Originally published on Ultrasound G.E.L. on 11/11/19 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!

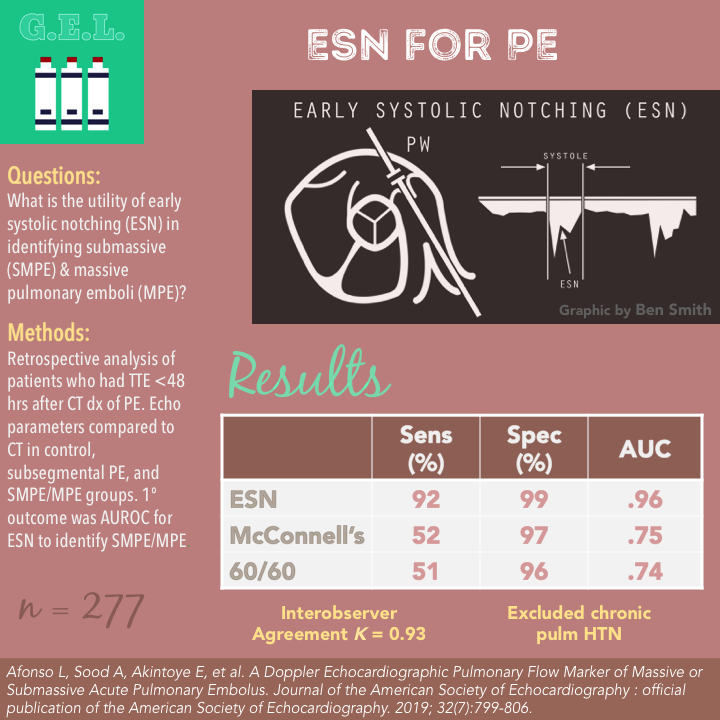
A Doppler Echocardiographic Pulmonary Flow Marker of Massive or Submassive Acute Pulmonary Embolus
J Am Soc Echocardiogr July 2019 – Pubmed Link
Take Home Points
1. In patients with suspected PE, the ESN pattern is highly sensitive and specific for a submassive or massive PE.
2. More research needs to be done to examine the feasibility of this test in a broader population of patients and operators, as well as to evaluate patient centered outcomes.
Background
Pulmonary embolism is common and represents a wide spectrum of illness severity. Point of care echocardiography has been used in the past to find evidence of right heart strain. This, in combination with their hemodynamic status, can help with stratification of these patients into a submassive or massive category which has diagnostic and prognostic value. However – none of the traditionally assessed signs are perfect. Not all PE patients with have classic findings such as an enlarged right ventricle, septal bowing, McConnell’s sign, etc. We’ve looked at other signs such as TAPSE before – and found that this is not sensitive enough to diagnose PE. These authors take a look at a new echocardiographic parameter that might be even more accurate in diagnosing the subset of massive and submassive PE: the right ventricular outflow tract early systolic notch (ESN).
Check out The Evidence Atlas – Echo for a review of prior evidence on point of care ultrasound in pulmonary embolism.
Questions
Which echocardiographic markers are most accurate in the diagnosis of massive and submassive pulmonary embolism?
(It seems that they were mostly looking at ESN based on their preliminary research.)
Population
Single academic center, between 2015-2017
Inclusion:
- Transthoracic echocardiography (TTE) within 48 hours of CT diagnosis of pulmonary embolism
Exclusions:
- Did not have complete exams with right ventricular outflow tract (RVOT) pulsed-wave doppler, tricuspid regurgitation, discernable RV endocardial border
- Suboptimal PW doppler studies
- Greater than moderate valvular heart disease
- History of PE
- Chronic pulmonary hypertension
Design
Retrospective cohort
RV dysfunction on CT defined as RV/LV diameter >0.9
Only counted segmental PEs or bigger (smaller PE’s would have been considered the same as having no PE)
Massive PE (MPE) defined by AHA definition: hypotension <90 mm Hg ≥ 15 min or requiring inotropic support (and hypotension not due to other cause) or pulselessness, or bradycardia + shock
Submassive PE (SMPE) defined as RV dilation on CT but no hypotension
Subsegmental PE (SSPE) defined as acute PE but none of those other things
This definition of “subsegmental” combined with excluding anything less than a truly segmental PE on CT is a bit unconventional
- CT is not a traditional or guideline based standard for defining submassive PE
- This is not a traditional subsegmental PE definition
- This could result in a large PE (without acute RV dilation or hypotension) being categorized as “subsegmental” in this study
The TTE measured:
- Early systolic notching from RVOT (also referred to as the “Spike and Dome pattern”
- Ejection time from RVOT
- Acceleration time from RVOT
- Deceleration time
- Spike and Dome velocities
- AT/ejection time ratio
- Notch time
- RVOT VTI
- RV diameter
- 60/60 Sign (link to 5 min sono)
- McConnell’s sign
Interobserverer variability assessed for ESN
Using CTA-confirmed diagnosis of Massive PE or Submassive PE, they calculated test characteristics and ROC. Then determined optimal cut offs for other echocardiographic parameters. Then looked for parameters with benefit if added to the ESN.
Secondary analysis looked at predictive utility for patients with subsegmental PE.
Who did the ultrasounds?
Presumably echocardiographers – not specifically mentioned but since this was retrospective it was whoever had already done the echo.
The Scan
Phased array transducer

