Author: Francesca Civitarese, DO (EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit, EM Resident at SAUSHEC, USAF)
As emergency medicine physicians, we pride ourselves on being specialists in managing the emergent airway. We are expected to perform in the most adverse circumstances, artfully managing the dirty airway, the bloody airway, the mangled airway, the obstructed airway, the burned airway, the swollen airway, the airway in someone who can’t lie flat, the rapidly changing airway, the airway needed in 2 minutes or less. Our airways are grimy. They often aren’t the pretty, sterile, controlled intubations that so many of us trained on initially. By securing an airway, we ultimately can save a life.
How do we initially assess the airway? There are several mnemonics presented in emergency medicine texts to reference when initially assessing a patient who needs an airway. Often, in the emergency room, the patient needs to be assessed quickly, and the tools below will help you anticipate potential “badness”. The quick and dirty way to risk stratify your patient’s airway:
MOANS – difficult BVM
M: mask seal. Won’t be that great in someone with a sweaty, slimy face. Won’t be great with facial deformities, patients without teeth, or patients with a thick beard. To help with a beard seal, you can sometimes use jelly lubricant to create a better face-to-mask seal, but be careful with this as it may make jaw thrust difficult and grip on the face harder.
O: obesity. The bigger the patient, the harder to bag. Obese patients have many things working against them, both with increased pressure on the neck from excess tissue, increased thoracic pressure from chest tissue, and difficulty moving the diaphragm against a large pannus. Also included in this category are the pregnant patient and those with compressive issues affecting the neck such as tumors, hematomas, angioedema, and neck swelling.
A: age. This becomes a factor in both the very old and very young. Older patients lose muscle tone and have more advanced arthritis or sclerosis/kyphosis. The young tend to have larger occiputs and heads in general, and less muscle tone/support to maintain the upper airway independently.
N: no teeth. Causes a “caving in” of the face, making it difficult to obtain an adequate seal. Leave dentures in place while bagging the patient if you can, and remove just prior to intubation.
S: stiff lungs. This includes the COPD’er, the asthmatic, the sarcoid, the pulmonary hypertension patient, or the patient with upper airway obstruction.
LEMON – difficult laryngoscopy
L (Look externally): particularly taking note of the following => the obese patient, the agitated patient, patients with small mouth, small mandible, big tongue, large teeth, dentures, short neck, beards or evidence of facial trauma/facial fractures that may make BVM difficult.
E (evaluate the 3-3-2 rule): this will give you a rough guideline to predict whether your patient is able to adequately open the mouth, and to estimate the location of the hyoid bone, base of the tongue, and the top of the larynx at the thyroid notch.
- Essentially you assess whether you can fit three fingers, lined up vertically, inside the patient’s mouth. This is the first “3”.
- Next, assess whether the distance from the tip of the chin to the neck is about 3 finger-breadths, the second “3” which indicates the posterior limit of the tongue.
- Finally, the distance between the base of the neck and the thyroid notch should be about 2 finger-breadths. This location will roughly estimate the location of the glottis in relation to the tongue, identifying the entrance to the larynx. If this length is more than 2 finger-breadths, the larynx may be difficult to access or visualize.
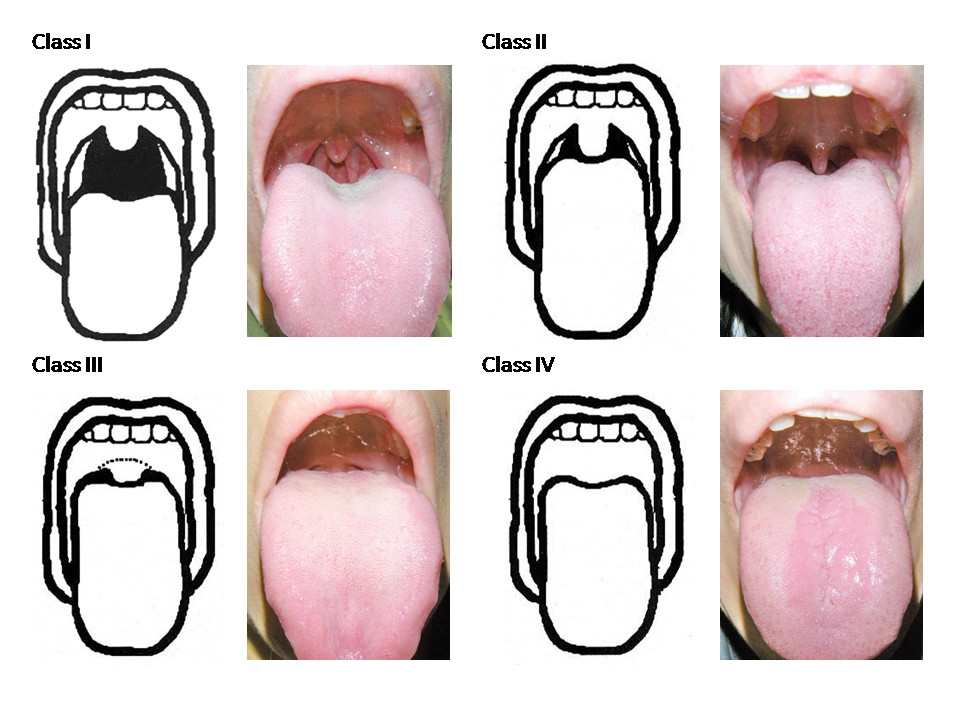
M (Mallampati Score): essentially giving you an external assessment tool about the patient’s ability to open their mouth, their tongue size, and the ability to visualize posterior pharynx structural landmarks. It should be assessed ideally with the patient upright, mouth opened as wide as possible, and tongue protruding as far as possible. Class I and Class II (the two best views) have been associated with lower intubation failure rates.
O (obstruction/obesity): These two factors are indicative of higher risk intubations. The four warning signs of upper airway obstruction include muffled voice (hot potato), difficulty managing secretions or swallowing, stridor, or the dyspneic patient. True stridor has been estimated to indicate a reduction of the airway to approximately 50% of normal diameter. Obese patients can pose several different issues with regards to airway, particularly having larger necks, thus resulting in poor 3-3-2 scores and bad glottic views.
N (neck mobility): Positioning is crucial in obtaining an emergency airway. Being able to align the axis of the head, mouth, neck, and larynx is crucial. The patient who cannot extend the cervical spine (those with arthritis, those in cervical spine precautions, history of spinal fusions, a history of ankylosing spondylitis) obviously make any intubation more difficult, let alone in the emergency setting.
The Cormack-Lehane Views
These views are important when you actually attempt laryngoscopy or intubation of the patient. The views decline in awesomeness from I to IV.
Grade I views indicate that you can see the vocal cords, epiglottis, and the arytenoids clearly on laryngoscopy.
Grade II views are typically only of arytenoids and epiglottis, with perhaps a small sliver of cords in view.
Grade III views only visualize epiglottis.
Grade IV views indicate that no glottic structures are in view, and typically are associated with difficult or failed intubations.
The Two Minute Drill: How I Prep My Airways
Airway prep in an expedited fashion can be a lifesaver. Know like the back of your hand how to do this, and have a memorized sequence of events so you never miss anything. I recommend being able to do a “2 minute drill”, i.e. hurry up offense for this, and be able to prep EVERYTHING in less than 2 minutes on your own.
Never rely on someone else to get something ready for you, because the one time that you do, it won’t be ready. You can ask for help with set up, but always confirm that it’s done.
Often, 2 minutes is about as much warning as you’ll get for an emergent intubation and you never want to get caught with your pants down.
This is obviously open to interpretation and personal style. Here is the sequence I run through consistently when preparing for an emergency airway. It may seem tedious and long to read, but each step is quick, and cannot be missed.
- GET THE RT. Page respiratory for support/vent.
- ASK FOR TWO LINES. Tell your RNs that you are intubating, ask for TWO good IV lines (if possible), if not, place an IO. The reason for this is my “safety first” philosophy. If one line goes subcutaneous, and the meds aren’t being adequately delivered and the patient is only HALFWAY sedated, you have no way to rescue the airway attempt without a second access. If something goes wrong with the first line approach, you always want to have a back-up.
