Authors: Vladimir Thomas, MD (EM Resident Physician, Downstate Medical Center / Kings County Hospital) and James Willis, MD (Clinical Assistant Professor / Assistant Program Director, Downstate Medical Center / Kings County Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
It is 4AM and a 13 year-old male presents to your ED contorted in pain by EMS. He is accompanied by his mom who states she suddenly heard him shout out while sleeping. She denies any significant past medical history. He says he feels nauseous and vomited twice en route to the hospital. On exam, vitals are T 98.7, HR 104, BP 110/70, RR 18, O2 100%. He is noted to be exquisitely tender and mildly swollen over his left testicle which appears elevated.
Principles
Painful testes account for 1% of emergency department visits each year. Testicular pathology requires rapid diagnosis to prevent potential infertility or other complications. In severe cases, complications such as necrosis and gangrenous testis may arise. In the case of torsion, salvage is time dependent with 96% success rates when perfusion is restored within 4 hours. Salvage is less than 10% if intervention is delayed for more than 24 hours. The annual incidence of torsion is said to be 3.8 in 100,000 males under 18. Historically, the incidence of torsion is 1 in 4000 in males under 25. The disease may occur at any age but is primarily associated with a bimodal distribution in the first year of life and adolescence (ages 11-18).
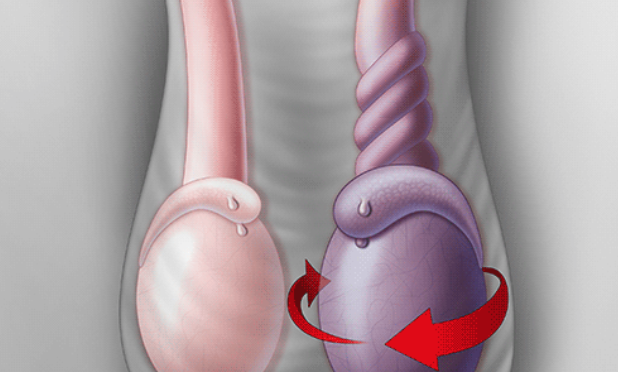
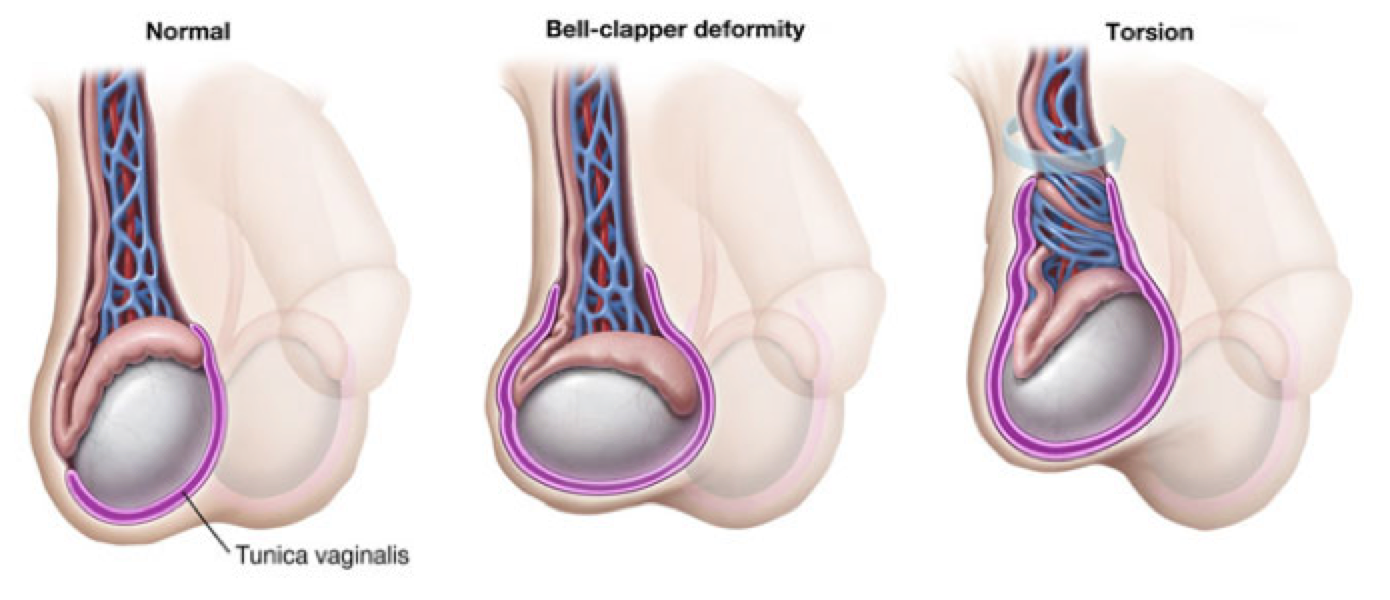
The testes are normally smooth, ovoid, and slightly asymmetric in size and firm but not hard. Prior to puberty, length may vary from 1.5 to 2 cm and increase to as much as 4 to 5 cm after puberty. The vas deferens projects from the tail of the epididymis and fixes to the vascular pedicle of the testicle to form the spermatic cord. The cord courses cranially to the inguinal canal. The testes enters the scrotum through the inguinal canal projecting from the abdomen. The tunica vaginalis results from the invagination of the peritoneum through the canal partly covering the testis and epididymis. A bell clapper deformity occurs when the tunica completely covers the testis and attaches higher on the spermatic cord. Intravaginal torsion occurs when the testicle rotates within the tunica vaginalis restricting arterial blood flow. Extravaginal torsion is more commonly seen in neonates, but may also occur within the womb.
