Abdominal Aortic Aneurysm: Clinical Highlights and Updates
By Brian Febbo MD
Emergency Medicine Resident, Advocate Christ Medical Center
Edited by Alex Koyfman MD (@EMHighAK) and Stephen Alerhand MD (@SAlerhand)
Case Presentation
An 82 year-old female with a past medical history of hypertension, diabetes mellitus, and gout, presents with a chief complaint of abdominal and back pain. She receives an ESI Triage level 3 and is roomed in the Geriatric Wing of the ER. Initial vital signs are HR 102, BP 115/87, RR 20, T 37.2 ˚C, SpO2 98% on room air. On initial evaluation, the patient is noted to be mildly unwell-appearing, pale, and with diffuse abdominal tenderness to palpation but without rebound or guarding. She is administered a dose of morphine and ondansetron, basic labs are drawn, and she is sent to the Radiology department for a Stat CT Abdomen and Pelvis without contrast to further delineate the cause of her symptoms.
20 minutes later, she is rushed back from Radiology, moribund appearing and minimally responsive. Repeat exam shows significantly worsened abdominal distension. She quickly goes into cardiopulmonary arrest and, despite aggressive resuscitative efforts, is declared dead 45 minutes later.
Overview
The rupture of an Abdominal Aortic Aneurysm (rAAA) is a hallmark emergency medicine presentation with which all practitioners must be intimately familiar. Overall mortality of this condition approaches 90%, but survival with treatment is approximately 40-50%. The classic triad consists of abdominal or flank pain, hypotension and a pulsatile abdominal mass, but only manifests in 50% of cases at best. While many patients will present with a clear abdominal catastrophe, more occult presentations such as pain mimicking renal colic, syncope, acute lower extremity