Authors: Mark Kastner, MD and Kathryn T. Kopec, DO (Department of Emergency Medicine, Carolinas Medical Center, Charlotte, NC) // Reviewed by: Cynthia Santos, MD (@CynthiaSantosMD); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)

Overview
Methotrexate toxicity is a rare emergency department presentation; however, its toxicity has a high potential for morbidity and mortality. Methotrexate is used in a variety of medical conditions including rheumatoid arthritis (RA), psoriasis, organ transplants, malignancy, and termination of pregnancy. (1) It is used in these conditions to assist with lowering the immune systems’ response to reduce rheumatological flare ups and slow down or halt cellular metabolism in an effort to fight malignancy. (2) Methotrexate is generally well tolerated by patients and affordable when compared to other treatments for these pathologies. Unfortunately, the mortality of toxicity is as high as 6% in high dose therapy (= or > 1000mg/m2) and most commonly seen when levels are not being routinely monitored. (2)
Pathophysiology
Methotrexate inhibits dihydrofolate reductase (DHFR) with 1000 times more affinity than folate. (3) It competitively inhibits the conversion of folate to tetrahydrofolate (THF). (Image 1)
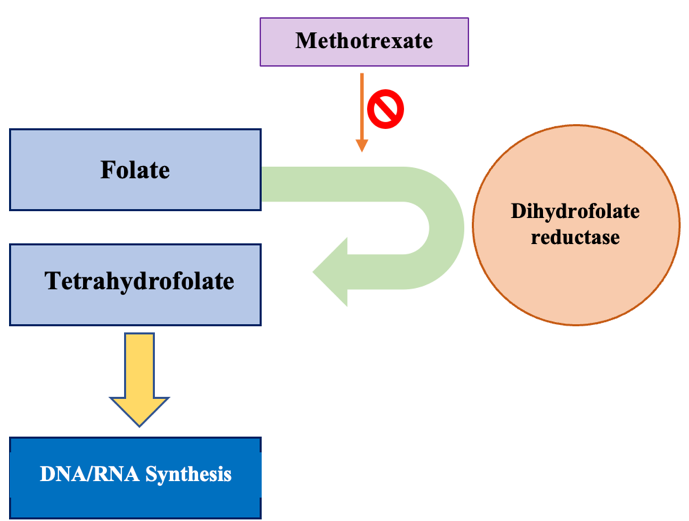
Image 1: Mechanism of Action of Methotrexate
THF is an essential compound in the synthesis of purines which are needed to make DNA. (3)
Therefore, methotrexate leads to the inability of cellular division.
Methotrexate has multiple possible routes of administration including oral, intravenous, intramuscular, and intrathecal. (4) It also has a wide range of dosing variability. When taken orally, peak plasma concentrations of the drug occur in about 2 hours and it has a bioavailability of about 64-90%. (1,5) Peak serum concentration after an IM injection occurs in 30-60 minutes.
Methotrexate’s half-life is 3-10 hours with doses less than 30mg/m2 and 8-15 hours at doses higher than that in IV, IM, and oral forms. (4) Methotrexate is excreted renally putting patients with chronic kidney disease or acute kidney injury at higher risk for toxicity secondary to reduced clearance. (6) Interestingly, studies have shown that low dose folate supplementation will not decrease efficacy of methotrexate therapy and is actually recommended in patients taking it for RA. (7)
Clinical Presentation
Patients usually present with nonspecific symptoms, so a detailed history is crucial to making the diagnosis. Common symptoms of toxicity include: (1)
- Oral mucositis
- Nausea, vomiting, & diarrhea
- GI hemorrhage
- Hepatitis
- Acute kidney injury
- Myelosuppression – leukopenia
- Encephalopathy
Nephrotoxicity is common as methotrexate and its metabolites can precipitate and cause direct damage to the renal tubules and hypoperfusion from arteriolar vasoconstriction. (3)
Intrathecal toxicity presents with more neurological symptoms such as altered mental status, back pain, seizures, irritability, ataxia, and hemiparesis. (4) Transaminitis and myelosuppression are more common in patients with chronic methotrexate exposure but can also be seen in acute poisonings. (2)
Diagnostic Testing
Secondary to an often non-specific clinical presentation, patients will need a laboratory workup to assess for other etiologies, while keeping a high suspicion of methotrexate toxicity. Recommended laboratory testing includes:
- CBC with differential – to assess bone marrow suppression
- LFTs – to assess for transaminitis
- BMP – to assess kidney function and electrolytes
- Urine pH can be helpful in case therapeutic interventions are needed
Methotrexate serum concentration levels can vary in their laboratory turnaround time. Typically, a level will come back in about 1-3 hours for in-house laboratories, so it can be useful in the emergency department. CSF methotrexate levels can also be measured by fluid obtained from a lumbar puncture. (8) Toxicity is based on the level and when the last dose was taken. (9) Levels should be monitored every 24 hours in the setting of toxicity. (6)
MTX levels considered toxic: (10)
24 hours after last dose: > 10 micromol/L
48 hours after last dose: > 1 micromol/L
72 hours after last dose: > 0.1 micromol/L
Management
Management is targeted based on the route, dosing, and clinical symptoms.
