Case:
A 62-year-old female with a history of diabetes and end stage renal disease (ESRD) on dialysis presents to the Emergency Department with chief complaint of shortness of breath, malaise and subjective fevers. The patient reports progressive shortness of breath with dyspnea on exertion over one month with malaise over the same duration and fevers in past 2 days. Additional symptoms include anorexia, myalgias, headache and chills. The patient denies cough, recent travel or known sick contacts. She is febrile, tachycardic, and mildly hypoxic and in mild respiratory distress. She has poor dentition and an audible cardiac murmur. The rest of her examination is non-focal.
What should you consider in the differential diagnosis and what are the next steps to evaluate and treat this patient?
Epidemiology:
Infectious Endocarditis (IE) is a rare infection, affecting approximately 3 to 10 per 100,000, with studies indicating that the incidence in rising and occurring in patients without known heart disease.1 Despite efforts made towards early treatment, the mortality approaches 20% at 30 days and greater than 30% within the first year of being diagnosed.2 In the United States, there are approximately 40,000 new cases of IE per year with mean hospital charges greater than $120,000 per patient.3, 4
Risk factors:
The patient’s past medical, surgical and social history are pertinent clues to their risk of developing infectious endocarditis. Endocarditis occurs as a result of infection of the endocardial surface, which can happen due to turbulent, high-pressure flow in certain cases, particularly in cases with valvular or cardiac structural defects. Additionally, hypercoagulable or inflammatory states may predispose patients to this infection.5
- Patients with a history of underlying cardiac disease including rheumatic heart disease, congenital heart disease, a history of heart surgery or a history of endocarditis are at risk for development of IE.
- Rheumatic heart disease in developed countries is much less common and continues to decline as the condition is more frequent in elderly patients, so is less often a cause of IE in these countries.5, 6 However, in developing countries, IE affects a younger age group, is often associated with rheumatic heart disease, and is predominantly caused by streptococci.7
- Infective endocarditis is rare in children, although the improved survival in congenital heart disease has resulted in increasing incidence in recent decades with the highest risk in those with cyanotic congenital heart disease, endocardial cushion defects, or ventricular septal defects.8 A recent European study evaluated the incidence ofIE from 2000 to 2018 with 21% of the 641 cases being related to adults with congenital heart disease.9 Specific predictors of IE in patients with congenital heart disease include those with prosthetic valves and valve repairs containing conduits as well as those with multiple cardiac defects.6
- Prosthetic valve replacement remains a significant risk factor for development of IE as the prosthetic valve serves as a nidus for infection and may place the patient at risk for infection with a multitude of bacteria including aureus, coagulase-negative staphylococci and Enterococcus species.5, 6, 8
- IVDA continues to be one of the highest risk factors for the development of IE. The proportion of IVDU-associated IE increased from 7.1% to 12.1% from 2000-2013, particularly with patients aged 15 to 34 years old.10 The majority of patients with IVDU-associated IE do not have underlying cardiac disease with approximately 50% of infections affecting the tricuspid valve due to aureus.5
- Immunosuppression (due to HIV, vasculitis, diabetes or malignancy) and hemodialysis remain risk factors for any infection, including IE. aureus remains the most common bacteria to cause bacteremia and subsequently IE in these patient populations.5