Presentation
The differential for scrotal pain with swelling includes testicular torsion, epididymitis/orchitis, and torsion of the testicular appendage. Torsion occurs from abnormal fixation of the testis within the tunica vaginalis permitting the testis to twist. This can occur with trauma but is more often associated with periods of growth, ie – puberty. It may occur while sleeping due to unilateral cremaster contraction resulting in twisting of the testis. With torsion the patient may endorse abdominal pain in the lower quadrants. Pain may be constant or intermittent with no relation to position given that the injury is ischemic in nature. It becomes inflammatory once the testis is infarcted. Testicular torsion classically presents with acute unilateral pain and swelling, abnormal cremasteric reflex, high position of the testicle, horizontal lie, and nausea/vomiting. The cremaster reflex is elicited by lightly stroking the skin of the inner thigh causing the cremaster muscle to contract and elevate the testicle. The odds ratio for absence of a cremaster reflex has been reported from 4.8-27.8. A retrospective study reviewing the records of 90 hospitalized patients 18 years or younger found cremasteric reflex absent in all patients diagnosed with testicular torsion (LR+ 7.9 [4.3-14.5], LR- 0.04 [0.003-0.62]). However, it is important to note that the presence of a cremaster reflex does not rule out torsion. Prehn’s sign (of epididymitis) which is relief of pain with elevation of the testis, does not distinguish torsion and epididymitis. One cross section study of 120 patients revealed the Prehn’s sign was present in 91.3% of patients found to have spermatic cord torsion and 21.7% of those with epididymitis.
Diagnostics
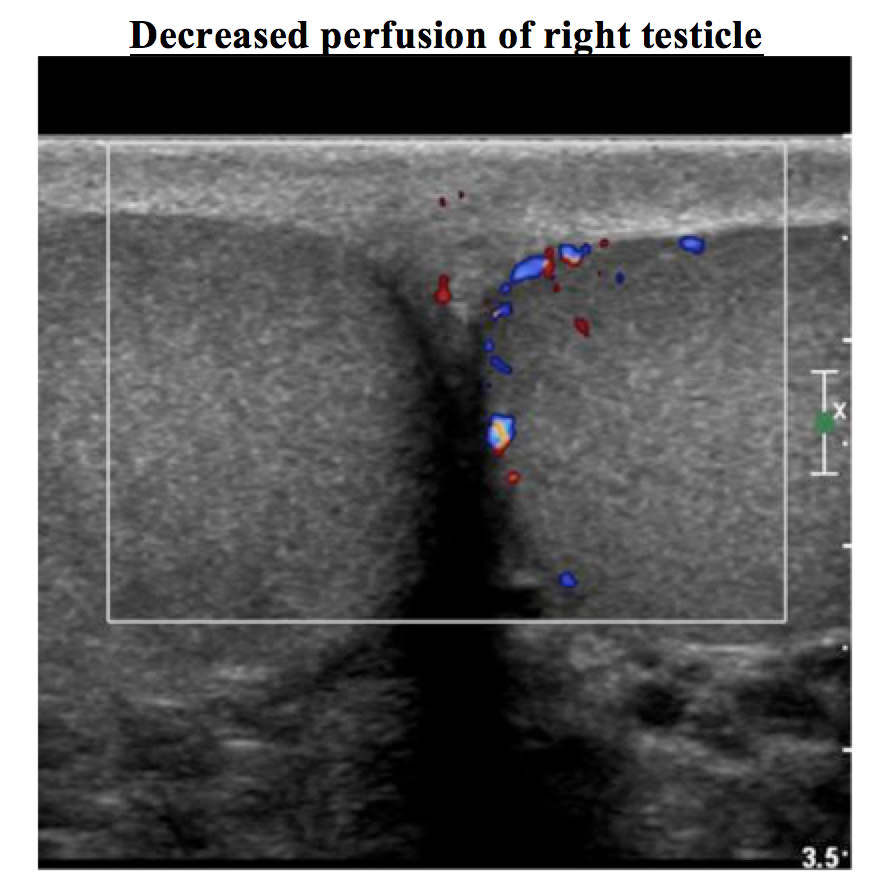
All patients with scrotal pain should be evaluated for torsion. If the diagnosis of torsion is certain, diagnostic evaluation should not delay definitive surgical management. Urinalysis may reveal pyuria, but this finding is not specific in the diagnosis of torsion. Doppler ultrasonography is regarded as the preferred study for diagnosis. It has a sensitivity ranging from 79 to 86% and a specificity of nearly 100%. Scintigraphy has sensitivities from 7 to 100% and specificity of 89 to 100%. These modalities are limited by availability and operator experience with interpretation. MRI is another option with a greater sensitivity (93%) and specificity (100%) but limited by availability and amount of time needed to obtain.