ischemia, or even lower extremity cyanosis mimicking phlegmasia cerulea dolens should raise the suspicion of the astute emergency clinician. A thorough understanding of this not uncommon and potentially deadly condition is essential for the practice of emergency medicine.
Definitions and Epidemiology
The normal aorta varies in size according to age, gender, and body habitus, but the average diameter in adults is less than 2.0 cm, so anything above 3.0 cm in diameter is considered aneurysmal.[i] Aneurysms are considered small if less than 4.0 cm in diameter, medium if 4-5.5 cm in diameter, large if 5.5-6 cm in diameter, and very large if > 6.0 cm in diameter. The risk of rupture increases with size and rate of expansion, with small aneurysms having a negligible risk.[ii] Abdominal aortic aneurysms are generally true aneurysms, in that they consist of pathologic dilatation of all 3 layers of the arterial wall, although mycotic (infected) aneurysms may be saccular and inflammatory aneurysms (which account for 2-10% of cases) are associated with primarily adventitial thickening[iii].
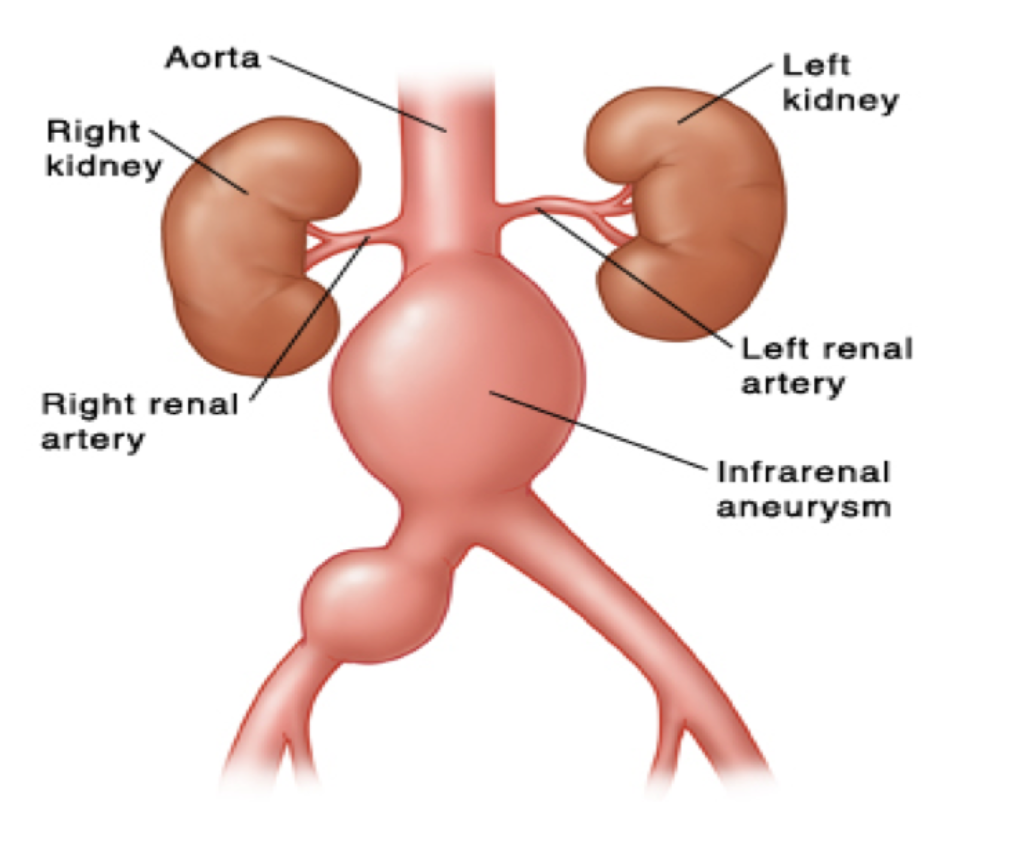
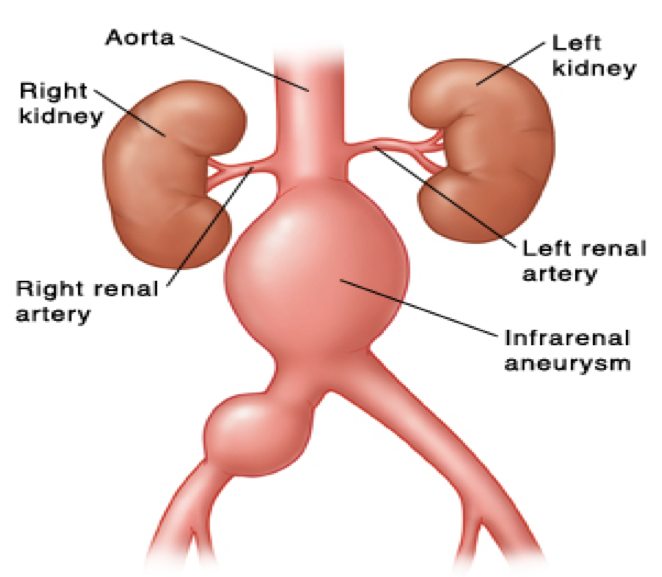
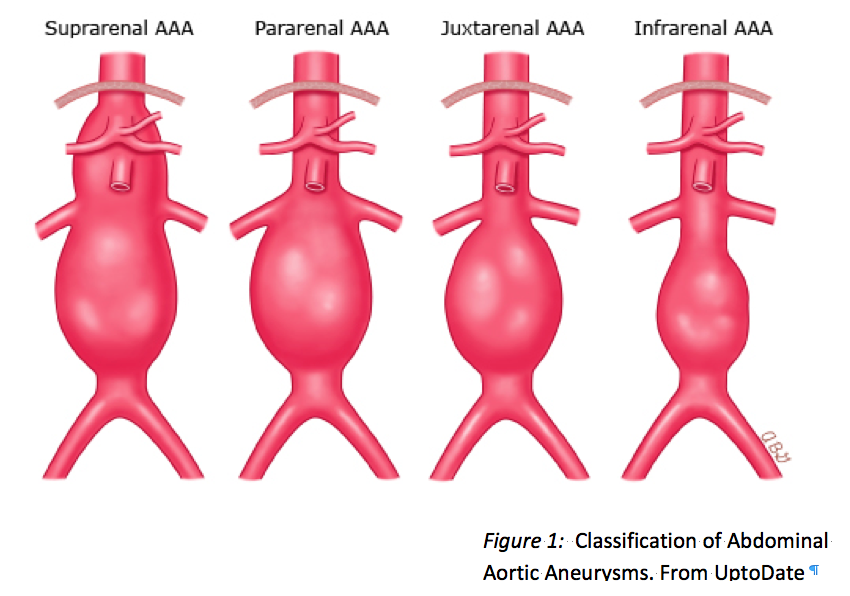
The majority of abdominal aneurysms are infrarenal, meaning the dilatation begins below the takeoff of the renal vessels. Less commonly, aneurysms may be suprarenal if they involve the takeoff of one of the visceral arteries but do not extend into the chest; pararenal if the renal but not superior mesenteric arteries arise from the aneurysm; or juxtarenal if at the junction of the renal artery takeoff (Figure 1). As discussed below, anatomic differences become important when considering whether the patient will be a candidate for endovascular aortic repair (EVAR).