- Surgical hardware placement including pacemakers and defibrillators places the patient at risk for nosocomial IE (NIE). More than 50% of NIE is diagnosed in patients greater than 60 years old compared to the 21% of community-acquired IE in the same age group.11 Pacemaker IE is most commonly due to aureus, occurring between 2 days after hospitalization to 4 weeks after the surgical procedure.5 Additionally, indwelling venous catheters, poor surgical technique and the development of hematomas will also place the patients at risk for infection and subsequent diagnosis of IE.5
- Poor oral hygiene: Oral streptococci comprise approximately 20% of bacterial endocarditis cases.12 It is debated whether antibiotic therapy will prevent or reduce bacteremia prior to dental procedures. There are no prospective, randomized placebo-controlled studies regarding the benefit or utility to prevent IE with antibiotic prophylaxis. The consensus from several studies is that a considerable amount of prophylaxis would need to be prescribed to prevent very few cases of IE in higher risk populations. The vast majority of cases of IE that occur as a result of oral microflora are likely due to daily activities including chewing, toothbrushing, use of toothpicks and other similar activities so prevention with focus on better oral hygiene may be more effective at decreased cases of IE.1, 12
Presentation:
The largest challenge regarding IE is the variability in clinical presentation, which ultimately leads to delayed diagnosis and subsequent treatment.1
- Systemic symptoms include fever, malaise, weakness, arthralgias and weight loss.1
- Cardiac complications occur in up to 50% of patients, including congestive heart failure, valvular insufficiency and valve rupture, conduction system deficits with resulting dysrhythmias or heart block. New murmurs may not be present initially but can occur in up to 85% of cases and may vary from an early diastolic murmur or short mid-diastolic “rumbling” Austin-Flint murmur (from aortic regurgitation) to a systolic murmur (from mitral regurgitation).5, 13
- Central nervous system manifestations occur in 33-50% of patients and include embolic occlusion of arteries, cerebral hemorrhage and infections of the CNS (such as meningitis, encephalitis or abscess). Emboli occur in 20% of cases of IE with embolic strokes occurring more commonly due to aureus and Streptococci with mortality reaching 40% .5
- Dermatologic manifestations occur in 5-15% of cases. Janeway lesions (painless hemorrhagic lesions on the hands or feet), Osler’s nodes (tender nodular red lesions on the hands or feet) and splinter hemorrhages
- Ophthalmologic findings include subconjunctival hemorrhages and retinal hemorrhages, a.k.a. Roth spots. While Roth spots are most commonly associated with the diagnosis of IE and have been previously quoted to be found in 80% of subacute bacterial endocarditis, this diagnosis is not specific and can be associated with many other diagnoses.5
- Pulmonary symptoms may be the result of pulmonary embolus, pulmonary infarction, abscess or pneumonia. Pulmonary emboli are more commonly associated with IVDU, affecting the tricuspid valve and right sided IE.5, 6
- Renal manifestations may result from emboli or infection. Renal emboli may result in ischemia, infarct or abscess. Additionally, a patient infected with IE may have renal failure or glomerulonephritis.5, 14
- Vascular phenomena associated with the diagnoses of IE also include mycotic aneurysms and emboli may also lead to infarcts of the spleen.5, 15
Evaluation:
Laboratory assessment:
- CBC, renal function panel, liver function test, CRP/ESR, lactic acid and urinalysis have been suggested as a minimum for evaluation of a patient suspected to have IE. The WBC is neither sensitive nor specific and may be elevated, depressed or normal although it is elevated in 50% in patients with IE.5 Similarly, the CRP and ESR are not sensitive nor specific and may be normal or elevated.16 Renal function may be decreased as a result of renal emboli, renal infarcts or glomerulonephritis. The urinalysis may reveal hematuria in 50% due to renal emboli.5.