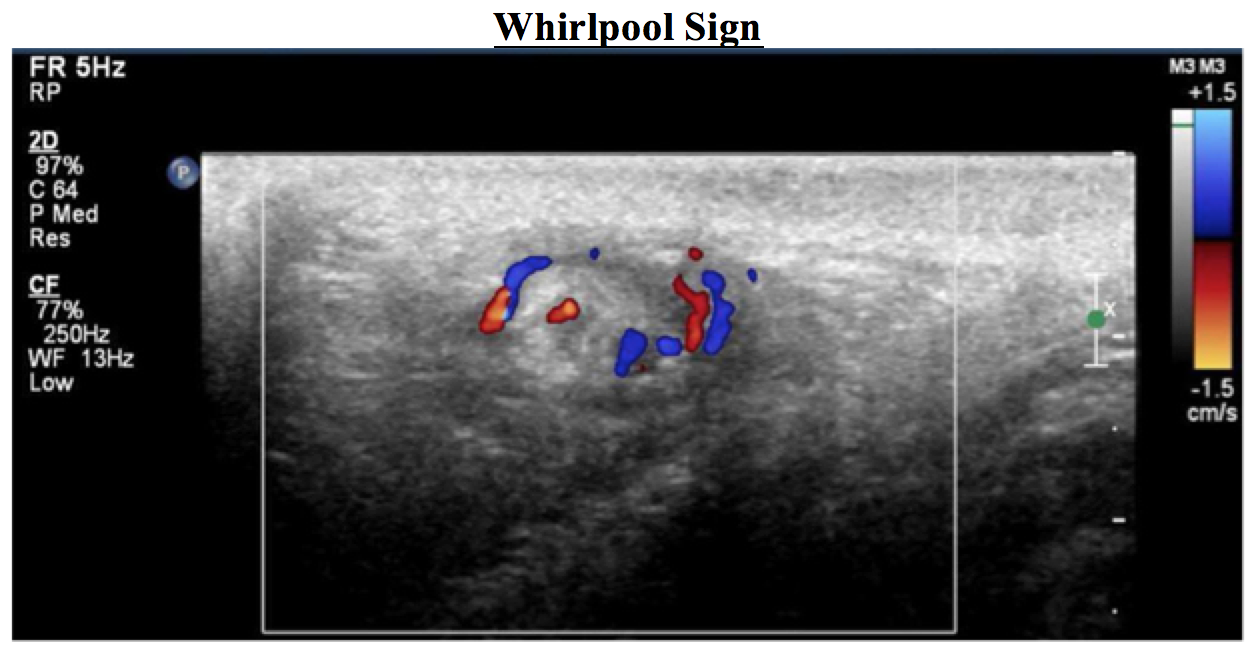
Most cases of torsion will not require imaging to confirm the diagnosis. Color Doppler ultrasound has the advantage of revealing scrotal anatomy and potentially confirming an alternate diagnosis. At times, ultrasound may be used to determine chance for salvage. When testicular arterial blood flow is lost with the additional finding of parenchymal heterogeneity of the testicular echotexture, there is roughly a 100% chance of testicular loss. In this instance, surgical intervention transitions to an elective procedure, with orchiectomy and contralateral fixation, rather than an urgent one. Color Doppler ultrasound is not always accurate and is subject to false negatives. High resolution ultrasonography has been employed for direct visualization of the twisting spermatic cord. This appears as a heterogeneous mass at the inguinal or paratesticular region and has been described as the “whirlpool sign”. High resolution ultrasonography was reported to have a sensitivity of 96% and specificity of 99% in this study. This is a fairly new concept but may lead to torsion ultrasound studies requiring evaluation of the spermatic cord up to the level of the internal ring in the future. When ultrasound is nondiagnostic and the presentation remains concerning, urology consultation is prudent in further decision making.