AAA is the most common true aneurysm, with screening studies showing a prevalence of up to 4-8% in asymptomatic older men.[iv] The vast majority of those found on screening studies are small aneurysms, with clinically important ones measuring > 4.0 cm present in about 1% of men 55-65 years old, with prevalence increasing with age.[v] The condition is about 6 times more common in men as compared to women, and tends to develop 10 years later in women.[vi] Smoking is by far the most important risk factor, accounting for an estimated 75% of moderate-to-large aneurysms; other risk factors include white race, family history, atherosclerosis (especially peripheral vascular disease), and hypertension.[vii] Interestingly, diabetes is actually a negative risk factor despite its association with other cardiovascular disease; AAAs also tend to enlarge more slowly in diabetics. Although women have a much lower incidence of the condition, they are at higher risk for rupture and more often present this way. This condition accounts for about 15,000 deaths per year in the United States, making it the 13th leading cause of death[viii].
Asymptomatic AAAs
A full discussion of the management of the incidentally found or asymptomatic AAA is beyond the scope of this review. Yet, these will undoubtedly be encountered in practice and a basic understanding is warranted. Importantly, if a patient with a known or newly diagnosed AAA is having any flank or abdominal pain that cannot be unequivocally attributed to another process, they should be presumed to have a symptomatic AAA and admitted for vascular surgery consultation and urgent repair.
In general, however, most AAAs will be asymptomatic upon discovery. Referral to a vascular surgeon is generally advised for aneurysms with a diameter > 5.5 cm, although elective repair may be considered at smaller diameters for patients with predictors of rupture, such as female gender, rapidly expanding aneurysms, and patients with other arterial aneurysms or peripheral arterial disease. Aneurysms which do not require repair can be followed by primary care physicians with serial imaging. Emergent vascular surgery consultation should be obtained for patients found to have very large aneurysms (>6.0 cm), with consideration given to admission for pre-operative evaluation. Annual rates of rupture increase to 30-50% for aneurysms greater than 8.0 cm in diameter, and as definitive guidelines for the timing of elective repair have not been published, consultation with a vascular surgeon is advised to determine disposition for these patients.
All patients should be counseled on the need for ongoing surveillance. Although no intervention has been proven to limit enlargement, patients should be counseled on risk factor modification, with smoking cessation the most high-yield intervention. In addition, AAA is considered a coronary risk equivalent, so absent a contraindication, most patients should be on aspirin and statin therapy according to published guidelines.[ix]
Clinical Presentation
“There is no disease more conducive to clinical humility than aneurysm of the aorta”
-William Osler
The clinical manifestations of AAA are quite diverse. Frank intra-peritoneal rupture will generally manifest as sudden death, and these patients will rarely make it to the hospital alive. Indeed, it is estimated that only about half of all patients with ruptured AAAs survive long enough to undergo treatment. Acute severe pain is the most common presentation of rupture, occurring in about 75% of cases.[x] The location of pain will vary based on the site of rupture: proximal rupture near the renal vessels will lead to flank pain and mimic renal colic; contained anterior rupture will cause abdominal pain; and more distal posterior rupture can lead to a contained retroperitoneal hematoma causing severe focal back pain. Importantly, if the rupture stabilizes, the pain may subside, leading to a false sense of security for both the patient and clinician. There are also numerous reports of rAAAs causing radicular pain (either femoral or sciatic) due to nerve compression.