- Blood cultures – a minimum of 3 from separate sites obtained at least 1 hour apart15 is recommended for diagnosis via the Duke criteria. However, this is not always feasible in an acutely ill patient in the Emergency Department. The goal should be to obtain 2-3 blood cultures from separate sites with cultures bottles filled completely to increase sensitivity of detecting blood stream infections.17
- ECG – may demonstrate ischemia or conduction abnormalities including heart blocks.5
Imaging:
- Chest X-ray – may demonstrate evidence of heart failure or may demonstrate multiple infiltrates in the setting of right-sided IE with multiple septic pulmonary emboli5
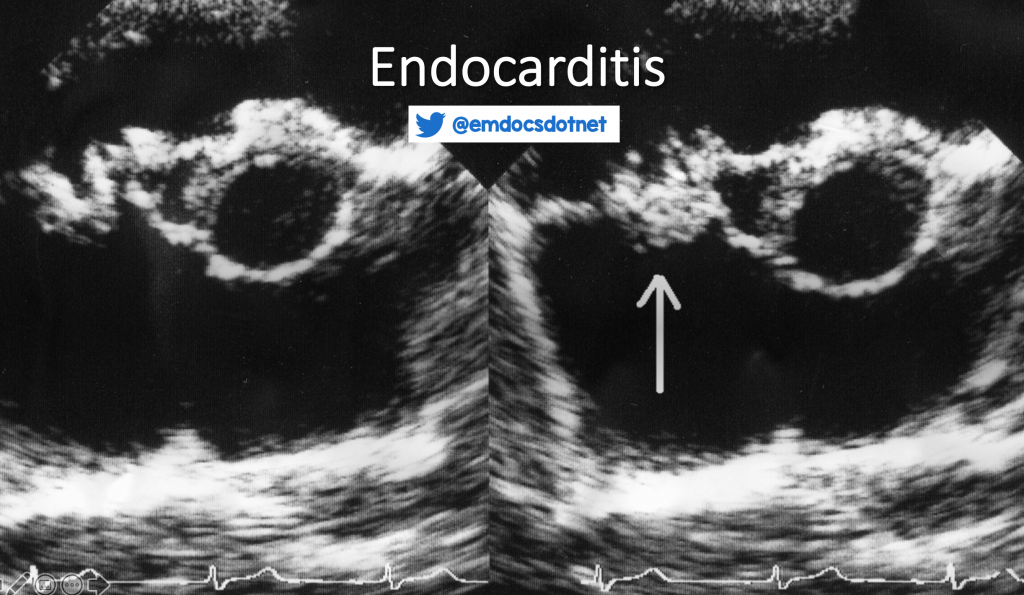
- Echocardiogram – TTE is first line imaging with a sensitivity rate of 40-60% and is the cornerstone for initial evaluation of patients with suspected IE. If TTE is non-diagnostic, the patient should be evaluated with TEE which has a sensitivity of 90%.6, 15
- Cardiac CT has similar diagnostic accuracy compared to TEE and less invasive but smaller vegetations (<4mm) may be missed on cardiac CT. An advantage of CT over TEE is in the detection of perivalvular extension of infection and pseudoaneurysms.6
- MRI may be used to diagnose cerebral embolic events, aide in early diagnosis of IE and the results may affect surgical planning, particularly the timing of surgery.6