Management
Manual detorsion can be performed by rotating the testicles using the open book motion when viewing the testes from below, rotating medially to laterally. The intent should be to perform 540 degrees of rotation. The patient should be given adequate sedation and/or analgesia. Manual detorsion should only be attempted in instances when there is delay in definitive surgical management and the patient has had symptoms for less than 24 hours.
When a patient presents within 12 hours of initial symptoms, immediate surgical exploration is warranted. Detorsion is performed along with orchiopexy of the contralateral side to prevent recurrence. Nearly 40% of patients will have a bell clapper deformity on the contralateral side. Even with definitive management, one third of testes will be considered dead at the time of surgical exploration. These patients are given immediate orchiectomy. Salvaged testes may atrophy after definitive management and resolution of symptoms. There is also possibility of injury to the contralateral testis.
Torsion of the testicular appendage
A less time-sensitive disease with similar presentation is that due to torsion of the testicular appendage. There are four appendages with no physiological function – appendix testis, appendix epididymis, paradidymis, and vas aberrans. The appendix testis is responsible for 92% of testicular appendage torsion with the appendix epididymis accounting for the remainder. These presentations are often prepubertal. Patients will present with sudden onset pain (more moderate in severity) and located midline in the scrotum. A “blue dot sign” is considered pathognomonic. This is an area less than 3mm with a pale bluish discoloration present on the scrotum at the superior pole caused by the cyanotic appendage beneath the scrotal wall. It is only present in approximately 25% of cases. Diagnosis can be confirmed with radioisotope scan or color Doppler ultrasound. There will be increased or normal flow on ultrasound. Treatment relies on supportive care with analgesia and scrotal support. The appendage autoamputates in roughly a week.
Pearls
- Testicular torsion is the most common cause of testicular pain occurring in 1/4000 males under 25 years of age; patients with a Bell clapper deformity are more susceptible.
- Presentation is key with patients reporting severe and sudden pain associated with swelling and tenderness.
- An absent cremaster reflex is the most sensitive finding but its presence does not completely rule out torsion.
- Testicular torsion is traditionally diagnosed with ultrasound which will reveal an enlarged testicle, increased echogenicity, and decreased Doppler flow compared to the contralateral testicle.
- Emergent urology consultation is indicated in order to salvage the testicle; salvage rates are as high as 90% in the first 6 hours, dropping to 20% after 24 hours.
- Manual detorsion should only be attempted if surgical intervention is delayed.
- Torsion of the testicular appendage has a similar presentation but only requires supportive care. It can be confirmed with physical diagnosis and ultrasound.
References / Further Reading
– Crawford, Paul, and Justin A. Crop. “Evaluation of scrotal masses.” American family physician 89.9 (2014).
– DaJusta, Daniel G., et al. “Contemporary review of testicular torsion: new concepts, emerging technologies and potential therapeutics.” Journal of pediatric urology 9.6 (2013): 723-730. 3
– Gordhan, Chirag G., and Hossein Sadeghi-Nejad. “Scrotal pain: evaluation and management.” Korean journal of urology 56.1 (2015): 3-11.
– McCollough, Maureen, and Ghazala Q. Sharieff. “Genitourinary and renal tract disorders.” Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, Pa: Mosby Elsevier (2009).
– Nicks, Bret A., and David E. Manthey. “Chapter 96. Male Genital Problems.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. Eds. Judith E. Tintinalli, et al. New York, NY: McGraw-Hill, 2011
– Sharp, Victoria J., Kathleen Kieran, and Angela M. Arlen. “Testicular torsion: diagnosis, evaluation, and management.” American family physician 88.12 (2013).
– Schmitz, David, and Sarah Safranek. “How useful is a physical exam in diagnosing testicular torsion?” Clinical Inquiries, 2009 (MU) (2009).
– Yin, Shan, and Jennifer L. Trainor. “Diagnosis and management of testicular torsion, torsion of the appendix testis, and epididymitis.” Clinical Pediatric Emergency Medicine 10.1 (2009): 38-44.





1 thought on “Testicular Torsion: Pearls and Pitfalls”
Pingback: Testicular Torsion: A Diagnostic Pathway | Emergency Medicine Cases