic cannabinoids, intensive care monitoring and management for seizures, ischemic stroke, and possible cardiotoxicity may be required. Death due to neurotoxicity or cardiotoxicity as well as suicidality has been reported with synthetic cannabinoid use.
Detection
- Synthetic cannabinoids do not show up in the standard urine drug screens available in most hospitals, which test for Tetrahydrocannabinol. The best methods for detecting synthetic cannabinoids are liquid chromatography / tandem mass spectrometry (LC-MS/MS) and gas chromatography / mass spectrometry (GC/MS) and are only available in select laboratories.
- The inability to detect synthetic cannabinoids using standard urine drug screens adds to its growing popularity.
Bottom Line
- Suspect synthetic cannabinoids in your patients who present with marijuana-like symptoms but screen negative for cannabis using standard urine drug screens. Most patients require symptomatic support as you would normally do for your patient presenting with marijuana intoxication.
- However, there have been a growing number of cases associated with life-threatening neurotoxic effects (seizures, strokes) and cardiotoxic effects (arrhythmia, acute coronary syndrome / myocardial infarction), presumably due to increased potency to the cannabinoid receptors in the newer synthetic cannabinoids.
Further Reading
- Crews, B. American Association of Clinical Chemistry, Clinical Laboratory News. Synthetic Cannabinoids. Vol 39, No 2.
- Harris C. Brown A. Synthetic Cannabinoid Intoxication. J Emerg Med. 2013;44(2):360-366.
- Monte A, et al. Correspondence: An Outbreak of Exposure to a Novel Synthetic Cannabinoid. N Engl J Med 2014; 370:389-390.
- Nelson L. Synthetic Cannabinoids: The Newest, Almost Illicit Drug of Abuse. New York State Poison Centers Toxicology Letter. Vol XVI, No 2.
- Vashi, Sonam (September 26, 2012). K2 Trend Not Slowing Down. WebMD Medical News.
- http://www.ncbi.nlm.nih.gov/pubmed/24275167
- http://www.ncbi.nlm.nih.gov/pubmed/24378862
- http://www.ncbi.nlm.nih.gov/pubmed/23890687
- http://www.ncbi.nlm.nih.gov/pubmed/24106544
- http://www.ncbi.nlm.nih.gov/pubmed/23609214
- http://www.ncbi.nlm.nih.gov/pubmed/21802885
- http://www.ncbi.nlm.nih.gov/pubmed/22271566





1 thought on “Synthetic Cannabinoids”
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM: Synthetic Cannabinoid Intoxication - emDOCs.net - Emergency Medicine Education