- ASK FOR THE MEDS. This is often a time-delay process. Ask early, and it will be at the bedside when you need it. Ask the RN to grab an RSI kit/intubation meds (this often takes time to grab meds and then draw them up), as well as post-intubation sedation meds (also typically takes time and can be disastrous if the patient wakes up while freshly intubated).
- SUCTION. Get your suction up and confirm that it is functioning. I often tuck this under the head of the bed on my right side (my dominant hand side), as your left hand will be holding the laryngoscope during the intubation. Know where the tubing and attachments are, and how to get them connected and working. This sounds simple, but in some facilities, you may have to set all of this up on your own. If you have your RT readily available, the ancillary staff can help with this part. Often, if there is vomit in the airway, blood clots, broken or avulsed teeth, or foreign bodies, suction may not cut it. Know where forceps are in your trauma bay, or have an alternative way to retrieve the obstruction in the airway in a hurry. You can also detach the Yankauer and attempt to use the tubing from the suction for the larger chunks or clots.
- GET THE O2. Have the bag/mask, non-rebreather, and a nasal cannula available, all attached to O2 (if you have a second oxygen tree around). Have all three… because you never know if you’ll have time to pre-oxygenate the patient before intubation, and it’s best to be prepared so that you can optimize your time to look for cords. This is another part of the action you can potentially turf to your RT, but again… know how to do it yourself.
- PROTECTION FROM VOMIT AND BLOOD. Put a face mask on with a shield. Just… trust me.
- THE TUBE. Have your ETT with stylet in place, tucked on the right side (or dominant hand side). If you like a “hockey stick bend” to your ETT, do it now. Remember, you may not always be able to (and certainly don’t have to) place the 8.0 tube in EVERYONE. Remember that you can always try a smaller caliber ETT, particularly in females first, if you think that the airway has narrow-potential. In reality, if needed, the ETT can be changed over a bougie later if a larger diameter ETT is desired.
- BLOW MY BALLOON UP. Get a 10cc syringe, test your balloon, then attach the syringe to the ETT.
- THE LARYNGOSCOPE. Have your handle and preferred blade, test that the light works from the handle and seat your blade in the handle to make sure it works. The worst is getting into the middle of an intubation and having to reload your handle (irritating) or discover the light isn’t adequate (also irritating).
- BACK UP PLANS. Prep your rescue airways (I prefer to always have two, and my go-tos are the bougie and the video laryngoscope). Often, I carry a scalpel in my front scrubs pocket “just in case” it turns into a failed airway situation requiring a surgical approach such as a bedside cricothyrotomy.
**remember, if you pick Glidescope as your rescue device, make sure yours is turned on, working, plugged in, and with Glidoscope stylet readily available. Obviously there are other options such as the various supraglottic devices, fiberoptics, changing the blade (mac to miller and vice versa), nasotracheal approaches, etc… but use what you are most comfortable with.
- CONFIRMATION OF MY TUBE. ETCO2 detector on the bed.
- GET READY FOR A SUPERSIZED PATIENT. Have ramping blankets just in case your patient happens to be obese or have a difficult airway.
- STUFF TO HELP WITH BVM. Know where you have your oral/nasal airways. Often, BVM can be difficult with a patient who is sedated, obese, diaphoretic, bleeding, no teeth, etc, and an oral airway can potentially facilitate bagging and ventilation prior to successful intubation.
The best clinicians I’ve worked with were always prepared for the easy, “first pass” airway, but also for the potential difficult intubation in each patient. Part of this preparation will be recognizing the sphincter-tighteners. The airways that even the experts at airway cringe at a little. The ones you pee your pants over. The ones you hear in myths and legends. These airways, my friends, are where heroes are made.
And so, I humbly present some of them to you here, with why they are scary, and how to manage them.
The Bloody Airway: The Trauma Airway and the GI bleeder
You walk in and your patient’s airway is full of blood. Just suction right?
Trauma
The trauma airway is particularly cool in that it can present mangled, bloodied, or requiring various alternative intubation/airway management methods to the routine direct laryngoscopy approach.
THE IMMOBILIZED TRAUMA PATIENT
Trauma patients often will present in cervical spine immobilization and on a backboard.
Why is this a scary airway?
This severely limits the range of motion of the neck and therefore the ability of the physician to line up the “anatomical stars” of geometric axes to visualize cords, particularly with direct laryngoscopy. It is important in these cases to minimize movement of the C-spine, as initial information about the trauma patient requiring an airway is often quite limited, placing them at high risk for potential C-spine injury. To maintain order in the chaos, think of the immobilized airway in a step-wise fashion.
PLAN OF ATTACK
Step 1: determine if the patient needs to be intubated.
Step 2: look at MOANS or LEMON.
Step 3: designate a helper. Find someone who knows how to maintain in-line stabilization.
Step 4: airway prep yourself and call out meds to your nurses.
Step 5: tell the team you are removing the C-collar temporarily to help secure the airway. This prevents some other random overeager, overachiever from moving the patient while they are in a vulnerable position with the collar off.
Step 6: remove C-collar and in-line stabilize.
Step 7: become a hero by intubating the immobilized trauma patient.
Some tips and tricks for the immobilized patient:
–Strict immobilization is key. Find someone who knows what they are doing. By removing the cervical collar, you are enabling greater range of motion of the mandible and improving jaw opening, but are NOT doing it to change the motion of the cervical spine. You should not “crank” back on the head to get your views. Keep your motions with laryngoscope slow and controlled, with awareness of potential C-spine movements.
The in-line immobilization can be enhanced with instruction from the head of the bed (i.e. you). Have your helper, buddy stand facing you with their back to the feet of the patient and face towards the head. At the head of the bed, secure the patient’s C-spine while doing the “hand off” between you and your helper. Then, after loosening the front of the collar, the helper should anchor both elbows on either side of the patient’s head at the shoulders. Then, to immobilize, press both forearms and hands together, creating a steady, human arm splint. There should be secure pressure, but no traction or rotational component from the helper.
Sedation Recommendation. Given that immobilization is so important, and because you need to be able to control the gentle intubation of the patient, in someone who may be disoriented or agitated, neuromuscular blockade is recommended, and RSI is still the go-to in these scenarios.
THE FACIAL TRAUMA PATIENT
Why is this a scary airway?
The airway in the patient with facial trauma can be tricky, depending on where the trauma is. It can directly block your approach, change your approach, or create a difficult airway scenario. The structures for 4 out of the 5 senses are in this area, and damage to the face can result in long-term impairment.
The interesting thing about even isolated facial fractures, is that they often accompany other badness, such as cervical spine injuries in up to 8% of patients, with this estimate rising to up to 10% with more serious injury, and also translating to intracranial involvement in 65-89%.1
There are some areas of the face that have predictable associated injury patterns.
Unilateral mandibular fractures are associated with upper C-spine injuries.
Unilateral midface fractures are associated with basilar skull fracture and severe ICH.
Upper face injuries are associated with mid/lower C-spine injuries, increased mortality rates, and severe ICH. Bilateral midface fractures are associated with basilar skull injuries, and death.1
As an airway technician, you have to be acutely aware of the “crumple zone”.
The Crumple Zone of the face is essentially the midface (i.e. nose/orbits/cheeks/upper mandible). It’s a lot weaker than the rest of the tougher/thicker bones of the front of the face, and prone to breakage; however, it provides a buffer between the site of injury and brain matter. If the crumple zone is trashed and/or completely obscuring access to the airway, you may have to just go ahead and cric the patient. This is one of the scenarios that a “cric first, ask questions later” approach is reasonable.2
PLAN OF ATTACK
If you can access the oropharynx, and the issue is blood or foreign bodies that can be easily removed, then use suction aggressively and proceed with standard oral intubation techniques using RSI.