*Blood cultures and echocardiogram are required to make diagnosis with the Modified Duke Criteria.15
Diagnosis:
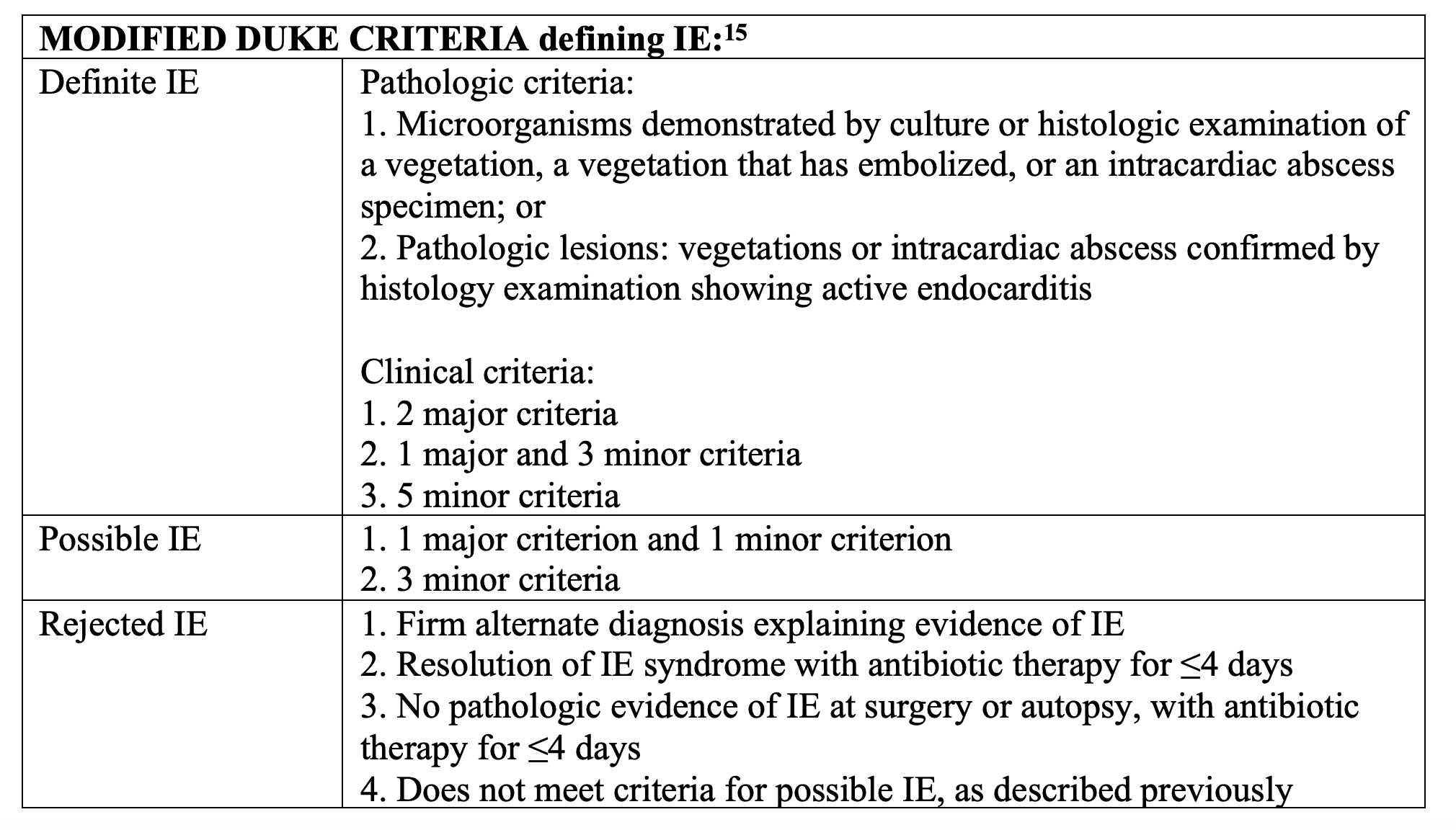
The diagnosis of IE requires consideration of all pertinent history and physical examination findings that will place a patient at risk. While the Duke criteria has been modified to increase the sensitivity in diagnosis of IE, it is a tool for clinicians to use with the majority of information that has been gathered after a patient has been admitted to the hospital. As Emergency Physicians seeing the patient initially, we can have a higher level of concern for IE in patients with fever or flu-like illness, risk factors (listed above) and any of the following:
- Known positive blood cultures
- Echocardiogram findings consistent with IE
- New or worsening murmur (concerning for valvular regurgitation)
- Vascular phenomena
- Major arterial emboli
- Septic pulmonary infarcts
- Mycotic aneurysm
- Intracranial hemorrhage or CVA
- Conjunctival hemorrhages
- Janeway’s lesions
- Glomerulonephritis
- Osler’s nodes
- Roth’s spots
- Rheumatoid factor
Patients with fever and/or infection such as meningitis, encephalitis, pneumonia, or abscesses (of the brain, kidney or lungs) with risk factors for developing IE may have endocarditis as the underlying cause to their primary diagnosis.

