Author: Sumintra Wood, MD (EM Resident Physician, Mount Sinai Hospital, New York, NY)
Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident, SAUSHEC, USAF)
A 62 year-old man with a history of HTN, CHF s/p LVAD on coumadin is brought in by EMS after he passed out three times this afternoon. Currently the patient feels well, denying any chest pain, dyspnea, headache, or fever.
His vitals are: T 36.3oC, HR 169, SpO2 100% RA, RR 16, BP unmeasurable.
His EKG shows:
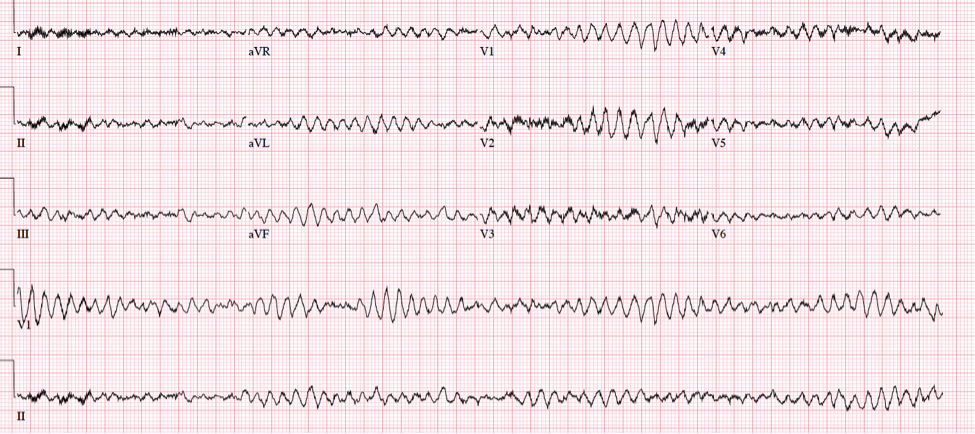
What do you do next?
Well, you need to figure out if your patient is actually stable or unstable.
Since LVAD patients do not typically have palpable peripheral pulses and blood pressures that can be measured by automated cuffs, first use US to get your patient’s MAP.
Attach a manual BP cuff to your patient’s arm, inflate > 120 mm Hg, then slowly deflate it while having the Doppler US probe over the brachial artery. The pressure reading at which arterial flow becomes audible (or visible) = MAP.
A normal MAP is 60-90 mm Hg. Your patient’s is 45.
To recap, your well-appearing LVAD patient is actually hypotensive, in torsades. If this is not corrected quickly your patient is at risk for right ventricular failure and death.
With the assistance of your LVAD team you perform procedural sedation and defibrillate your patient with conversion to sinus rhythm.
The patient heads up safely to the CCU, but you’re still left wondering what other LVAD emergencies you need to be prepared to handle.
Let’s start with LVADs themselves…
Left ventricular assist devices (LVADs) are mechanical circulatory pumps that improve perfusion in patients with severe LV dysfunction and heart failure.
LVADs can be used as a bridge to myocardial recovery, transplantation, or as destination therapy.1
The LVAD is placed in the upper abdomen and connected to an external power supply. Blood travels through a tube in the left ventricle into the LVAD, which pumps blood through another tube into the aorta and throughout the body.
 Types of LVADs:
Types of LVADs:
1st generation devices – no longer in use.
2nd generation devices – most commonly found currently. Smaller than first generation and have continuous non-pulsatile flow (decreases risk of hemolysis due to shear stress on RBCs but also means no palpable pulse, difficulty determining BP from automated cuff).2
3rd generation devices – may help minimize thrombus formation and hemolysis.3
Approach to LVAD patients in the ED
-Manage ABCs (airway, access, monitoring).
-Obtain patient’s blood pressure (either via doppler US or by placing arterial line) during initial assessment.
-Contact LVAD team coordinator (should be specific to your hospital, or patient should have phone number of coordinator).
-Auscultate for hum of LVAD and alarms. An alarm may indicate a battery problem. Check driveline and pump parameters. Perform bedside echo.
Assess for the following LVAD emergencies:
a) Arrhythmias
Most LVAD patients have underlying ischemic heart disease or other types of cardiomyopathy, so they are at increased risk for atrial and ventricular dysrhythmias.
The incidence of sustained VT/VF is ~52% in LVAD patients.4 If this is not corrected, the patient can go into RV failure and decompensate.