You may have to use other measures to control upper airway (read: nasal) bleeding such as packing the nose or direct pressure. If the bleed is brisk, consider that the maxillary artery end branches at the pterygopalatine fossa may be involved or even the common carotid at the skull base. You can use anterior and posterior packing methods in an attempt to tamponade this while you obtain your airway, but do so with care.2
As a rule of thumb, typically you should not do a naso-tracheal intubation in the patient with significant facial injuries, as it is often more difficult, anatomy can be disrupted resulting in secondary injury such as airway damage, disruption of hematoma, precipitation of swelling, or potential to disrupt the cribriform plate. You run the risk of worsening the airway by going in blind.
So, when do you use nasotracheal intubation, you may ask? When there is no contraindication and the patient is a perceived difficult airway whom RSI may be less than desirable. For a patient to be a candidate for a trial of nasotracheal intubation, the practitioner must feel that they have adequate access to the nose, nasopharynx, and oropharynx. Also, they should consider if the patient may tolerate awake intubation techniques.
Cricothyrotomy, or tracheostomy, prior to cervical spine clearance, may be required if the entire crumple zone and laryngeal inlet is damaged and is obscuring the airway.3, 4
Le Fort Fractures
Le Fort Fractures were originally classified by a French Surgeon, who decided to drop cannon balls on the faces of cadaver heads to see the potential break patterns in the crumple zone. Kind of like a bad car-dummy commercial.
Essentially there are three types of LeFort Fractures.
Le Fort I
Fracture line separates the upper teeth from the face. It is a horizontal fracture line through the alveolar ridge that removes the palate from the maxillae
Le Fort II
Forms a “pyramid” with the fracture line, with the upper teeth as the base of the pyramid and the fracture arch through the inferior orbital rim and nasal bones. If the infraorbital rims are intact, it EXCLUDES a Le Fort II. This type of fracture can be associated with infraorbital paresthesias due to the proximity of the fracture to the infraorbital foramen. Touch under the center of the patient’s eye/cheek to see if they perceive normal sensation here.
Le Fort III
The “loose face” syndrome, where the fracture line dislodges the midface from the rest of the person. Like the Le Fort II, the fracture line goes through the naso-frontal suture, maxillae, orbital walls. However, the fracture that distinguishes this from Le Fort II is the involvement of the zygomatic arches. If the zygomatic arches are intact, it cannot be a Le Fort III. Often, these fractures also involve the posterior aspect of the ethmoid and can be associated with CSF leakage.
Patients with Le Fort Fractures often can present in extremis and require emergent airway attention. Consider temporizing measures such as an LMA or transtracheal jet ventilation… while you get out your scalpel. They are more likely to require cricothyrotomy/emergency tracheostomy (estimated at 22% overall in one study).2,5
THE NECK TRAUMA PATIENT
The patient with blunt or penetrating neck trauma, or with obvious tracheal injury can be tricky. Also in this category are the strangulation patients.
Why is this a scary airway?
The potential for airway compromise and difficult intubation is high, particularly with airway obstruction (from swelling, hematoma, blood, subcutaneous air, excessive secretions), cervical spine fracture risk (more so in blunt neck injuries as opposed to penetrating), and the potential for spinal injuries. Even simple bag-valve mask use in these patients can worsen the airway by potentiating subcutaneous air spread through the fascial planes and distort the airway. In strangulation victims, be aware that they are at particularly high risk for progressive airway edema, blunt vascular, laryngeal, or esophageal injuries, as well as pulmonary edema and ARDS. Look for evidence of facial or neck petechiae, ligature marks or bruises, or subconjunctival hemorrhages.6
As a rule of thumb, if the penetrating object is still in the neck… do not remove it. It could potentially be providing temporary hemostasis to lacerated critical vessels/structures and you pulling it out can result in exsanguination.
Assess the airway by having the patient cough (for hemoptysis), swallow (for dysphagia) and speak (assessment of laryngeal function). These are cheap, quick, easy ways to assess for neck damage.6
Take Note of The Zones of the Neck
Penetrating and blunt injuries to the neck can be classified based on the zones. This gives you an anatomical reference to convey the location of the injury.
Broadly speaking:
Zone I: everything below the inferior border of the cricoid cartilage to the clavicles/sternal notch. Zones I and III injuries are difficult to access surgically, contain critical vessels and anatomical structures, and are often non-compressible, thus having higher mortality rates than zone II injuries.7-9
Zone II: between the cricoid cartilage and angle of the mandible, in between I and III. Generally speaking, Zone II injuries are the most common and the easiest to access surgically, and also interestingly, easiest to achieve hemostasis.7-9
Zone III: above the angle of the mandible to the skull base.7-9
Neck trauma in the anterior aspect of the neck and lateral aspect of the neck in front of the sternocleidomastoid muscles carries higher risk for airway compromise due to the proximity of the larynx, trachea, laryngeal nerves, and major blood vessels.7-9,12
PLAN OF ATTACK
Approach to airway management
Airway management in neck injuries varies widely and is controversial. There is not an agreed upon “right way” to manage these airways. To make a long story short, early attempts at orotracheal intubation should be explored, and if failed, heroic techniques used.
INDICATION FOR INTUBATION
Eggen et al. defined criteria for emergent intubation: respiratory distress, airway compromise from blood or secretions, subcutaneous emphysema, tracheal shift, or change in mental status.6,10
Eggen, et al.10 did a review attempting to create criteria for penetrating neck wound patients regarding airway management for a “when to intubate” guideline. They performed an 8-year retrospective chart review of 114 patients and categorized them into 3 groups, with group I being “urgent”, group II being “elective”, and group III with no intubation. Urgent intubations were described as those with airway compromise from blood or secretions, extensive subcutaneous emphysema, tracheal shift, or altered mental status. Thirty total patients met criteria for urgent intubations, 25 of which were successfully intubated in the ED, 4 of whom were never intubated, and the fifth who was not intubated initially required an emergent trach in the OR. There were no patients in this review requiring an emergent airway procedure who did NOT meet the initial “urgent” category requirements.10
They proposed that plain films of the neck, obtained in 41 patients, were found to have findings indicative of airway compromise in 39%. These findings included prevertebral swelling/air, tracheal or laryngeal shift, or encroachment of the air column. They proposed that Group II and Group III patients’ airway management could be conservative (ie no intubation) if they had negative plain films of the neck, no indication for surgical exploration, and who did not fit into the “urgent” category.10
RECOMMENDED MANAGEMENT:
Many authors subscribe to the early management in the trauma patient = easier management. Potentially, the neck trauma airway can become progressively more difficult, i.e. with expanding hematoma/swelling/subcutaneous air, etc. This can all lead to airway narrowing and the risk that the patient will develop acute airway obstruction.
To head this off at the pass, many practitioners tend to err on the side of caution, with intubation in both blunt and penetrating neck injury earlier as opposed to later. There are no current agreed upon guidelines on “when to intubate”, or how to intubate, so obviously clinical judgment is in play here. As of now, it seems that the general consensus is that patients should be intubated sooner rather than later, before the patient clinically deteriorates and needs an emergent intubation with a distorted airway scenario.
For our purposes, anyone arriving with instability (either from an airway perspective with evidence of progressive or impending airway obstruction from subcutaneous emphysema or expanding hematoma, or instability from a hemodynamic standpoint from penetrating wounds) should be intubated.
Suggested by Walls, intubation should be performed in all GSWs to the neck regardless of evidence of platysma violation, as well as all stab wounds that violate platysma or show respiratory/vascular compromise. Ideally, an awake intubation with light IV sedation should be attempted if the patient can tolerate it; however, if the patient is agitated, combative, etc., RSI should be attempted instead.11
Several approaches to the airway have been proposed, including awake fiberoptic intubation, RSI fiberoptic intubation, retrograde intubation, standard RSI orotracheal approach, or awake orotracheal approaches, based on individual patient circumstances, clinician experience, and urgency. The surgical airway is always an option.