Most commonly, patients will present to the ED after an oral overdose. Activated charcoal therapy should be considered if the ingestion was within 1-2 hours of arrival and the patient has a normal mental status. GI symptoms should be treated with supportive and symptomatic care such as antiemetics and analgesia.
Oral mucositis is a dose related adverse effect that is caused by both normal and toxic concentrations of the drug. (3) In severe cases, this is considered an oncologic emergency because it can lead to infections. Folic acid supplementation should be started or increased as this will help with the ulcerations. (11) Analgesia with the swish and spit method can be used with the following solutions:
– Viscous lidocaine
– Liquid diphenhydramine
– Magic Mouthwash
Dexamethasone or other oral steroid preparations can also be applied or swished and spit out. (11) If the pain is so severe that the patient cannot tolerate PO, then IV pain medications can be used. Ultimately, some patients may require IV maintenance fluids or nutritional supplementation with TPN.
Nephrotoxicity can occur and should be treated with aggressive IVF hydration to maintain kidney perfusion and prevent further renal injury. (3) Greater then 2-2.5L/day of urine output is recommended. (9)
Alkalinization of the urine with IV sodium bicarbonate can help prevent precipitation of the methotrexate. This is done by giving a bolus of 1-2 mEq /kg of sodium bicarbonate until urine pH is > 7. (3) Once goal urine pH is met, maintenance fluids containing sodium bicarbonate to maintain the urine pH is suggested.
There are no specific indications for hemodialysis, although it may be of some benefit in patients with a pre-existing AKI. Get nephrology on board early in these patients to determine its value.
Methotrexate still present in the serum can be dialyzed off, but HD will not reverse effects from intracellular toxicity that has already occurred. (12)
Intrathecal overdose is life threatening. If identified early the methotrexate-CSF mixture can be drained back out. An equal amount of normal saline must then be infused. This process, referred to as ventriculolumbar perfusion, must be done over a couple hours and the CSF pressure needs to be closely monitored. (8)
Bone marrow suppression should be treated in conjunction with a hematologist. Granulocyte colony-stimulating factor (GCSF) can be used to help produce additional cell lines. Platelet and RBC transfusions may also be necessary. (6)
Antidotes:
Leucovorin (folinic acid):
- Folinic acid is the active form of folate and it does not require DHFR (which is inhibited by methotrexate) (13)
- Allows cells to overcome the inhibition by MTX and make DNA.
- Should be given as soon as possible after an overdose, do not wait for methotrexate levels to return
- Aim to administer leucovorin at the same dose or greater than that of the methotrexate dose that was taken by the patient. (14)
- Dose range is 10 to 25 mg/m2 IV or IM every 6 hours for at least 72 hours
- Some toxicologists will also use a starting dose of 100 mg/m2 over 15-20 minutes
- Often given until methotrexate concentrations are undetectable
- Can also be given even with negative MTX levels if leukopenia is still present (2)
- Dosing for patients with renal compromise is 150 mg/m2 q3 hours initially
Glucarpidase:
- Reserved for use in patients with delayed renal clearance (15)
- Hydrolyzes methotrexate into inactive compounds
- Can be given both IV and intrathecally
- Dose is 50 units/kg IV bolus over 5 minutes (13)
- Adverse effects include nausea, vomiting, headache, hypotension, and flushing. (16)
Take Home Points:
- Methotrexate is used in multiple medical conditions and toxicity will likely only become more common as its’ therapeutic indications continue to expand.
