
Written by: Nico Volz MD, Kelly Bogaert MD, and John Rozehnal MD (Emergency Resident Physicians, Icahn School of Medicine at Mount Sinai), Stephen Alerhand, MD (@SAlerhand – Emergency Physician and Ultrasound Fellow, Icahn School of Medicine at Mount Sinai) //
Edited by: Manpreet Singh, MD (@MPrizzleER – Assistant Professor in Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center)
52 yo F, with PMH fibroids and ovarian cystectomy, presenting with epigastric pain, nausea, vomiting, and decreased PO for 3-4 days. Decreased bowel sounds on exam with tenderness in epigastric region and RUQ, no apparent rebound or guarding.
T 36.5 P 63 BP 163/96 RR 20 SpO2 98% RA
Your differential at this point includes cholecystitis, biliary colic, pancreatitis, or gastritis. You decide to perform a RUQ ultrasound. You do not find any gallstones in the RUQ, though incidentally you find several dilated loops of bowel. Could it be a small bowel obstruction?
What is the utility of bedside US for SBO?
Gold standard for diagnosing SBO is surgical pathology, however this is not useful as a diagnostic tool in the ED. Historically, KUB’s are performed as an initial diagnostic test, followed by CT if they are indeterminate. However, abdominal X-ray has a sensitivity of 66-77% and specificity of 50-57%.[1]
A recent meta-analysis by Taylor and Lalani aimed to provide ED physicians with evidence-based data for the utility of ultrasound as an initial and accurate imaging modality to detect SBO. While the study points out that more data is needed (only 6 US studies met inclusion criteria), early results suggested that x-ray has limited utility with a positive likelihood ratio (+LR) of only 1.64, CT and MRI had +LRs of 3.6 and 6.77 respectively, whereas ultrasound had a +LR of 14.1 when performed by radiologists and 9.55 when performed as bedside US scans.[2] Further commentary based on this study brings into question whether we should stop considering plain film (acute abdominal series) as an initial diagnostic tool for evaluating SBO.[3]
One of the two bedside ED-performed studies reviewed in this meta-analysis was performed by Unluer et. al., who performed a prospective study of 174 patients presenting to the ED with suspected SBO.[4] The team trained EM residents to perform POCUS for SBO during a 3-hour session and with 5 practice scans. Studies were considered positive if 2 or more of these findings were present:
● Dilated loops of bowel in 3 segments
● Increased peristalsis
● Collapsed colonic lumen
They found a sensitivity of 97.7% and a specificity of 92.7%. These seem like good numbers!
How do I perform this?
1. Choose and position your probe: Select the highest frequency probe based on the patient’s body habitus—ideally, the curvilinear 3-5 MHz transducer in large adults.[5] Marker should be facing toward the patient’s right side.
2. Perform sequential graded compression with a transverse view starting in the RLQ and “mow the lawn” all the way to the LUQ. Then, mow the lawn longitudinally from the LLQ to the RUQ. Assess bowel compressibility as you go.

What am I looking for?
● Know which part of the bowel you are looking at, as size cutoffs suggestive of obstruction vary depending on location.
○ Large bowel will have visible haustra. If you are looking at large bowel and see the signs below, you may incorrectly diagnose SBO.
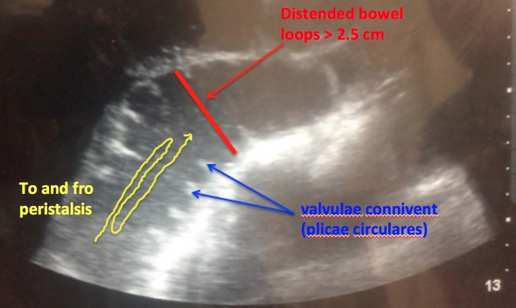
○ Jejunum will have “valvulae conniventes” on the interior aspect of the bowel wall, which appears like black and white keys of a piano (known as the keyboard sign).
○ Ileum will not have haustra or valvulae conniventes.
● Look for dilation. Dilation >25 mm in jejunum or >15 mm in ileum and present in more than three loops of bowel = SBO.[4]

● Look for “to-and-fro” motion (see video clip 1).[5]
(courtesy of Emergency Medicine at Hopital Universitairede Mirebalais)
(Courtesy of Joshua Guttman MD)
● Look for compressibility. Non-compressible small bowel proximal to collapsed, compressible bowel6. Lack of compressibility without a transition point does not equal SBO and may be seen in ileus.
● Look for free fluid and localized bowel wall edema (>2 mm thick) as these can be secondary signs of SBO.[6,7]
Key points
– Ultrasound is a fast and sensitive tool for identifying small bowel obstructions.
– The proper use of POCUS can expedite care, replace plain film radiography, reduce cost, reduce duration of stay, lead to expedited surgical consultations, and reduce unnecessary radiation.
– Studies have shown that emergency medicine physicians can accurately diagnose SBO with high sensitivity and specificity after a short amount of training.
Resources
1. Mallo RD et al. CT diagnosis of ischemic and complete obstruction in SBO: a sys review. J Gastrointest Surg. 2005;9:690–694.
2. Taylor MR, Lalani N. Adult Small Bowel Obstruction. Acad Emerg Med. 2013;20:528-44.
3. Carpenter CR, Pines JM. The End of X-rays for Suspected Small Bowel Obstruction? Using Evidence-based Diagnostics to Inform Best Practices in Emergency Medicine. Acad Emerg Med. 2013;20:618-20.
4. Unlüer EE1, Yavaşi O, Eroğlu O, et al. Ultrasonography by emergency medicine and radiology residents for the diagnosis of small bowel obstruction. Eur J Emerg Med. 2010 Oct;17(5):260-4.
5. Hefny AF, Corr P, Abu-Zidan FM. The role of ultrasound in the management of intestinal obstruction. Journal of Emergencies, Trauma and Shock. 2012;5(1):84–86.
6. Alerhand S, Koyfman A. Ultrasound for Small Bowel Obstruction. emDOCS. Oct. 2014. http://www.emdocs.net/ultrasound-small-bowel-obstruction/
7. Guttman, Joshua et al. Point-of-care ultrasonography for the diagnosis of small bowel obstruction in the emergency department. CJEM. 2014 Aug 1;16(0):30-3.
8. Noble, V. E., & Nelson, B. (2011). Manual of emergency and critical care ultrasound. Cambridge: Cambridge University Press
9. Rich, C POCUS for Appendicitis http://brownemblog.com/blog-1/2017/3/3/pocus-for-appendicitis Accessed 10/20/2017





2 thoughts on “US Probe: Ultrasound for Small Bowel Obstruction”
Pingback: Ileus – Ultraljud – Mind palace of an ER doc
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM: Small Bowel Obstruction - emDOCs.net - Emergency Medicine Education