A word of caution regarding surgical airways: they represent a failed airway scenario. Cricothyrotomy is still the go-to rescue airway and relatively contraindicated in the scenario of expanding hematoma over the cricothyroid membrane. Remember that emergent crics may be performed if the injury is above the cricothyroid membrane, or in the crashing patient regardless of location of suspected injury. It is contraindicated in the patient whom the location of the injury is unknown, as it can result in complete disruption of the airway in cases of laryngotracheal dissociation. In neck-trauma patients, tracheostomy at least 1 tracheal ring below the injury is a route that is more often chosen.12, 13
If the airway is obviously exposed and the hole in the trachea is evident, you can sometimes just put the ET tube into the existing hole or wound site. Grab the distal segment with a towel clip to stabilize the trachea, and then directly intubate through the wound.
If you have time, comfort level, and the resources, fiberoptics are ideal. The benefit of awake fiberoptic intubations (either orotracheal or nasotracheal) is that you can visualize the damage to the airway, look for mucosal tears, and potentially place the ETT distal to the injury. ETT cuff should be inflated distal to any evident mucosal injury to prevent worsening of the defect and potential airway compromise. Ideally with topical anesthesia methods, you can intubate the cooperative, relatively stable patient with a neck injury this way. Again, this is highly dependent on the clinician’s comfort level and availability of these resources.
The preferred initial method in the ED seems to be orotracheal intubation, with RSI having strong success rates, direct cord visualization, and few complications. If you are concerned that the patient cannot be bagged (i.e. beard, obesity, developing airway distortion) try to avoid paralysis on the first attempt. Ketamine (1-2mg/kg slow IVP) is a great option for sedation in these patients that you don’t want to paralyze, as it preserves respiratory drive. If you have time, try to put nebulized 4% lidocaine in the mix as well to facilitate your attempt.6 You can also use versed (0.05mg/kg) or fentanyl (1-2mcg/kg) for this purpose.
In a retrospective study of 748 patients with penetrating neck injuries evaluated in the ED, 11% (82) required urgent airway management, with 42 undergoing successful orotracheal intubation with 100% success rate, with 39 of them being with RSI as the initial method. Interestingly, RSI was successful in this study even after fiberoptic intubation failures in 3 patients. Thus, more than 2/3 of patients in this study with critical airways were successfully intubated with RSI.14
Universally speaking, it is believed that blind intubation isn’t a great plan with neck trauma because you can worsen the injury, hypothetically dislodge clots, or precipitate complete airway obstruction from what may have only been partial obstruction initially. However, a recent small study in 2004 showed a 90% success rate in prehospital blind nasotracheal intubations after failed orotracheal attempts by EMS staff, with similar mortality rates to orotracheally intubated patients.15
An interesting and often undiagnosed injury to the neck initially is the “clothesline” in which there is a mechanism of blunt trauma to the neck so severe that it caused a complete tracheal transection. Of note, RSI is dangerous in these patients because it causes loss of respiratory muscle tone and can result in misalignment of the two segments of the trachea, which can make ventilation and orotracheal intubation difficult, if not impossible.6
GI Bleed Airway
Acute upper GI bleeds, while being life-threatening from a hemodynamic perspective, can also create a critical airway scenario.
Upper GI bleeds are often divided into variceal (esophageal or gastric varices) and non-variceal etiologies.
Non-variceal bleeds include peptic ulcers (gastric and duodenal), Mallory-Weiss tears, erosive esophagitis, arteriovenous malformations, as well as UGI tumors and malignancies, and constitute the majority of upper GI bleed presentations (approx. 80-90%).16,17 Peptic ulcer, specifically posterior duodenal ulcer, is the most frequent cause of major, life-threatening upper GI bleeding, as erosion of the ulcer through to an underlying artery such as the gastroduodenal artery or gastric arteries on the lesser curve has the capability of producing severe hemorrhage, dependent on the size of the defect and diameter of the artery.18
Variceal hemorrhages occur at an annual rate of 5-15% and depend largely on the size of the varices. There is a 20% mortality rate at 6 weeks following a variceal bleeding event.17,19
Why is this a scary airway?
Airway protection in the upper GI bleed patient is paramount, in that the patient with brisk bleeding is at high risk for aspiration of blood or gastric contents. Cardiopulmonary events are responsible for adverse events in 23-50% of patients with upper GI bleeds, and 50-60% of deaths.20,21
PLAN OF ATTACK
Intubation is the preferred method for airway protection during EGD, which ultimately provides definitive management and diagnosis for the upper GI bleeder. There does not appear to be widespread, comprehensive prospective studies regarding safety/efficacy of intubation in these cases, or even consensus amongst clinicians regarding endotracheal intubation in upper GI bleeds.22
In a retrospective study, Rudolph, et al. examined outcomes from ICU admitted patients with upper GI bleeding from 1988 (n=101) (where intubation was rarely performed prophylactically prior to EGD) were compared with patients from 1992 (n=119), where intubation was commonplace.23 Intubation use increased significantly from 1988 (3%) to 1992 (15.1%). The authors concluded that intubation for airway protection may have prevented the rare fatal massive aspiration episode but did not significantly decrease the high frequency of acquired pneumonia (12.9% vs 15.1%}, other cardiopulmonary events (5% vs 3.4%), number of ICU days (7.1d vs 6.4d), or overall mortality (15.9% vs 11.8%).23
Amongst experts in the field of upper GI bleeding and endoscopy, only 20-25% believe unstable vital signs necessitate intubation, and only 60% believe that ongoing hematemesis is an indication. Additionally, intubation for GIB with altered mental status only reached 73%. Intubation for the GI bleed patient with poor respiratory status, defined as CO2 retention or pulse oximetry <90%, was recommended by 60-75%. For the uncooperative patient, intubation was recommended by 67-80%.
Many experts stated that instead of intubation for airway protection, they would instead use a large bore suction catheter to remove clots/blood from potentially being aspirated, as well as an “overtube” during the endoscopic procedure as opposed to an ETT. Some advocated for prophylactic intubation in patients with severe GI bleeding and a history of cirrhosis, stating that in their facility it decreased incidence of pulmonary complications.22,23
In a retrospective study of ICU patients who underwent endoscopy for UGI bleeds, 53 had elective prophylactic intubation, and were compared with non-intubated, matched controls. The incidence of cardiopulmonary complications, both ICU and hospital length of stay, as well as hospital mortality were similar in both groups, leading the researchers to conclude that complications following endoscopy for UGI bleed are rare and not significantly affected by prophylactic intubations. 24
From an emergency medicine perspective, if the patient is unstable and not protecting the airway, follow your principles of A, B, C.
Intubate the patient if you feel that they are high risk for aspiration and not able to maintain a patent airway.
It would be generally acceptable to intubate the patient who:
- is having massive hematemesis
- who is hemodynamically unstable
- who at baseline has intrinsic lung disease
- who has low pulse oximetry (which could indicate that they have already aspirated)
- the cirrhotic patient
RSI can be used for this purpose (with lots of suction). There are currently no clinical guidelines regarding airway approach and will largely be case-based and per provider preference. Additionally, during your set up of the airway, instead of the standard suction device, attach a larger bore suction catheter or remove the Yankauer if you encounter clots that are not able to be suctioned and use the tubing instead as a suction device.
The Obstructed Airway: Angioedema and Deep Space Infections
Angioedema
Generally speaking there are two types of angioedema, the “allergic” variety and the “hereditary” variety, although it can also be idiopathic, related to antibiotics or food exposures/allergies. Angioedema can manifest as abrupt onset, non-pruritic, non-pitting painless swelling anywhere in the body, but the location of primary concern for the EM doctor is the airway. Swelling in angioedema is a result of extravasation of intravascular fluid into the reticular dermis, subcutaneous, and submucosal spaces, secondary to diffuse vasodilation and increased vascular permeability.25
Causes and pathology of angioedema are still being researched, and often controversial.