Management:
- Antibiotics:
- Native valve endocarditis is most commonly due to aureus, viridans group streptococci, Streptococcus gallolyticus (bovis), Enterococcus species, HACEK (Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella species) organisms) organisms.Prosthetic valve endocarditis is most commonly caused by S. aureus, coagulase-negative staphylococci, Enterococcus species. The following regimen is recommended for initial ED management to cover both native and prosthetic valve IE:
- Vancomycin 20 mg/kg IV loading dose and then 15 mg/kg every 12 h AND
- Cefepime 2 g IV every 8 h
- *If patient has a severe penicillin allergy, substitute Cefepime with Aztreonam 2g IV every 8 hours
- Native valve endocarditis is most commonly due to aureus, viridans group streptococci, Streptococcus gallolyticus (bovis), Enterococcus species, HACEK (Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella species) organisms) organisms.Prosthetic valve endocarditis is most commonly caused by S. aureus, coagulase-negative staphylococci, Enterococcus species. The following regimen is recommended for initial ED management to cover both native and prosthetic valve IE:
- Aminoglycosides (i.e. Gentamicin) were recommended historically for all patients with prosthetic valves, particularly to cover enterococcal infection, however multiple studies have indicated that this is causing increased renal injury without benefit to many patients.5 The combination of ampicillin and aminoglycosides has been deemed essential for at least the first 2 weeks of treatment to reduce the risk of relapse in endocarditis caused by faecalis, but Emergency Physicians do not often have the results of blood cultures and sensitivities prior to admitting the patient.18 For patients with prosthetic valves or speciated blood cultures at admission with enterococcus species, aminoglycoside coverage may be added to broaden coverage. Consideration of adding Gentamicin, Ampicillin or Rifampin should be discussed with the admitting physician.5, 6, 18
- Surgery: More than 50% of patients with endocarditis will need valve surgery within their initial hospitalization. Consultation with CT surgery in the ED is recommended in several situations. Surgical indications include:
- Treatment-refractory heart failure
- Cardiogenic shock or persistent pulmonary edema due to valvular insufficiency
- Persistent infection despite appropriate antibiotics
- Fungal or pseudomonal infection
- Multiple emboli
- Valvular complications including dehiscence, perforation, fistula or large perivalvular abscess5
*Surgery is not indicated for IE associated with IVDU due to the high rate of recurrence.5
*Surgery is contraindicated for at least one month after intracranial hemorrhage.19
Emergency surgery should be performed for patients within 24 hours if patients have endocarditis with severe congestive heart failure or cardiogenic shock caused by:
- Aortic valvular regurgitation
- Severe prosthetic dysfunction (dehiscence or obstruction)
- Or fistula into the cardiac chamber or pericardial space.
Urgent surgery should be performed for patients within days if they have:
- Native valve endocarditis with persisting congestive heart failure, signs of poor hemodynamic tolerance, or abscess
- Prosthetic valve endocarditis with persisting congestive heart failure, signs of poor hemodynamic tolerance, or abscess
- Prosthetic valve endocarditis caused by staphylococci or Gram-negative organisms
- Large vegetation (>10 mm) with an embolic event
- Large vegetation (>10 mm) with other predictors of a complicated course
- Very large vegetation (>15 mm), especially if conservative surgery is available
- Large abscess and/or periannular involvement with uncontrolled infection
Early elective surgery should be performed (during the in-hospital stay) if the patient has:
- Severe aortic or mitral regurgitation with congestive heart failure and good response to medical therapy
- Prosthetic valve endocarditis with valvular dehiscence or congestive heart failure and good response to medical therapy
- Presence of abscess or periannular extension
- Persisting infection when extracardiac focus has been excluded19
Cognitive Biases:

Why are we missing this diagnosis as a result of these cognitive biases?
- Vague symptoms. Symptoms of IE may be initially indistinguishable from other more common diagnoses. Particularly in flu season, or in light of COVID 19, it is a common mistake to anchor on more simple diagnoses including viral illness and not keeping a broader differential.20
- Failure to identify risk factors. We often fail to consider the numerous risk factors predisposing patients to IE, such as underlying cardiac disease or valve replacement, immunocompromised state, IVDA, hemodialysis patients or patients at risk for nosocomial infection.1, 5
- Incomplete physical exams. We may be guilty of not performing a full physical examination and potentially missing some of pertinent physical exam findings. While not always present, cardiac murmurs, Janeway lesions, Osler nodes, Roth spots, splinter hemorrhages, embolic skin lesions are all helpful clues for the diagnoses.1, 21
- The patient may have multiple diagnoses. The patient with IE may have additional and more clinically evident diagnoses, including but not limited to pneumonia, meningitis, acute heart failure, acute myocardial infarction or stroke.13 It is essential to pursue co-existing diagnoses or underlying causes of the primary diagnosis in order to avoid search satisfying.
- Additionally, particularly given that IE is rare, it is less likely to be within the top few diagnoses that are being considered in our deadly differential. We may be guilty of not considering the diagnosis in the differential. This is an example of premature closure.