Special thank you to Ben Smith @UltrasoundJelly for crafting this lovely graphic. Find more great stuff from Ben at his website ultrasoundoftheweek.com.

Here’s how the paper described it:
Pulsed Wave Doppler of RVOT was performed with parasternal short axis view at level of aortic valve or from the subcostal short axis
Sample 0.5 cm proximal to pulmonic valve
Looked for early systolic notching (ESN), aka the spike and dome morphology. Binary present or not. The “spike” is a narrow peaked initial wave with early deceleration and had to occur within first half of systole, followed by a second doppler wave that was more curvilinear (dome).
Notches later in systole were called midsystolic notching.
Sweep speed should be 50-100 mm/sec
Learn how to do Echo for Right Heart Strain from 5 Minute Sono!
Learn how to do the 60/60 Sign from 5 Minute Sono!

Check out Right Ventricle Pathology on the POCUS Atlas!

Results
Patients
- Started with 5122 patients who had CT for suspected PE
- 526 (10.2%) had a PE of any type
- After initial screening they were down to 260
- After cutting the scans with inadequate RVOT imaging, down to 187
- Then they added in 90 patients WITHOUT PE for control group.
N = 277
- Mean age 56 years
- 48% men
- 44% MPE or SMPE
- 38% with SSPE
- 39% no PE
- Demographic table: less males in SSPE group, more smokers in MPE/SMPE group, more hypertension in no PE group, lower SBP in
- MPE/SMPE, higher HR in groups with more PE
Primary Outcome
Test Characteristics for ESN to Identify MPE or SMPE
Sensitivity 92% (CI 84-97%)
Specificity 99% (CI 96-100)
AUROC 0.96 (CI .92-.98)
ESN was observed in 92% of patients with MPE or SMPE, 2% of SSPE and no patients without PE
Secondary Findings
ESN was more accurate than the other echo findings
McConnell’s Sign
Sensitivity 52% (CI 40-63%)
Specificity 97% (CI 94-99%)
AUROC 0.75 (CI .68-0.80)
60/60 Sign
Sensitivity 51% (CI 40-62%)
Specificity 96% (CI 91-99%)
AUROC 0.74 (CI .68-.79)
Having a low Acceleration time (≤ 87 msec) or low AT/ejection time were about 90% sensitive but still not as good as ESN, which was most sensitive.
ESN was also most specific, and McConnell’s and 60/60 sign were the only other ones that came close.
None of the signs were remotely sensitive for a SSPE (single digits) but they were still fairly specific (92-95%).
Adding any of these other parameters to the ESN did not improve its accuracy.
Additional Findings
SSPE 19% had midsystolic notching but only 2% with early systolic (so the fact that it is early is an important distinction)
In MPE or SMPE – systolic notching was early in 92% and mid in 1%
100% of control subjects had no systolic notching
Of the patients with either MPE or SMPE without ESN (n = 7), 5 had poorly discernible or intermittent ESN or midsystolic notching. 2 had the triphasic doppler pattern which apparently also counts as ESN.
Interobserver agreement on ESN K = 0.93
Limitations
Not quite POCUS – but honestly it is probably better to have this established by more comprehensive imaging before testing with an additional variable of experience level.
Highly selected population. This was patients with suspected PE. There was an overall incidence of 10.2% incidence of PE, but we don’t know the specific overall risk of the population since they randomly added 90 patients without PE.
Definitions. As mentioned above, the definitions for submassive and subsegmental PE are not typical. Is CT the best way to identify submassive PE? This study showed that echo picks up a lot more RV strain than CT. Most people will take into account positive biomarkers such as troponin or BNP and echocardiographic findings in determining a submassive PE. Furthermore, it is confusing to call the smaller PEs in this study “subsegmental”, when they were at least segmental (they excluded PEs that were smaller). These PEs could actually be any size at all as long as there was no hypotension or right heart strain on CT. Therefore, this population is likely skewed towards larger PEs. This is important to understand if you are applying this test to a population of all PEs, where the accuracy might not be the same. It would be great to have this data reanalyzed using more conventional definitions.