- Clinical presentation can be non-specific, so history and a high level of suspicion are key in the diagnosis of methotrexate toxicity.
- CBC, BMP, LFTs, urinalysis, and methotrexate levels are recommended if there is concern for toxicity.
- Once the diagnosis is made, aggressive IVF hydration and urine alkalization are the mainstays of treatment to protect the kidneys. Dialysis can be considered.
- Folinic acid (leucovorin) should be used as early as possible and is the mainstay of treatment.
- Glucarpidase is used in patients with delayed renal clearance and is one of the only treatments that can be administered intrathecally.
References:
- Bertino, Joseph R. “Methotrexate: historical aspects.” Methotrexate. Birkhäuser, Basel, 2000. 1-7.
- Wang, Richard Y.”Methotrexate, 5-Fluorouracil, and Capecitabine.” Goldfrank’s Toxicologic Emergencies, 11e Lewis S. Nelson, et al. McGraw-Hill, 2019, https://accessemergencymedicine-mhmedical-com.libproxy.lib.unc.edu/content.aspx?bookid=2569§ionid=210272684.
- Howard, Scott C., et al. “Preventing and managing toxicities of high-dose methotrexate.” The oncologist12 (2016): 1471.
- In: In Depth Answers [database on the Internet]. Greenwood Village (CO): IBM Corporation; 2021 [cited March 10, 2021]. Available from: www.micromedexsolutions.com. Subscription required to view.
- National Center for Biotechnology Information. “PubChem Compound Summary for CID 126941, Methotrexate” PubChem, https://pubchem.ncbi.nlm.nih.gov/compound/Methotrexate. Accessed 16 March, 2021.
- Widemann, Brigitte C., and Peter C. Adamson. “Understanding and managing methotrexate nephrotoxicity.” The oncologist6 (2006): 694-703.
- Morgan, Sarah L., et al. “Supplementation with folic acid during methotrexate therapy for rheumatoid arthritis: a double-blind, placebo-controlled trial.” Annals of internal medicine11 (1994): 833-841.
- O’Marcaigh, Aengus S., et al. “Successful treatment of intrathecal methotrexate overdose by using ventriculolumbar perfusion and intrathecal instillation of carboxypeptidase G2.” Mayo Clinic Proceedings. Vol. 71. No. 2. Elsevier, 1996.
- “Test ID: MTHX Methotrexate, Serum.” MTHX – Clinical: Methotrexate, Serum, www.mayocliniclabs.com/test-catalog/Clinical+and+Interpretive/37047.
- “Test ID: MTHX Methotrexate, Serum.” MTHX – Clinical: Methotrexate, Serum, www.mayocliniclabs.com/test-catalog/Clinical+and+Interpretive/37047.
- Scully, Crispian, Meir Gorsky, and Francina Lozada-Nur. “The diagnosis and management of recurrent aphthous stomatitis: a consensus approach.” The Journal of the American Dental Association2 (2003): 200-207.
- Wall, Susan M., et al. “Effective clearance of methotrexate using high-flux hemodialysis membranes.” American journal of kidney diseases6 (1996): 846-854.
- LaSala, Gregory S, et al. “Leucovorin to the Rescue.” Emergency Medicine News, 21 Aug. 2016, journals.lww.com/emnews/blog/thetoxcave/pages/post.aspx?PostID=28#:~:text=Leucovorin%20(folinic%20acid)%20should%20be,counteract%20the%20effects%20of%20methotrexate.
- Olson, Kent R., et al., eds. Poisoning & drug overdose. Vol. 13. Lange Medical Books/McGraw-Hill, 2007.
- Ramsey, Laura B., et al. “Consensus guideline for use of glucarpidase in patients with high‐dose methotrexate induced acute kidney injury and delayed methotrexate clearance.” The oncologist1 (2018): 52.
- Kitchlu, Abhijat, and Anushree C. Shirali. “High-flux hemodialysis versus glucarpidase for methotrexate-associated acute kidney injury: What’s best?.” Journal of Onco-Nephrology1 (2019): 11-18.





1 thought on “ToxCard: Methotrexate ”
good! learning a little more thanks to your work!