Originally published on Ultrasound G.E.L. on 11/06/17 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM), Dr. Creagh Bougler, MD (@CreaghB), and Dr. Jacob Avila, MD (@UltrasoundMD) from Ultrasound G.E.L. team!
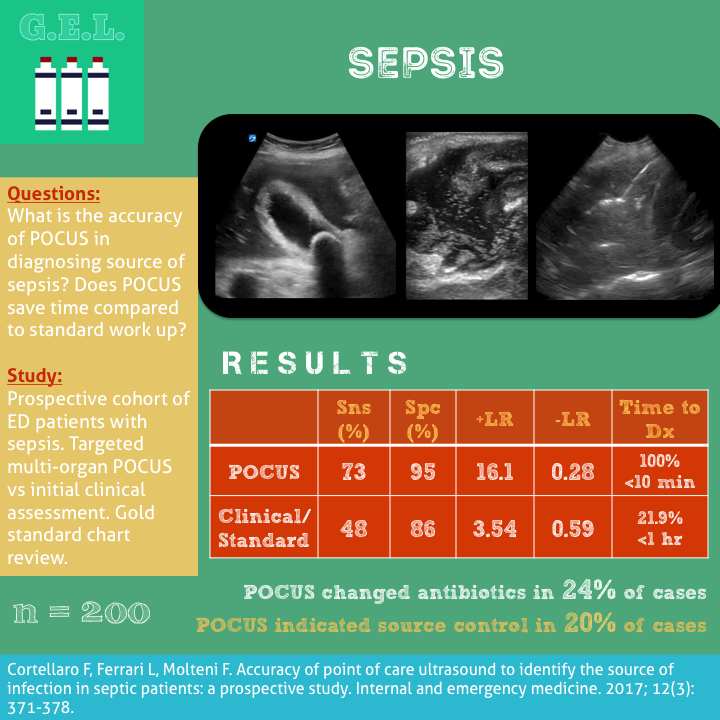
Accuracy of point of care ultrasound to identify the source of infection in septic patients: a prospective study
Intern Emerg Med April 2017 – Pubmed Link
Take Home Points
1. Using POCUS in evaluation of sepsis is more accurate than physical exam and history alone.
2. POCUS is specific for sepsis source diagnoses with +LR 16.06.
3. Using POCUS can potentially save time to diagnosis and appropriately alter management.
Background
Sepsis is a disease that is prevalent and has a high mortality. We now have a lot of emphasis being placed on early diagnosis of sepsis, early antibiotics, and early source control. We know that ultrasound can find a lot of potential causes for sepsis, and it can potentially saves some time in doing so. This article takes a look to see how the diagnosis made with ultrasound compares to a traditional work up – both in time and accuracy.
Questions
What is the accuracy of using point-of-care ultrasound (POCUS) in diagnosing the source of sepsis?
What is the time to source identification with POCUS compared to standard work up?
Population
Single center, tertiary care hospital in Italy
Emergency department patients
Inclusion:
- The presence of infection (probable or documented) + 2 or more systemic manifestations of infection (Surviving Sepsis Campaign definition)
Exclusion:
- Refusal to consent
- Unable to obtain consent
Design
Prospective cohort
Intervention
Step 1. All patients received “initial clinical assessment” which included:
- history and physical exam
- Arterial blood gas
- lactate
Step 2. Then, based on Step 1
- diagnostic work up determined
- interventions determined
- provisional source of sepsis identified
Step 3. Within 10 minutes – the same physician would perform POCUS
- Could choose lung, abdominal, cardiac, soft tissue, or joint based on preliminary diagnosis and H&P
- If no clear source, did all of the scans!
- If scan was indeterminant, it was called non-diagnostic
- Recorded change in therapeutic interventions
- Recording new diagnosis based on POCUS
- Patients were allowed to have treatment plan changed based on POCUS
Step 4. After hospital discharge, two emergency physicians determined the source of the patients’ sepsis (with a third to help if disagreement).
Who did the ultrasounds?
Emergency physicians trained according to the Italian Society of Emergency Medicine (SIMEU) guidelines with SIMEU and WINFOCUS certification in emergency ultrasound;
The Scan
There were a lot of scans using a variety of probes. If you don’t know how to do any of these, check out the videos below!