How can we improve?
- Always be consistent and perform a thorough history and physical examination so you don’t miss subtle findings that can clue you into this diagnosis.
- Consider the diagnosis of IE in patients with underlying cardiac disease (rheumatic heart disease, congenital heart disease, prosthetic valve replacement), IVDA, hemodialysis, immunosuppression (HIV, vasculitis, diabetes, malignancy) or those at risk for nosocomial infections (indwelling venous catheters, surgical hardware placement or recent surgery) and patients with poor oral hygiene.
- Have a higher level of concern for IE in patients with risk factors and known positive blood cultures, echocardiogram findings consistent with IE, new murmur (concerning for valvular regurgitation), fever >38°C (particularly of unknown origin). vascular phenomena, major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway’s lesions, or immunologic phenomena (glomerulonephritis, Osler’s nodes, Roth’s spots). Use the Modified Duke Criteria to aide in diagnosis for high-risk patients.
- Obtain an echocardiogram and three sets of blood cultures from different sites (ideally obtained >1 hour apart and bottles filled completely) in patients who are at risk for IE.
- Start the appropriate antibiotics as soon as IE is identified as possible (usually Vancomycin and Cefepime IV). In patients with prosthetic valves or at risk for enterococcus bacteremia consider addition of Gentamicin.
- Consult CT surgery for patients with IE with severe congestive heart failure or cardiogenic shock caused by aortic valvular regurgitation, severe prosthetic dysfunction (dehiscence or obstruction) or fistula into the cardiac chamber or pericardial space.
- Do not anchor or forget that your patient may have more than one critical diagnosis and that IE may be an underlying cause to your primary diagnosis (such as stroke, meningitis, or pulmonary emboli).
Pingback:
http://www.emdocs.net/em3am-endocarditis/
http://www.emdocs.net/r-e-b-e-l-em-bacterial-endocarditis/
http://www.emdocs.net/the-em-educator-series-endocarditis-how-to-put-all-of-the-findings-together/
References:
- Cahill TJ, Baddour LM, Habib G, et al. Challenges in Infective Endocarditis. J Am Coll Cardiol. Jan 24 2017;69(3):325-344. doi:10.1016/j.jacc.2016.10.066
- Vincent LL, Otto CM. Infective Endocarditis: Update on Epidemiology, Outcomes, and Management. Curr Cardiol Rep. Aug 16 2018;20(10):86. doi:10.1007/s11886-018-1043-2
- Bor DH, Woolhandler S, Nardin R, Brusch J, Himmelstein DU. Infective endocarditis in the U.S., 1998-2009: a nationwide study. PLoS One. 2013;8(3):e60033. doi:10.1371/journal.pone.0060033
- Slipczuk L, Codolosa JN, Davila CD, et al. Infective endocarditis epidemiology over five decades: a systematic review. PLoS One. 2013;8(12):e82665. doi:10.1371/journal.pone.0082665
- Long B, Koyfman A. Infectious endocarditis: An update for emergency clinicians. Am J Emerg Med. Sep 2018;36(9):1686-1692. doi:10.1016/j.ajem.2018.06.074
- Hubers SA, DeSimone DC, Gersh BJ, Anavekar NS. Infective Endocarditis: A Contemporary Review. Mayo Clin Proc. 05 2020;95(5):982-997. doi:10.1016/j.mayocp.2019.12.008
- Yew HS, Murdoch DR. Global trends in infective endocarditis epidemiology. Curr Infect Dis Rep. Aug 2012;14(4):367-72. doi:10.1007/s11908-012-0265-5
- Cahill TJ, Prendergast BD. Infective endocarditis. Lancet. Feb 2016;387(10021):882-93. doi:10.1016/S0140-6736(15)00067-7
- Ly R, Compain F, Gaye B, et al. Predictive factors of death associated with infective endocarditis in adult patients with congenital heart disease. Eur Heart J Acute Cardiovasc Care. Jan 2020;doi:10.1177/2048872620901394
- Wurcel AG, Anderson JE, Chui KK, et al. Increasing Infectious Endocarditis Admissions Among Young People Who Inject Drugs. Open Forum Infect Dis. Sep 2016;3(3):ofw157. doi:10.1093/ofid/ofw157