ALLERGIC FORM
The most commonly accepted explanation for the cause of the allergic form of angioedema is often related to the activation of IgE-mediated mast cells or basophils in response to a trigger, which then release histamine and bradykinin, which ultimately results in inflammatory changes. Other inflammatory markers such as IgA, IgM, and IgG mediators can also cause reactions resulting in angioedema.26
Triggers for allergic angioedema can include drugs/chemicals, food, inhalants, parasitic infections.26 There are also some chemical-releasers of histamine, including morphine/codeine and iodinated contrast.26
ACEI Angioedema
One of the most common presentations of angioedema in the ED is the known adverse effect to angiotensin converting enzyme inhibitors (ACE Inhibitors), which are a class of medications often prescribed for hypertension. In the largest observational study reviewed for this article, incidence was highest amongst African Americans, older patients, those with chronic heart failure or CAD, and females.27
Exact pathophysiology of angioedema reactions in ACEI use is still being debated. It can happen months to years after ACEI initiation, and has not been found to be dose-dependent or related.28
It is thought that the mechanism behind angioedema in ACEI use is because these agents cause a decrease in angiotensin converting enzyme, which is responsible for both blocking angiotensin 1 to angiotensin 2 breakdown, as well as blocking the breakdown of bradykinin. This affects the kinin-kallikrein system, resulting in vasodilation due to the accumulation of bradykinin. Incidence of angioedema in patients using these medications has been estimated anywhere from 0.1% to 1.0% of all users.28,29
Hereditary angioedema, inherited in a heterozygous, autosomal dominant fashion, is thought to be complement-activated. Hereditary angioedema is attributed to deficiency of (or dysfunction of) C1 esterase inhibitor. The hereditary angioedema patients often do not have urticarial lesions, and more often present with family history, peripheral edema, or abdominal colic symptoms.30,31 This form of angioedema can also occur in response to or worsen during times of stress, infection, puberty, menstruation, pregnancy, hormone replacement therapy, or oral contraceptive use.32 Reactions can often occur following trauma, which can be as minor as simple dental procedures.
To get a little scientific and fancy: the rationale behind these activations is that the fibrinolytic pathway is activated by natural clotting cascade activation after trauma/surgical procedures, which results in plasmin production, which then activates C1. The C1 proenzyme, once activated, often by an antigen/antibody complex, then binds to C1 esterase. The C1-INH is responsible for preventing further activation of the complement cascade, and is basically a regulator of the response. If this regulator is missing, or dysfunctional, it results in excess cleavage of C4 and C2 (by the active form of C1 that has gone unchecked). The consequences of this excess cleavage result in increased capillary and vascular permeability and increased immune response.33
There are two types of hereditary angioedema, Type I designating those patients with low C1-INH antigenic protein levels and low activity (approx 85%), and type II with normal levels of the protein but low C1-INH function (approx. 15%). A third type has also been described with normal C1-INH levels and function.32
Why is this a scary airway?
Airway involvement in these patients classically manifests as asymmetric swelling of the lips, face, tongue, oropharynx, hypopharynx, or larynx, is well-defined, and not in gravity-dependent locations. In general, it lasts about 24-48 hours. 34 Up to 50% of patients will present with urticaria.35 Patients can also present with symptoms including eyelid or facial swelling, swelling at the floor of the mouth or submandibular space, shortness of breath, stridor, voice changes, inability to manage secretions, or pain with swallowing.36,37
MEDICAL PLAN OF ATTACK
Have a very low threshold for intubation/airway management. Some medical interventions may improve the airway or temporize the patient until definitive management can be achieved (briefly reviewed below).
Hereditary Angioedema
It is recommended that patients with known hereditary angioedema who are undergoing surgical procedures should have plasma derived (pd) C1-INH readily available, and in certain cases (such as major surgical procedures or in patients who have had previous reactions to minor procedures) actually undergo pre-treatment, 1 hour or less prior to surgery.
If pd C1-INH is unavailable, the patient can have pre-treatment with a limited course of Danazol, or stanozolol (or another attenuated anabolic androgen, which act to increase endogenous levels of C1 esterase inhibitor and C4 levels) as well as antifibrinolytic prophylaxis with tranexamic acid (which act to inhibit conversion of plasminogen to plasmin). Studies of efficacy for these therapies are limited and ongoing.32
Acute attacks should be treated as early as possible with plasma-derived C1-INH (pdC1INH), generally at a dose of 20 units per kilogram. They can be treated with fresh frozen plasma, which increases the C1 esterase inhibitor level, although FFP is not currently approved by the FDA for this indication.38-40
FFP can also be used in patients with ACEI-induced angioedema, with some studies showing efficacy in these patients as well.38,41,42
In Europe, other agents for therapy are available such as Icatibant, a bradykinin receptor blocker that is administered subcutaneously in 30mg doses. In the United States, Ecallantide is a kallikrein inhibitor approved for use in hereditary angioedema, also administered in 30mg subcutaneous doses.
Typically, patients presenting with angioedema warrant very low thresholds for airway intervention, as progressive edema can be life-threatening.43-46
Patients in the ED with the symptoms of angioedema will often receive steroids, epinephrine, and antihistamines, usually diphenhydramine (H1 blocker) as well as an H2 blocker. These interventions can be helpful in the “allergic” type of angioedema, but have not shown definitive benefits in angioedema relating to hereditary types or ACEI induced angioedema, which do not respond to steroids or antihistamines and only show transient benefits from epinephrine.32, 43-46
In ACEI related cases or hereditary angioedema, typical medial therapy as described above is still being researched, and efficacy is debatable. Although data is limited, there have not been many adverse outcomes documented with regards to administration of these medications in patients with ACEI angioedema or hereditary angioedema.47
In some cases, ED observation as opposed to definitive airway management may be preferable. These cases are typically milder, and don’t carry the “red flag” symptoms of deeper airway involvement or compromise like stridor, voice changes, drooling, etc., but are more isolated to swelling of the face or lips.48,49
In a retrospective study of 177 patients investigating risk factors to progression of the airway in angioedema patients, patients with isolated lip or facial edema were safely observed for a period of time in the ED, and ultimately deemed stable for discharge. 46
In the literature reviewed, observation periods of 4-8 hours in patients with isolated symptomatology who were discharged were not associated with adverse events. 50
In a study attempting to predict airway compromise in angioedema, a retrospective analysis was conducted of 93 episodes of angioedema, which included a classification system for severity and disposition data. They found that patients ultimately dispositioned to the ICU for observation had higher rates of voice changes, hoarseness, dyspnea, and associated rash. Those requiring airway intervention also had these characteristics, as well as stridor. They proposed that patients with facial rash/edema/lip edema (stage I) and soft palate edema (stage II) could be potentially treated as outpatients or on the ward. Patients with lingual edema (stage III) typically required ICU admission and observation, and Stage III and IV (laryngeal edema) patients more often required airway intervention.51
In another study, with 228 ED visits for ACEI related angioedema, patients were grouped into categories based on areas of involvement, with Type I being lip/anterior tongue, type 2 including floor of the mouth, palate, or oropharyngeal edema, and Type 3 with laryngeal or hypopharyngeal edema. It was found that Type I was the most common (63.5% of all patients), and most frequently discharged from the ED (71.3%). Patients with Type III edema were more likely to be intubated (approx. 34%). Approximately 10% of the patients in the study required intubation, all within the first 12 hours of presentation to the ED.44
Fiberoptics in the ED
If you have access to this resource, direct visualization of the degree of potential laryngeal edema can be helpful. In a study by Bentsianov, et al., patients who were deemed to initially have a normal larynx in fiberoptic investigation did not progress to requiring intubation.50
INTUBATION in ANGIOEDEMA
Airway intervention in angioedema is typically a case-by-case call, with no set guidelines on when to intervene. Some studies have attempted to characterize necessity of definitive airway placement based on locations of swelling, with swelling at the hypo-pharynx, base of the tongue, anterior oral tongue, or larynx associated with higher rates of intubation.43-46, 51
If you do decide to intubate the patient, and you have available advanced airway specialists in your hospital, they should be called. These “advanced airway” specialists can be another ED physician to help, but also consider other available resources such as anesthesia, general surgery, or ENT.