There are several presenting complaints aside from pain that should raise suspicion for a rAAA. Otherwise unexplained syncope or hypotension, even if transient, should prompt consideration of the condition. A subjective complaint of “feeling faint” is present in about 30% of patients. Sudden increases in intra-peritoneal pressure may cause an acute inguinal hernia, which can be misleading.[xi] Rupture into the inferior vena cava may produce acute heart failure and massive leg swelling with cyanosis, mimicking phlegmasia cerulea dolens.[xii] Acute lower limb ischemia may occur due to the distal embolism of thrombus, which can occur with or without acute rupture.
AAAs can be symptomatic without acute rupture as well. Generally, these will present with subacute pain in the flank or abdomen due to rapid enlargement and compression of surrounding structures. Inflammatory aneurysms, a distinct clinical entity which typically occur in younger patients and rupture less frequently, may be associated with chronic malaise, fevers, weight loss, and abdominal pain. Primary bacterial infection of the aortic wall causing mycotic aneurysms are rare but have been reported. These can result in primary aortoduodenal fistulas and cause massive GI bleeding, a complication typically associated with previous AAA repair.
Physical examination may offer clues to the diagnosis but will often be unrevealing. About half of patients with a rAAA will have a pulsatile mass palpable in the epigastrium,[xiii] so while insensitive, this can be an important clue to the diagnosis. A full vascular exam should be performed, and unequal carotid or radial pulses can point to a thoracic aortic dissection as a cause of the patient’s symptoms. Subcutaneous ecchymosis of the flank (Grey-Turner sign), periumbilical region (Cullen’s), proximal thigh (Fox’s), or scrotum (Bryant’s) may be present as well — these are neither sensitive nor specific. Importantly, any transient hypotension should be considered a red flag for this condition.
ED Management
Patients who present with symptoms of a possible rAAA should be considered at high risk for unpredictable hemodynamic collapse. Thus, appropriate management should include close monitoring—ideally in a room set up for resuscitation—and large bore peripheral access. Practitioners should hold a high index of suspicion for this condition, as initial misdiagnosis is common, occurring in about 40% of cases — the most common incorrect diagnoses being renal colic, myocardial infarction, and diverticulitis.[xiv] In general, further diagnostic and management pathways will depend on the hemodynamic status of the patient.
For the patient in clinical shock, diagnostic efforts must occur at the bedside in tandem with resuscitation. Although lab studies are not useful in making the diagnosis, basic chemistries, CBC, coagulation parameters, and fibrinogen will be useful for the ongoing treatment and blood product administration. Patients should be type and cross-matched for 6-10 units of PRBCs, with un-crossmatched type O blood made immediately available. The blood bank should be made aware of the likely need for FFP and platelets, and a massive transfusion protocol initiated. Fluid resuscitation of these patients should be performed in a manner analogous to patients with penetrating torso trauma, with controlled volume administration targeting a systolic blood pressure of 80-90 mmHg.[xv] While airway management may be necessary if the patient is obtunded or otherwise unable to protect their airway, ideally this is delayed until the patient is prepped and ready for surgery, as induction can precipitate hemodynamic collapse. Central access with a sheath introducer or a MAC catheter is advised in anticipation of the massive fluid requirements, but this should not delay transport to the OR. If the patient requires transfer to another center, sending several units of blood along with the patient would be advisable given the possibility of deterioration en route.
