Originally published on Ultrasound G.E.L. on 1/30/17 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM), Dr. Creagh Bougler, MD (@CreaghB), and Dr. Jacob Avila, MD (@UltrasoundMD) from Ultrasound G.E.L. team!
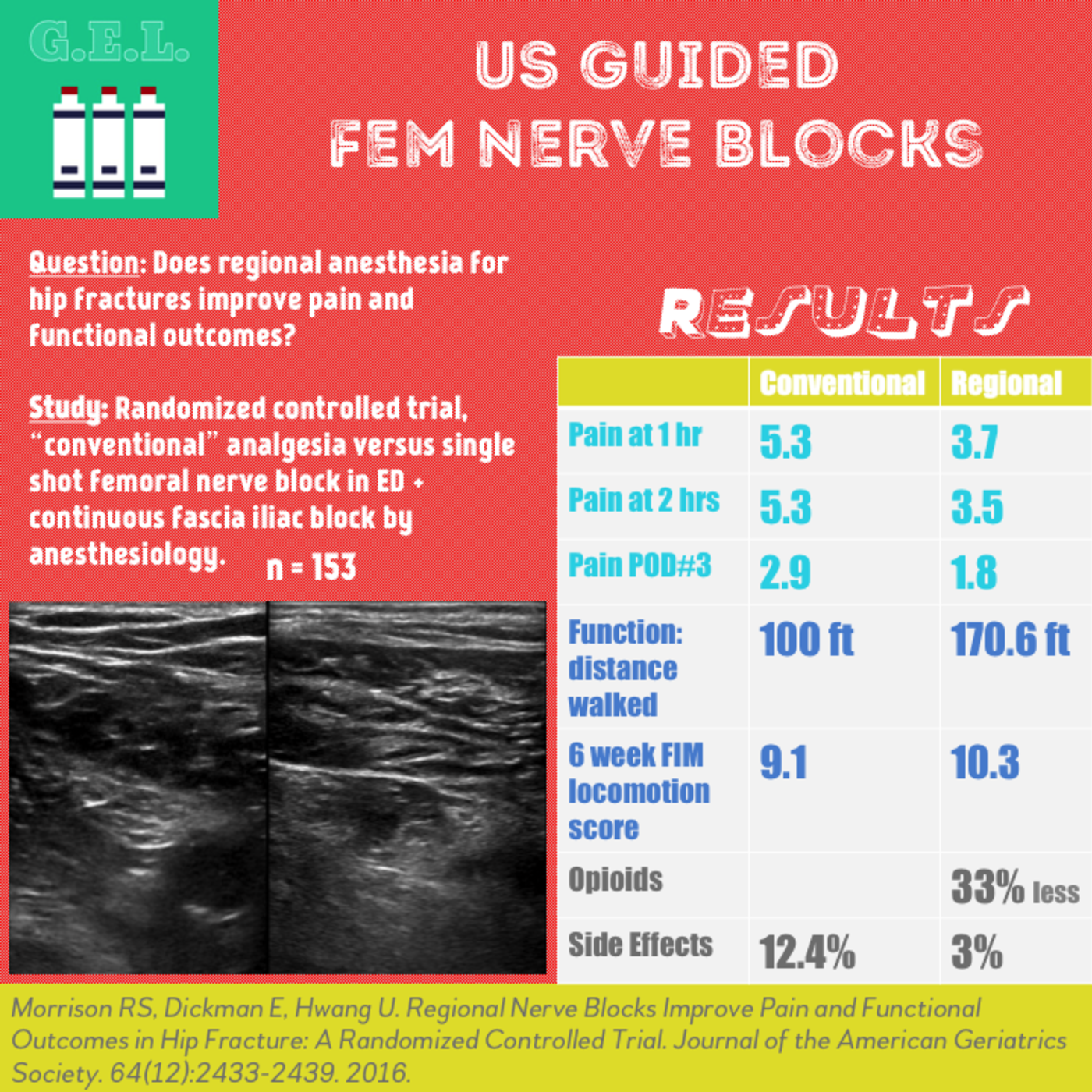
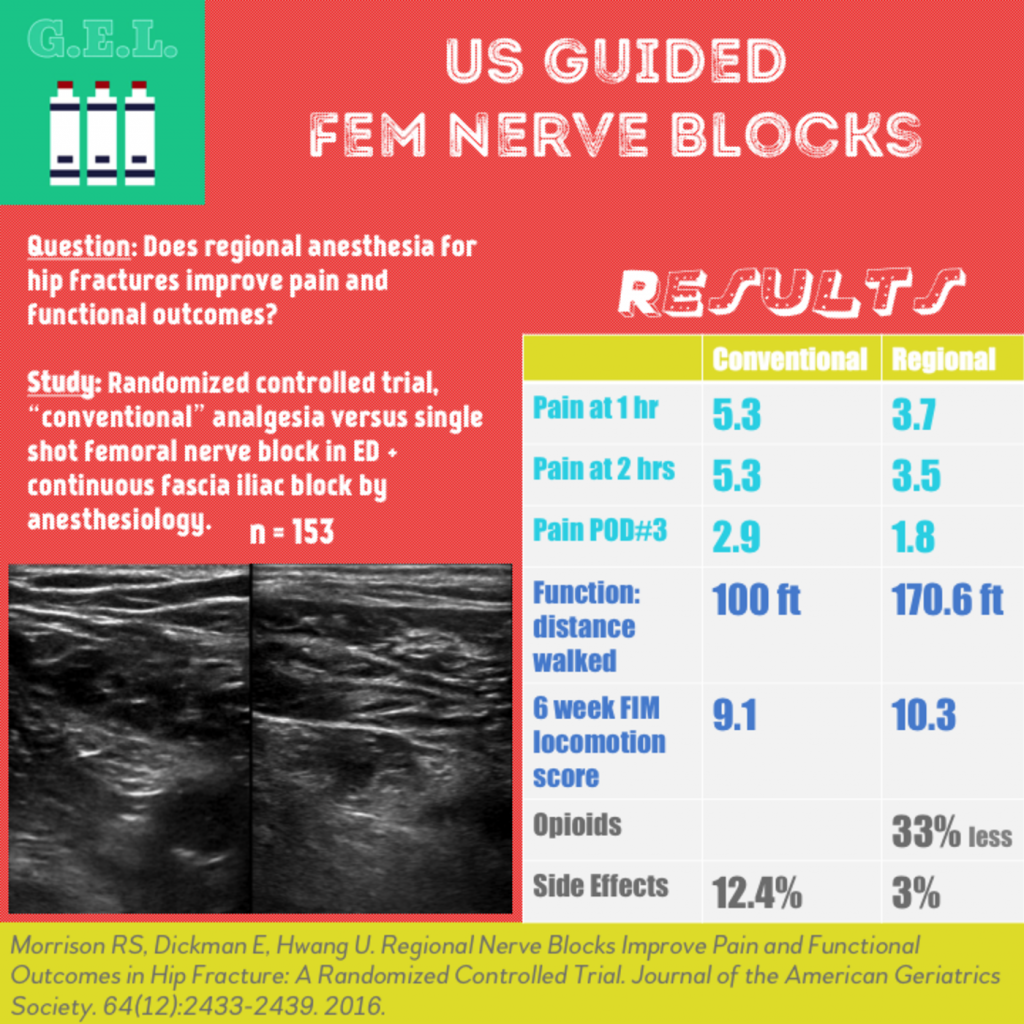
Regional Nerve Blocks Improve Pain and Functional Outcomes in Hip Fracture: A Randomized Controlled Trial
Journal of the American Geriatrics Society October 2016 – Pubmed Link
Take Home Points
1. A single shot femoral nerve block in the ED followed by anesthesiologist-performed continuous regional anesthesia is a feasible method of pain control in hip fracture.
2. This method of regional anesthesia resulted in better pain control, less opioids and related side effects, and better functional outcomes compared to control.
Background
Hip fractures are common. More than 250,000 adults over 65 years old are hospitalized for this annually. There is significant risk for loss of functional outcomes for this population (only 50% recover their ability for activities of daily living, only 54% can walk unaided after 1 year). Pain limits recovery and is associated with postoperative complications, less physical therapy, worse function. Opioids are not ideal for pain due to side effects. Regional anesthesia has been proven to be a great alternative. This is where ultrasound comes in. Besides anesthesiologists, most providers would likely not be comfortable performing landmark or nerve-stimulator guided peripheral nerve blocks. Ultrasound has made this much safer and easier.
Question
Does the use of regional anesthesia for hip fractures improve outcomes in pain in the emergency department, pain and function postoperatively, and pain and function 6 weeks after discharge?
Does the use of regional anesthesia for hip fractures decrease opioid requirements and side effect incidence?