In the ED, if you have access to anesthesia for intubation in a more controlled setting, and the patient can be/has time to be/is not in too much extremis to be transferred there, this may be the time to swallow your airway pride, rally the troops, and engage your anesthesia and surgical colleagues for an intubation in the OR setting.
If this isn’t possible, pull on your big boy/girl panties and make sure you’re prepared for battle.
- Prior to intubation, examine the airway. These airways can be precarious, and prolonged manipulation can precipitate increases in swelling.
- Mark the neck in the “just in case” failed airway scenario, in the event that you have to emergently progress to a surgical airway.
- Prepare everything at the bedside, including multiple back-up airway options with video laryngoscopy if available, bougie, and supraglottic devices, and also always including a surgical option. Avoid manipulation of the airway or oropharynx until everything is prepared.
- Preoxygenate the patient as much as possible. Administration of heliox (80% helium and 20% oxygen), which has less density and less turbulent flow than oxygen, may help you obtain acceptable oxygen saturations even through the very tight or nearly occluded airway.52
- Try not to transfer the patient with angioedema anywhere, even for a short distance, without a secured airway, (or without a babysitter like yourself, a resident, etc. armed with intubation meds/airway equipment, who can rapidly intubate the patient if needed) as they are unpredictable and can be rapidly progressive.52 Be wary that the external exam may not be indicative of the degree of swelling in the hypopharynx or laryngeal structures, and a somewhat benign external exam does not mean that there isn’t swelling at the level of the airway.52 Similarly speaking, profound lip swelling can be quite impressive and intimidating on initial exam, but does not always correlate with hypopharynx or laryngeal edema. In all cases, err on the side of caution. 52
In the literature reviewed, blind techniques are contraindicated and can potentiate dynamic airway changes that can occlude the airway.52
Currently, consensus of the literature seems to recommend that if the resources are available, an awake airway exam with fiberoptics or flexible endoscopy should be performed, and if there is found to be severe base of the tongue edema or laryngeal edema, the preferred method for intubation is via fiberoptics in a controlled environment such as the operating room. If intubation must be completed in the ED, flexible endoscopy can serve as a conduit for intubation.52-54
There are some advantages to approaching these patients with awake techniques. Flexible endoscopy can be performed while awake, particularly if the patient is not yet in extremis. The patient, if able to be well anesthetized topically, can have the glottic structures visualized directly also by video laryngoscopy or direct laryngoscopy. Both techniques, if well visualized, enable to you to proceed immediately with intubation. Be aware that, in an irritated upper airway, administration of topical anesthetic or airway manipulation during the “awake look” can precipitate increases in swelling, so be prepared to rapidly convert to intubation or surgical airway techniques.
RSI techniques in these patients should be reserved for those that you are highly confident orotracheal intubation is likely to be successful, as well as confident that the patient can be bagged in the event of a failed orotracheal attempt.52 Alternatively, you can proceed with awake investigations, or primary cricothyrotomy, if the obstruction is suspected to be complete or rapidly progressive and the likelihood of orotracheal intubation/RSI success is low. Remember that these are rarely straightforward cases.
Disposition of the patient is also less straightforward. Some patients with isolated lip and facial swelling, as mentioned before, may be observed in the ED for a period of time to ensure there is no progression, and then discharged on a steroid taper with an H2 blocker for prevention of steroid-induced gastritis as well as prescriptions for diphenhydramine, and an epi-pen if allergy-related. Strong return precautions are essential!
Patients with swelling at the lips, inside of the mouth, or soft palate and related structures are the “on the fence” patients with regards to placement in the hospital. When in doubt, err on the side of ICU placement if you feel the swelling has progressed, but some of these patients may be appropriate for floor or ward monitoring after a period of observation in the ED.51
Patients with confirmed hypopharyngeal or laryngeal edema/swelling should be observed in an ICU setting. 51
Deep Space Infections
Deep space oral and neck infections are most commonly associated with dental infections, but also are found with adeno-tonsillar tissues, salivary glands, peritonsillar infections/abscesses, untreated tonsillitis or pharyngitis, and tuberculosis. They are polymicrobial, with group A strep, staph, peptostreptococcus, bacteroides, Fusobacterium, and other anaerobes being the most commonly cultured organisms.55,56
The most common presenting complaints in a retrospective study of 173 patients found to have deep space neck infections were pain, neck swelling, odynophagia, dysphagia, fever, dysphonia, trismus, ear pain, and shortness of breath.57 The most common involved site was the submandibular space, followed by peritonsillar, retropharyngeal, and parotid spaces.57
Ludwig’s angina, although infrequent, is a significant deep space neck infection for emergency medicine doctors. It is defined as a rapidly progressive, gangrenous, bilateral submandibular cellulitis or abscess with posterior displacement of the tongue, often seen in patients with poor dentition or dental infections. There should be involvement of the sublingual, submylohyoid, and submental spaces. It is an airway emergency because of the progressive lingual obstruction of the airway. The culprit teeth are most often the molars, particularly the 2nd and 3rd.57
Exam for Ludwig’s will reveal a thick-feeling, “woody” textured area of swelling in the submandibular space that feels tense to the practitioner. The floor of the mouth will be swollen and tender. The patient will also likely have enlarged cervical adenopathy. These infections can range from cellulitis to abscess and are most often relegated to the submandibular space, but can also be in other areas within the fascial planes of the neck, including the retropharyngeal tissues.
As with any space-occupying airway lesion, deep space neck infections can result in compromise that can present with dyspnea, tachypnea, stridor, dysphagia, odynophagia, vocal changes, ear pain, drooling, or mental status changes from hypoxia.
Why are these scary airways?
These infections can progress rapidly, with life-threatening complications including airway obstruction/total occlusion, descending mediastinitis, pneumonia, empyema, pericarditis, sepsis, and thrombosis of venous structures in the neck. Mortality can reach 40% with these complications.56,59
Patients may have limited neck mobility, laryngeal edema, or trismus, all of which can make airway management perilous and difficult to access with conventional laryngoscopy. They often present with “mass effect” from the infection, creating distorted airway anatomy, purulence or bleeding in the airway, and precarious, friable airway tissue. Rapid airway progression is common.
Remember too that these patients will be panicked, very ill, potentially already hypoxic, and can also have difficulty lying flat due to stridor. Induction and anesthesia choices are crucial in these patients, as there is no guarantee that you can a) oxygenate after you sedate the patient, or b) intubate the patient.
MEDICAL PLAN OF ATTACK
Treatment of these infections generally involves IV antibiotics, with coverage for gram positive and gram negative aerobic and anaerobic organisms. Often, this involves penicillin, or a 3rd gen cephalosporin, with either metronidazole or clindamycin. Many of these patients will require emergent surgical drainage. Other medical therapy can include pain control, antipyretics, and steroids to mute the strong inflammatory response, although this remains controversial.60
AIRWAY PLAN OF ATTACK
Protecting the airway is paramount, as mortality from deep space neck infections is overwhelmingly from airway compromise as opposed to systemic sepsis.61 If signs of compromise are present, immediate intubation vs. cricothyrotomy vs. tracheostomy should be performed. It is better to intubate early versus waiting for imminent progression to potentially an airway that will require heroic measures to secure. If the clinical diagnosis is likely and signs/symptoms are present for respiratory compromise, airway management should always occur before imaging studies.
There are no guidelines at this point or pathways for the approach to the airway, nor are there formal recommendations for “watching and waiting versus early intubation”. Intervention is very case-dependent and resource-dependent. If you have ENT or OMFS at your facility, get them involved early.
Because the airway is distorted and manipulation of the airway with direct laryngoscopy can precipitate collapse, you should always be prepared with a surgical airway option at bedside.