If a patient with a known history of AAA arrives unstable with symptoms consistent with rupture, no confirmatory diagnostic tests are necessary and the patient should be transferred to the OR expeditiously. Most patients, however, will require bedside imaging to confirm the diagnosis. Bedside ultrasound has emerged as the test of choice in this case. Ultrasound has a sensitivity of 98% in fasted patients undergoing screening, and while bowel gas and body habitus can hinder the exam, this is less of an issue in imaging the larger aneurysms that are likely to present ruptured. To obtain images of the aorta, a low frequency curvilinear probe is used. The probe is placed in the midline in the high epigastrium, and, using the liver as an acoustic window, gentle steady pressure is applied to displace bowel until the spine is visualized. The aorta will be seen as a round, hypoechoic structure on the patient’s left. (Figure 2) The sonographer should attempt to scan throughout the length of the aorta to the bifurcation (typically at the umbilicus), and should also obtain a sagittal view. Importantly, the diameter is measured from outer wall to outer wall, with > 3.0 cm being abnormal. If ultrasound is not available, a cross table lateral X-ray may show an AAA in up to 67% of cases. (Figure 3)
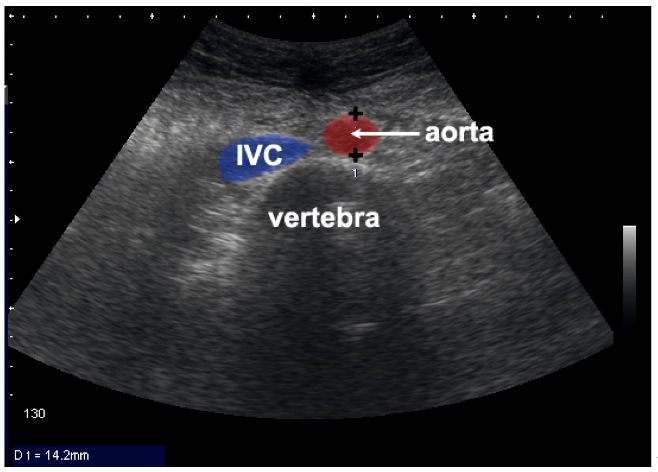

Figure 2: On the left, a normal sized Aorta, IVC and vertebra are labeled. On the right, a nearly 6 cm AAA is visualized. Images obtained from Dean AJ, Ku BS. Abdominal Aortic Aneurysm. Retrieved from: http://www.sonoguide.com/abdominal_aortic_aneurysm.html

Figure 3: A lateral abdominal X-ray showing the classic eggshell calcification of a AAA, confirming the diagnosis with 100% specificity. Image obtained from Radvany MG, Cho KJ. Abdominal Aortic Aneurysm Imaging. Retrieved from: http://emedicine.medscape.com/article
CT imaging of the abdomen is generally advised for hemodynamically stable patients, although US should be performed immediately in the patient with high clinical suspicion to aid in triage and to speed disposition. In addition to assessing for alternative conditions, CT provides important anatomic information about the AAA. Plain CT can usually determine whether the AAA is ruptured or merely symptomatic. Signs of rupture on CT include retroperitoneal hematoma or free intraperitoneal blood, an indistinct aortic wall, and loss of the normal fat plane around the aorta. Signs of ‘impending rupture’ or an unstable aneurysm may also be seen and include layering of hematoma within the aorta (‘crescent sign’), breaks in the calcification of the wall, and blebs or other irregularity within the wall[xvi]. The distinction between symptomatic and ruptured is critical, as the former can be admitted to the hospital for close monitoring and preoperative evaluation rather than emergent repair. Although contrast is not required for this determination, its administration is helpful to obtain more aortic detail for preoperative planning and to ascertain whether the patient is a candidate for EVAR.
EVAR has become the preferred method for the elective repair of AAAs in patients at high perioperative risk, and it has recently become more commonly applied for rAAAs as well. Although randomized trials have not borne out improved mortality rates for EVAR in this setting, it does appear that perioperative morbidity is decreased and thus EVAR is favored for anatomically suitable patients.[xvii],[xviii] About 70% of AAAs are anatomically suitable for EVAR, with the main criterion being an adequately long aneurysm neck to allow seating of the graft without occlusion of the renal arteries. (Although complex supra- and pararenal aneurysms may be amenable to EVAR on an elective basis, the grafts used need to be custom manufactured, which precludes emergent use.) In order to perform EVAR in this setting, the patient must be treated at an experienced center and the anatomy must be defined and deemed suitable. For the persistently unstable patient unable to undergo CT scanning, preoperative angiography in the OR may be an option. Whether the patient should be transferred to a referral center in order to undergo EVAR is a complex decision and is best made in consultation with an experienced vascular surgeon — although transfer may well become the norm given the decreased experience in open AAA repair among general surgeons in the current era.