This is probably hard to get, especially if not used to complex PW doppler measurements. This is evidenced by the fact that they excluded 28% (73/260) of their patients because the RVOT doppler was not satisfactory. The authors mention that this can be influenced by sweep speed, distance to valve, angle. Even the representative pictures of ESN in the article are hard to discern the finding. One has triphasic notching which is apparently also diagnostics!
Excluded preexisting pulmonary arterial hypertension. So it might not be able to determine how acute the process is- this is where the 60/60 rule might be more useful. The authors suggest that in people with PAH, the notching might be later (not early). It is important to remember that ESN does not necessary PE, but that there is some fairly proximal obstruction in the pulmonary vasculature (so theoretically a compressive tumor could cause it as well).
Discussion
Why does the ESN happen? Authors propose that the systolic flow deceleration is from the blood flow being reflected back due to the increase in the pressure in the pulmonary arteries. The blood then continues forward due to the patency of the remainder of the pulmonary bed. How high and early this first “spike” wave comes is dependent on the degree of pulmonary vascular resistance and the distance to that area. Therefore, the PASP is inversely related to notching timing. That is why it is more mid systolic in less severe (usually smaller) PEs.
What do we do with this information? This study does not tell us when to suspect a PE – because all of the patients included were already suspected of the etiology. What it tells us is that in patients with a possible PE, the RVOT ESN predicts which are submassive or massive. You would think that for massive PE, you would be able to figure that out based on their hypotension. So perhaps this comes down to more accurately identifying submassive PE, compared to traditional echo parameters. If this is the case, there are two questions remaining. The first is – does it outperform the use of CT findings or serum markers to diagnose? The second is – does this change patient centered outcomes? It is at least conceivable that it might. Submassive PEs have higher mortality, so prognostication could be valuable. More importantly, some submassive PEs are candidates for catheter directed thrombolytics, so perhaps by identifying this group earlier, a more targeted therapy can be applied. Obviously, more data is needed because currently there are a lot of assumptions you have to make to obtain this proposed benefit.
Take Home Points
1. In patients with suspected PE, the ESN pattern is highly sensitive and specific for a submassive or massive PE.
2. More research needs to be done to examine the feasibility of this test in a broader population of patients and operators, as well as to evaluate patient centered outcomes.
Our score
Expert Reviewer for this Post

Nik Theyyunni, MD @Heydrnik
Nik Theyyunni is the ultrasound director at the University of Michigan, Department of Emergency Medicine.
Reviewer’s Comments
The criterion standard issue is a huge limitation in our ability to use this in practice. I’d like to see this study reanalyzed as discussed above – then we could use this data to discuss if we should be using this with PERT teams or other stake holders rather than this just being a cool ultrasound thing.
Cite this post as
Michael Prats. Early Systolic Notching for Pulmonary Embolism. Ultrasound G.E.L. Podcast Blog. Published on November 11, 2019. Accessed on June 25, 2021. Available at https://www.ultrasoundgel.org/80.