In surgical literature, awake surgical airway (tracheostomy) is still designated as the standard of care in deep space infection airway management (SESAP 12, American College of Surgeons, Volume 1, 2004). In a retrospective study of 85 patients seen at Parkland Memorial Hospital in Dallas, Texas, with deep space neck infections, patients with tracheostomy management were compared to those with endotracheal intubation, with findings of shorter overall hospital stays (4.8 vs 5.9 days), shortened ICU stays (1.1 days vs 3.1 days), and lower overall incidence of complications (such as need for repeated surgical drainage, loss of the airway, airway stenosis) in the tracheostomy group (6% vs 10%).62
However, with advancement of airway techniques in the ED, many other strategies have proven successful and efficient, and tracheostomy may not always be necessary in every case. Despite being a small study, a retrospective analysis at UCSF-Fresno of 29 patients identified with true Ludwig’s angina found that only 8 required advanced airway intervention and were managed safely this way, and that no patient required a surgical airway. 63
In the ED, if you have access to Anesthesia for intubation in a more controlled setting, and the patient can be/has time to be/is not in too much extremis to be transferred there, this may be the time to swallow your airway pride, rally the troops, and engage your Anesthesia and Surgical colleagues for an intubation in the OR setting.
If you need to manage the issue in the ED, ideally, if you have capabilities for awake, fiberoptic intubation in a head-up position, this may be the next best option, with surgical rescue option available to you at the bedside.
Make sure to have several “rescues” at the bedside, including video laryngoscopy, bougie, and other supraglottic devices, such as LMA (remembering that, with unpredictable airway distortion, the LMA may not obtain an adequate seal). Try to manipulate the airway as little as possible prior to the intubation attempt.64 Other options include cricothyrotomy under local anesthesia, fiberoptic awake nasotracheal intubation, retrograde intubation (essentially a “needle cric” with a catheter, through which a guidewire is passed in the upward direction, through the cords, grasped, and brought out through the mouth, over which an ETT can be passed), blind nasal intubations, or the conventional intubation with laryngoscopy.65
Blind nasal intubation carries significant inherent risk including rupture of the abscess, disruption of the mucosa, or complete airway obstruction. Awake cricothyrotomy, in a panicked, ill, hypoxic patient can be difficult. As much as possible, try to maintain spontaneous breathing.
Management of the “scary airway” is obviously an art, and these recommendations are open to interpretation. Generally speaking, preparation is key.
- Communicate well with your ED team.
- Always have multiple back-ups that you are comfortable with.
- Review and practice for the potential cricothyrotomy or failed airway scenario.
- Familiarize yourself with awake intubation.
- If you have the opportunity, train with fiberoptics.
- Intubate Early, Apologize Later. Particularly if your sphincter is tight and you think the airway will progress during the patient’s ED stay. You may potentially prevent the need for heroic measures later by securing an airway early.
- Finally, don’t be afraid to involve other subspecialists early in the case, or to elect to have the critical patient intubated in a controlled operating room setting if this is what may be best for the patient.
References / Further Reading
- Mithani S, St.-Hilaire H, Brooke B, Smith I, Bluebond-Langner R, Rodriguez E. Predictable Patterns of Intracranial and Cervical Spine Injury in Craniomaxillofacial Trauma: Analysis of 4786 Patients. Plastic and Reconstructive Surgery. 2009;123(4):1293-1301.
- Curran J. Anaesthesia for facial trauma. Anaesthesia & Intensive Care Medicine. 2014;15(8):373-378.
- Maldonado I, Becker S. Safety of percutaneous tracheostomy in trauma patients. Critical Care. 2010;14(Suppl 1):P225.
- Ben Nun A. Percutaneous tracheostomy in patients with cervical spine fractures – feasible and safe. Interactive CardioVascular and Thoracic Surgery. 2006;5(4):427-429.
- Bagheri S, Holmgren E, Kademani D, Hommer L, Bell R, Potter B et al. Comparison of the Severity of Bilateral Le Fort Injuries in Isolated Midface Trauma. Journal of Oral and Maxillofacial Surgery. 2005;63(8):1123-1129.
- Schaider, J. Bailitz, J. An Evidence Based Approach to Traumatic Emergencies. Neck Trauma: Don’t put your neck on the line. EB Medicine [Internet]. 2003;5(7):5-36. Available from: http://www.ebmedicine.net
- SALETTA J, LOWE R, LIN L, THORNTON J, DELK S, MOSS G. PENETRATING TRAUMA OF THE NECK. The Journal of Trauma: Injury, Infection, and Critical Care. 1976;16(7):579-587.
- Carducci B, Lowe R, Dalsey W. Penetrating neck trauma: Consensus and controversies. Annals of Emergency Medicine. 1986;15(2):208-215.
- Thal E, Meyer D. Penetrating neck trauma. Current Problems in Surgery. 1992;29(1):5-56.
- Todd Eggen J, Jorden R. Airway management, penetrating neck trauma. The Journal of Emergency Medicine. 1993;11(4):381-385.
- Walls R, Wolfe R, Rosen P. Fools rush in? Airway management in penetrating neck trauma. The Journal of Emergency Medicine. 1993;11(4):479-480.
- Desjardins G, Varon A. Airway management for penetrating neck injuries: the Miami experience. Resuscitation. 2001;48(1):71-75.
- Shearer V, Giesecke A. Airway Management for Patients with Penetrating Neck Trauma. Anesthesia & Analgesia. 1993;77(6):1135???1138.
- Mandavia D, Qualls S, Rokos I. Emergency airway management in penetrating neck injury. Annals of Emergency Medicine. 2000;35(3):221-225.
- Weitzel N, Kendall J, Pons P. Blind Nasotracheal Intubation for Patients With Penetrating Neck Trauma. The Journal of Trauma: Injury, Infection, and Critical Care. 2004;56(5):1097-1101.
- Esrailian E, Gralnek I. Nonvariceal Upper Gastrointestinal Bleeding: Epidemiology and Diagnosis. Gastroenterology Clinics of North America. 2005;34(4):589-605.
- Khamaysi I, Gralnek I. Acute upper gastrointestinal bleeding (UGIB) initial evaluation and management. Best Practice & Research Clinical Gastroenterology. 2013;27(5):633-638.
- Palmer K. Acute upper gastrointestinal bleeding. Medicine. 2011;39(2): 94-100.
- Bari K. Treatment of portal hypertension. WJG. 2012;18(11):1166.
- Freeman M. Textbook of Gastroenterology. Philadelphia: Lippincott, Williams, and Wilkins; 2009.
- Mandelstam P, Sugawa C, Silvis S, Nebel O, Rogers G. Complications associated with esophagogastroduodenoscopy and with esophageal dilation. Gastrointestinal Endoscopy. 1976;23(1):16-19.
- Waye J. Intubation and sedation in patients who have emergency upper GI endoscopy for GI bleeding. Gastrointestinal Endoscopy. 2000;51(6): 768-771.
- Rudolph S, Landsverk B, Freeman M. Endotracheal intubation for airway protection during endoscopy for severe upper GI hemorrhage. Gastrointestinal Endoscopy. 2003;57(1):58-61.
- Rehman A, Iscimen R, Yilmaz M, Khan H, Belsher J, Gomez J et al. Prophylactic endotracheal intubation in critically ill patients undergoing endoscopy for upper GI hemorrhage. Gastrointestinal Endoscopy. 2009;69(7):e55-e59.
- Austin K. Harrison’s Principles of Internal Medicine. 9th ed. New York: McGraw Hill Book Co.; 1980.
- Kaplan A. Allergy, Principles and Practice. St Louis, MO: CV Mosby Co; 1978.
- Miller D, Oliveria S, Berlowitz D, Fincke B, Stang P, Lillienfeld D. Angioedema Incidence in US Veterans Initiating Angiotensin-Converting Enzyme Inhibitors. Hypertension. 2008;51(6):1624-1630.
- GRANT N, DEEB Z, CHIA S. Clinical experience with angiotensin-converting enzyme inhibitor induced angioedema. Otolaryngology – Head and Neck Surgery. 2007;137(6):931-935.
- Howes L, Tran D. Can Angiotensin Receptor Antagonists Be Used Safely in Patients with Previous ACE Inhibitor-Induced Angioedema? Drug Safety. 2002;25(2):73-76.
- FRANK M. Hereditary Angioedema: the Clinical Syndrome and Its Management. Annals of Internal Medicine. 1976;84(5):580.