- Giamarellou H. Nosocomial cardiac infections. J Hosp Infect. Feb 2002;50(2):91-105. doi:10.1053/jhin.2001.1144
- Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. Oct 2007;116(15):1736-54. doi:10.1161/CIRCULATIONAHA.106.183095
- Jolobe OMP. Acute presentations of infective endocarditis. Am J Emerg Med. Mar 2019;37(3):557-558. doi:10.1016/j.ajem.2018.07.051
- Satoskar AA, Parikh SV, Nadasdy T. Epidemiology, pathogenesis, treatment and outcomes of infection-associated glomerulonephritis. Nat Rev Nephrol. 01 2020;16(1):32-50. doi:10.1038/s41581-019-0178-8
- Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. Apr 2000;30(4):633-8. doi:10.1086/313753
- Heiro M, Helenius H, Sundell J, et al. Utility of serum C-reactive protein in assessing the outcome of infective endocarditis. Eur Heart J. Sep 2005;26(18):1873-81. doi:10.1093/eurheartj/ehi277
- Lamy B, Dargère S, Arendrup MC, Parienti JJ, Tattevin P. How to Optimize the Use of Blood Cultures for the Diagnosis of Bloodstream Infections? A State-of-the Art. Front Microbiol. 2016;7:697. doi:10.3389/fmicb.2016.00697
- Cuervo G, Escrihuela-Vidal F, Gudiol C, Carratalà J. Current Challenges in the Management of Infective Endocarditis. Front Med (Lausanne). 2021;8:641243. doi:10.3389/fmed.2021.641243
- Prendergast BD, Tornos P. Surgery for infective endocarditis: who and when? Circulation. Mar 2010;121(9):1141-52. doi:10.1161/CIRCULATIONAHA.108.773598
- Prakash S, Bihari S, Need P, Sprick C, Schuwirth L. Immersive high fidelity simulation of critically ill patients to study cognitive errors: a pilot study. BMC Med Educ. Feb 8 2017;17(1):36. doi:10.1186/s12909-017-0871-x
- Chellis M, Olson J, Augustine J, Hamilton G. Evaluation of missed diagnoses for patients admitted from the emergency department. Acad Emerg Med. Feb 2001;8(2):125-30. doi:10.1111/j.1553-2712.2001.tb01276.x





1 thought on “Endocarditis: Why do we miss it, and how do we improve?”
From Dr. David Talan:
Nice article. a couple points to add if you don’t mind…
Your recommended empiric regimen is fine although I’d have referenced vancomycin + ceftriaxone from this NEJM review (https://www.nejm.org/doi/full/10.1056/NEJMcp2000400). The 2015 AHA guidelines do not offer advice on an empirical regimen and just say consult ID.
Note that ceftriaxone is active against Enterococcus and is used with ampicillin, further reason to spare the patient an aminoglycoside and also choose ceftriaxone over cefepime (Enterococcus being much more common than Pseudomonas; it’s not clear that cefepime is active in this way). But vanco and cefepime is fine too. No one expects we cover every possibility, and most blood cultures now result with ID in <24 hours.
The NEJM review addresses native valve endocarditis, and if there is a prosthetic valve, then recommendations are not as clear and many recommend vancomycin with gentamicin and rifampin. Personally, I feel there is a shift away from aminoglycosides as the benefit of "synergy" has been challenged and especially in those elderly patients with prosthetic valves who are more prone to toxicities. Besides, ED MDs know vancomycin and ceftriaxone well. I just add rifampin if it's a prosthetic valve to show the admitting service some je ne sais quoi. let the admitting service start the aminoglycoside.
Finally, there are suspected cases and then there are possible cases, where let's say a patient has viral URI type symptoms but still with the fever, one has to consider endocarditis. This comes up more than you might suspect. It's acceptable to get a TTE (and other screening labs) in the ED and, if negative, after drawing BCs, give daptomycin (q24 hrs) and ceftriaxone and d/c home, arranging close f/u with their cardiologist or PCP.
dt