Population
Three New York Emergency departments – all teaching hospitals
Inclusion
- Hip fracture (femoral neck, intertrochanteric, pericapsular) confirmed on radiography
- ≥60
- Consented
Exclusion
- Died before intervention
- Removal of fascia iliaca block catheter before post op day 3
- Not study related serious adverse event
- Withdrew consent or left against medical advice
- Lost to follow up
- Could not self-report pain (i.e. advanced dementia)
- Non-English, Spanish, or Russion speaking
- Anticoagulated
Who did the scans?
Training sessions at three study sites to all incoming emergency medicine residents and a core group of attending emergency physicians
1 hour didactic
30 minute hands-on training session – simulated patient encounters
Design
Randomized, controlled trial – conventional analgesic therapy versus femoral nerve block
Not physician blinded
Enrolled 8am to 8pm, Sunday to Friday, April 2009 to March 2013
Primary outcome measures:
- Pain 1 and 2 hours after ED admission
- Pain at rest, with transfers, and with walking on POD 3
- Distance walked in 2 minutes on POD 3
Secondary outcome measures:
- Opioid requirements (morphine equivalents)
- Opioid related side effects
- Number of physical therapy sessions missed or shortened
- FIM locomotion scores 6 weeks after discharge
Intervention
Femoral Nerve Block Arm (FNB)
Femoral nerve block in ED (see details of block in “the Block” below)
Continuous fascia iliaca block placed by anesthesiologist within 24 hours, until post operative day 3
As needed opioids at discretion of treating physicians
Control
Standing and as-needed parenteral and oral analgesics (opioids and acetaminophen)
No sham injections
Outcome Measurements
- Pain score on numeric rating scale 0-10
- Daily interviews (blinded) regarding pain and opioid side effects
- Confusion Assessment Method (CAM) and opioid side effects from chart review
- Physical performance testing on post-op day 3
- Telephone interview 6 weeks after discharge to assess walking ability
- Functional status assessed with Functional Independence Measure (FIM)
- Depression with Geriatic Depression scale
The Scan
Ultrasound Guided Femoral nerve block (as reported in this study)
- Linear probe
- Single shot (as opposed to continuous catheter infusion – which was performed by anesthesiologists later) of 20 mL of 0.5% bupivacaine
Femoral Nerve Block by Highland Ultrasound
Femoral Nerve Block by Ultrasound Podcast
Fascia Iliaca Compartment Block video by Mike Stone
Mike Stone’s classic lecture on ultrasound guided nerve blocks
Results
Intention to treat analysis
N = 153 for inhospital portion
- 72 intervention (FNB)
- 81 control
N = 108 for the 6 week follow up
Primary Outcomes
Pain
Pain at 1 hour – FNB 3.7 vs Control 5.3
Pain at 2 hours – FNB 3.5 vs Control 5.3
Pain POD 3:
- At rest – FNB 1.8 vs Control 2.9
- With transfers – FNB 4.7 vs Control 5.9
- With walking – FNB 4.1 vs Control 5.6
Function
Distance walked in 2 minutes – FNB 170.6 ft vs Control 100 ft
Secondary Outcomes
More in FNB were walking past their chair – FNB 82% vs Control 64%, OR 2.49
FNB less likely to miss or shorten PT – FNB 12.5% vs Control 27.2%, OR 0.38
At 6 weeks, FIM locomotion score (better walking and stairclimbing) – FNB 10.3 vs Control 9.1
FNB required 33% less parenteral morphine equivalents than controls in ED – FNB 0.8 mg/hr vs Control 1.2 mg/hr
Number of patients with severe side effects (defined as ≥1 days of nausea, sedation, unclear thinking) – FNB 3% vs Control 12.4%. OR 0.20
Delirium – FNB 15.9% vs Control 17.1, not statistically significant
No bleeding, falls, or catheter related infections in intervention group
Limitations
Possible placebo effect
Convenience sample
29% of population lost to 6 week follow up
Since this was a bundled treatment (ED single shot block + catheter) it is unknown which component is most important.
Exclusion of those with advanced dementia who might have benefited most from non-opioid therapy.
Functional benefits seen may not be specific to regional anesthesia, but could be a result of the superior pain control.
The resources and time invested in this pain control approach was not compared to the traditional approach. Setting up this type of protocol requires interdepartmental cooperation and communication.
Take Home Points
1. A single shot femoral nerve block in the ED followed by anesthesiologist-performed continuous regional anesthesia is a feasible method of pain control in hip fracture.
2. This method of regional anesthesia resulted in better pain control, less opioids and related side effects, and better functional outcomes compared to control.
Our score






1 thought on “Ultrasound G.E.L. – Ultrasound Guided Femoral Nerve Blocks for Hip Fractures”
Pingback: Höftblockad – Mind palace of an ER doc