Lung – 10 lung fields
Abdominal – including looking for hepatic abscess and diverticula and appendix
Cardiac – including assessment for vegetation
Soft tissue – abdominal muscle abscess, not otherwise described
Joints – intraarticular fluid
Results
Patients
n=200
- Mean age was 64.2 years old
- 71/200 patients (35 %) met diagnostic criteria for severe sepsis or septic shock
- 89% had source identified after chart review
Most common Infections:
- Respiratory (pneumonia) (39.5 %)
- Urinary (23%)
- Abdominal infections (19.5 %). Cholecystitis most common.
Primary Outcome
Accuracy for Diagnosis
POCUS:
Sensitivity 73% (66-79%)
Specificity 95% (77-99)
+LR 16.06
-LR 0.28
Accuracy 75%
Clinical Assessment:
Sensitivity 48% (41-55%)
Specificity 86% (66-95%)
+LR 3.54
-LR 0.59
Accuracy 52.5%
Secondary Outcomes
Time to Diagnosis:
POCUS:
73% had source identified
100% diagnoses <10 minutes
Standard work-up:
89% had source identified
<1 hr in 21.9%
<2 hr in 52.8%
<6 hr in 71.3%
24 hr in 15.7%
Other Findings
POCUS diagnosis changed antibiotics given in 24% of cases – and it was in an appropriate change in accordance with final diagnosis as determined by chart review (except in one case of malaria).
POCUS helped indicate source control strategy in 20%.
- examples were surgery, interventional radiology for hydronephrosis with ureterolithiasis, or endoscopic procedures in cholangitis with biliary obstruction.
Among the 48 sources not immediately identified by POCUS, 30 (62.5%) were urinary tract infections.
POCUS had only one false positive in a patient in whom a soft tissue abscess was considered the septic source but the final diagnosis was malaria.
POCUS is 97% sensitive for respiratory infection, 79% for abdominal infection, then sensitivity drops off for other causes of sepsis.
Limitations
May be an unfair comparison. Compared POCUS to having barely any diagnostic information (only history, physical, blood gas and lactate?). May have been more fair to compare a full work up without POCUS to a full work up with POCUS.
The authors make the claim that POCUS could help decrease time to antibiotics. This makes the assumption that antibiotics are being delayed for finding a source. If this is not true (as many patients are given early broad spectrum antibiotics), there may not be as big a benefit to POCUS. However, it is still good to know source for more targeted antibiotics, earlier deescalation, and source control.
Same physician treating patient and performing ultrasound. On the one hand, this could bias someone to see something that they already suspect; HOWEVER, this is actually how POCUS is supposed to be used – by the provider, for the provider. Therefore, this is actually a good thing about this study, it reflects what should be happening in clinical practice. They also did not allow the initial diagnostics ordered to be changed.
Not enough cases to know how good it is for finding endocarditis (traditionally TTE is not sensitive), soft tissue abscess, and joint infection.
How did they determine the timing for the POCUS diagnosis? Is it a fair comparison? Whereas the clock stops for POCUS right after the exam is complete, it is not clear what determined the end-point of the time to diagnosis for the standard work up.
Fairly advanced ultrasound skills – diverticulitis, appendicitis, endocarditis? These guys are pros. This may not be externally valid if you are not an Italian POCUS all-star.
Not quite patient oriented outcomes. It did change the management of the physician a good amount. We might be tempted to extrapolate that earlier diagnosis means earlier antibiotics and better outcomes but we clearly need more research.
Take Home Points
1. Using POCUS in evaluation of sepsis is more accurate than physical exam and history alone.
2. POCUS is specific for sepsis source diagnoses with +LR 16.06.
3. Using POCUS can potentially save time to diagnosis and appropriately alter management.
Our score





2 thoughts on “Ultrasound G.E.L. – POCUS in Sepsis”
Pingback: Ultraljud vid sepsis – Mind palace of an ER doc
Pingback: LITFL Review 350 • LITFL Medical Blog • FOAMed Review