- Frank M. Hereditary Angioedema: The Clinical Syndrome and its Management in the United States. Immunology and Allergy Clinics of North America. 2006;26(4):653-668.
- Bowen T, Cicardi M, Farkas H, Bork K, Longhurst H, Zuraw B et al. 2010 International consensus algorithm for the diagnosis, therapy and Management of hereditary angioedema. Allergy, Asthma & Clinical Immunology. 2010;6(1):24.
- Pruet C, Kornblut A, Brickman C, Kaliner M. MANAGEMENT OF THE AIRWAY IN PATIENTS WITH ANGIOEDEMA. The Laryngoscope. 1983;93(6):749???755.
- Elliott W. Incidence and Characteristics of Angioedema Associated With Enalapril. Yearbook of Cardiology. 2006;2006:80-81.
- CHAMPION R, ROBERTS S, CARPENTER R, ROGER J. URTICARIA AND ANGIO-OEDEMA. Br J Dermatol. 1969;81(8):588-597.
- Chiu A, Burningham A, Newkirk K, Krowiak E, Davidson B, Deeb Z. Angiotensin-Converting Enzyme Inhibitor-Induced Angioedema: A Multicenter Review and an Algorithm for Airway Management. Annals of Otology, Rhinology & Laryngology. 2001;110(9):834-840.
- Banerji A, Clark S, Blanda M, LoVecchio F, Snyder B, Camargo C. Multicenter study of patients with angiotensin-converting enzyme inhibitor- induced angioedema who present to the emergency department. Annals of Allergy, Asthma & Immunology. 2008;100(4):327-332.
- Lewis L. Angioedema: Etiology, Pathophysiology, Current and Emerging Therapies. The Journal of Emergency Medicine. 2013;45(5):789-796.
- Pekdemir M, Ersel M, Aksay E, Yanturali S, Akturk A, Kiyan S. Effective Treatment of Hereditary Angioedema with Fresh Frozen Plasma in an Emergency Department. The Journal of Emergency Medicine. 2007;33(2): 137-139.
- Prematta M, Gibbs J, Pratt E, Stoughton T, Craig T. Fresh frozen plasma for the treatment of hereditary angioedema. Annals of Allergy, Asthma & Immunology. 2007;98(4):383-388.
- Karim M, Masood A. Fresh-frozen plasma as a treatment for life-threatening ACE-inhibitor angioedema. Journal of Allergy and Clinical Immunology. 2002;109(2):370-371.
- Warrier M, Copilevitz C, Dykewicz M, Slavin R. Fresh frozen plasma in the treatment of resistant angiotensin-converting enzyme inhibitor angioedema. Annals of Allergy, Asthma & Immunology. 2004;92(5):573-575.
- McCormick M, Folbe A, Lin H, Hooten J, Yoo G, Krouse J. Site involvement as a predictor of airway intervention in angioedema. The Laryngoscope. 2011;121(2):262-266.
- GRANT N, DEEB Z, CHIA S. Clinical experience with angiotensin-converting enzyme inhibitor induced angioedema. Otolaryngology – Head and Neck Surgery. 2007;137(6):931-935.
- Al-Khudari S, Loochtan M, Peterson E, Yaremchuk K. Management of angiotensin-converting enzyme inhibitor-induced angioedema. The Laryngoscope. 2011;121(11):2327-2334.
- Brook C, Devaiah A, Davis E. Angioedema of the upper aerodigestive tract: risk factors associated with airway intervention and management algorithm. International Forum of Allergy & Rhinology. 2014;4(3):239-245.
- Nasir M, Sharma G. Angiotensin-converting Enzyme Inhibitor And Angiotensin II Receptor Blocker-Induced Angioedema: Overuse of Ineffective Treatment. Journal of Allergy and Clinical Immunology. 2011;127(2):AB105-AB105.
- Sondhi D. Airway Compromise Due to Angiotensin-Converting Enzyme Inhibitor-Induced Angioedema. Chest. 2004;126(2):400.
- Banerji A, Clark S, Blanda M, LoVecchio F, Snyder B, Camargo C. Multicenter study of patients with angiotensin-converting enzyme inhibitor- induced angioedema who present to the emergency department. Annals of Allergy, Asthma & Immunology. 2008;100(4):327-332.
- Bentsianov B, Parhiscar A, Azer M, Har-El G. The Role of Fiberoptic Nasopharyngoscopy in the Management of the Acute Airway in Angioneurotic Edema. The Laryngoscope. 2000;110(12):2016-2019.
- ISHOO E, SHAH U, GRILLONE G, STRAM J, FULEIHAN N. Predicting airway risk in angioedema: Staging system based on presentation Otolaryngology – Head and Neck Surgery. 1999;121(3):263-268.
- Walls R, Murphy M. Manual of emergency airway management. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
- Chiu A, Burningham A, Newkirk K, Krowiak E, Davidson B, Deeb Z. Angiotensin-Converting Enzyme Inhibitor-Induced Angioedema: A Multicenter Review and an Algorithm for Airway Management. Annals of Otology, Rhinology & Laryngology. 2001;110(9):834-840.
- Palmer M, Rosenbaum S. Clinical practice guideline: initial evaluation and management of patients presenting with acute urticaria or angioedema. [Internet]. 2015 [cited 1 August 2011];. Available from: http://www.aaem.org/ education/urticaria_angioedema
- UNGKANONT K, YELLON R, WEISSMAN J, CASSELBRANT M, GONZALEZVALDEPENA H, BLUESTONE C. Head and neck space infections in infants and children. Otolaryngology – Head and Neck Surgery. 1995;112(3):375-382.
- Huang T, Liu T, Chen P, Tseng F, Yeh T, Chen Y. Deep neck infection: Analysis of 185 cases. Head & Neck. 2004;26(10):854-860.
- Bakir S, Tanriverdi M, Yorgancilar A, Yildirim M, Tekbas G et al. Deep neck space infections: a retrospective review of 173 cases. American Journal of Otolaryngology. 2012;33(1):56-63.
- Kremer M, Blair T. Ludwig angina: forewarned is forearmed. Journal of the American Association of Nurse Anesthesia. 2006;74:445-451.
- Bottin R, Marioni G, Rinaldi R, Boninsegna M, Salvadori L, Staffieri A. Deep neck infection: a present-day complication. A retrospective review of 83 cases (1998?2001). European Archives of Oto-Rhino-Laryngology. 2003;260(10):576-579.
- Saifeldeen K. Ludwig’s angina. Emergency Medicine Journal. 2004;21(2): 242-243.
- Jenkins K, Wong D, Correa R. Management choices for the difficult airway by anesthesiologists in Canada. Can J Anesth/J Can Anesth. 2002;49(8): 850-856.
- Potter J, Herford A, Ellis E. Tracheotomy versus endotracheal intubation for airway management in deep neck space infections. Journal of Oral and Maxillofacial Surgery. 2002;60(4):349-354.
- Wolfe M, Davis J, Parks S. Is surgical airway necessary for airway management in deep neck infections and Ludwig angina? Journal of Critical Care. 2011;26(1):11-14.
- Karkos P, Leong S, Beer H, Apostolidou M, Panarese A. Challenging airways in deep neck space infections. American Journal of Otolaryngology. 2007;28(6):415-418.
- Hagberg C. Special devices and techniques. Anesthesiology Clinics of North America. 2002;20(4):907-932.
- http://www.ncbi.nlm.nih.gov/pubmed/23200327
- http://www.ncbi.nlm.nih.gov/pubmed/19945607
- http://www.ncbi.nlm.nih.gov/pubmed/24582643






3 thoughts on “The Sphincter Series: A Scary Airway Review”
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Airway Obstruction - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationThe EM Educator Series: Trauma to the Face, Challenging Airway, and Other Considerations - emDOCs.net - Emergency Medicine Education
Thank you! I am really impressed. It is a fantastic, deeply ( and scary) pragmatic glance to a wide range of difficult airway cases. Some of the principles and advises found here should be carved into our brains.