Conclusion
Ruptured or symptomatic AAA is a critical condition with which the emergency physician should be familiar. Although not a condition one will see commonly, it is a rapidly fatal and time-sensitive condition that the EP must be ready for. Timely diagnosis with appropriate resuscitation and involvement of the operative team can mean the difference between life and death.
Take Home Points:
– Consider and rule out this diagnosis in ‘non-classic’ presentations such as isolated flank or back pain, syncope, unexplained hypotension, and lower limb ischemia.
– Bedside ultrasound is the key to early diagnosis in high risk patients.
– Resuscitation should target a low normal blood pressure with limitation of fluid administration, but be prepared for immediate massive transfusion if required.
– Be familiar with the recent shift towards endovascular repair in suitable patients
References / Further Reading:
[i] Johnston KW, Rutherford RB, Tilson MD, et al. Suggested standards for reporting on arterial aneurysms. Subcommittee on Reporting Standards for Arterial Aneurysms, Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery and North American Chapter, International Society for Cardiovascular Surgery. J Vasc Surg 1991; 13:452.
[ii] Chaikof EL, Brewster DC, Dalman RL, et al. SVS practice guidelines for the care of patients with an abdominal aortic aneurysm: executive summary. J Vasc Surg 2009; 50:880.
[iii] Rasmussen TE, Hallett JW Jr. Inflammatory aortic aneurysms. A clinical review with new perspectives in pathogenesis. Ann Surg 1997; 225:155.
[iv] Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP. Ultrasonography screening for abdominal aortic aneurysms: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med 2014; 160:321.
[v] Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med 2003; 348:1895.
[vi] Ibid.
[vii] Lederle FA, Johnson GR, Wilson SE, et al. The aneurysm detection and management study screening program: validation cohort and final results. Aneurysm Detection and Management Veterans Affairs Cooperative Study Investigators. Arch Intern Med 2000; 160:1425.
[viii] Wilmink AB, Quick CG. Epidemiology and potential for prevention of abdominal aortic aneurysm. Brit J Surg.1998;85:55–62
[ix] Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006; 113:e463.
[x] Rinckenbach S, Albertini JN, Thaveau F, et al. Prehospital treatment of infrarenal ruptured abdominal aortic aneurysms: a multicentre analysis. Ann Vasc Surg 2010; 24:308.
[xi] Khaw H, Sottiurai VS, Craighead CC, Batson RC. Ruptured abdominal aortic aneurysm presenting as symptomatic inguinal mass: report of six cases. J Vasc Surg 1986; 4:384.
[xii] Salo JA, Verkkala KA, Ala-Kulju KV, et al. Hematuria is an indication of rupture of an abdominal aortic aneurysm into the vena cava. J Vasc Surg 1990; 12:41.
[xiii] Azhar B, Patel SR, Holt PJ, et al. Misdiagnosis of ruptured abdominal aortic aneurysm: systematic review and meta-analysis. J Endovasc Ther 2014; 21:568.
[xiv] Ibid.
[xv] Dick F, Erdoes G, Opfermann P, et al. Delayed volume resuscitation during initial management of ruptured abdominal aortic aneurysm. J Vasc Surg 2013; 57:943.
[xvi] Siegel CL, Cohan RH, Korobkin M, et al. Abdominal aortic aneurysm morphology: CT features in patients with ruptured and nonruptured aneurysms. AJR Am J Roentgenol 1994; 163:1123
[xvii] van Beek SC, Conijn AP, Koelemay MJ, Balm R. Editor’s Choice – Endovascular aneurysm repair versus open repair for patients with a ruptured abdominal aortic aneurysm: a systematic review and meta-analysis of short-term survival. Eur J Vasc Endovasc Surg 2014; 47:593.
[xviii] Antoniou GA, Georgiadis GS, Antoniou SA, et al. Endovascular repair for ruptured abdominal aortic aneurysm confers an early survival benefit over open repair. J Vasc Surg 2013; 58:1091.
19 http://www.ncbi.nlm.nih.gov/pubmed/23406071
20 http://www.ncbi.nlm.nih.gov/pubmed/18614326





1 thought on “Abdominal Aortic Aneurysm: Clinical Highlights/Updates”
Pingback: Best Case Ever | Ruptured AAA | EM Cases : Emergency Medicine Cases