Emergent cardioversion is indicated if the patient is unstable (ie by BP measurement or has AMS but if stable, can discuss cardioversion further with LVAD team before proceeding).
b) Acute decompensated heart failure
Recurrent or persistent heart failure is a very common cardiac emergency in LVAD patients presenting to the ED, occurring in at least 20% of patients.5
This can occur due to RV or LV dysfunction or from general device failure.
| Causes of RV Failure |
| Primary myocardial dysfunction |
| Cardiac tamponade |
| Tricuspid regurgitation |
| Ventricular arrhythmias |
| Pulmonary hypertension |
| Pulmonary embolism |
| LVAD pump speed too high |
Suspect RV failure in patients with hypotension, peripheral edema, and JVD with echo findings of RV dilation, a D-shaped LV, and/or plethoric IVC.6
| Causes of LV Failure |
| Pump thrombosis |
| Cannula obstruction |
| Motor failure |
| Aortic insufficiency |
| Anemia due to GI bleed |
c) Bleeding
LVADs can cause acquired von Willebrand Disease, thought to be from the action of rotary or axial flow pump of the LVAD which causes high shear stress that may increase lysis of large vWF multimers.7 Patients are at a higher risk of GI bleeds and intracranial bleeds.8
d) Thrombosis
LVAD patients are also at risk for pump thrombosis and ischemic stroke, despite use of anticoagulation to minimize these complications.
The diagnosis of pump thrombosis can be suggested by hemolysis and changes in pump performance. Hemolysis may be suggested by hematuria, worsening renal function, and elevated LDH (> 1000). Patients with pump thrombosis may be asymptomatic or can present in severe heart failure.9
e) Infection
Can occur in pump, pump pocket, and around driveline, but driveline infections are the most common. Drainage from the skin exit site is suggestive of a driveline infection.
Patients may present with only localized skin infections or may be septic.
The most common bacteria causing infections include S. aureus and coagulase-negative staph, followed by gram-negative bacilli (Klebsiella, Pseudomonas).10
f) LVAD patient in extremis
What do you do if your LVAD patient isn’t awake or breathing? Since pulses likely will not be palpable, along with securing the patient’s airway, the next step is to listen over the heart for a whirring sound indicating that the pump is working. If there is no sound, look for a reason why the pump isn’t working (power supply, battery, cables). If the pump is okay, perform doppler US to determine MAP and echo to assess for tamponade, findings suggestive of PE, etc. Chest compressions are controversial in LVAD patients as they can theoretically dislodge the device, but may be considered on a case-by-case basis as a last resort.11
In summary, LVAD patients are a unique patient population that are at high risk for several specific types of emergencies (arrhythmias, heart failure, thrombosis, bleeding, and infection). Careful monitoring of these patients and coordination with their LVAD teams are important for their management in the ED.
Special thanks to Dr. Felipe Teran for his guidance on all things LVAD.
References / Further Reading
- Miller L, Guglin M: Patient selection for ventricular assist devices: a moving target. J Am Coll Cardiol 2013; 61(12): pp. 1209-21.
- Krishnamani R, DeNofrio D, Konstam M: Emerging ventricular assist devices for long-term cardiac support. Nat Review Cardiol 2010; 7(2): pp. 71-6.
- Morshuis M, El-Banayosy A, Arusoglu L, et al. European experience of DuraHeart magnetically levitated centrifugal left ventricular assist system. Eur J Cardiothoracic Surg 2009; 35(6): pp. 1020-7.
- Anderson M, Videbaek R, Boesgaard S et al. Incidence of ventricular arrhythmias in patients on long-term support with a continuous-flow assist device (HeartMate II). J Heart Lung Transplant 2009; 28(7): pp. 733-5.
- Burke M, Givertz M: Assessment and management of heart failure after left ventricular assist device implantation. Circulation 2014; 129(10): pp. 1161-6.
- Mitoff P, Beauchesne L, Dick AJ et al. Imaging the failing right ventricle. Curr Opin Cardiol 2012; 27(2): pp. 148-53.
- Uriel N, Pak SW, Jorde UP et al. Acquired Von Willebrand syndrome after continuous-flow mechanical device support contributes to a high prevalence of bleeding during long-term support and at the time of transplantation. J Am Coll Cardiol 2010; 56(15): pp. 1207-13.
- Wilson TJ, Stetler WR Jr, Al-Holou WN et al. Management of intracranial hemorrhage in patients with left ventricular assist devices. J Neurosurg 2013; 118(5): pp. 1063-8.
- Goldstein DJ, John R, Salerno C et al. Algorithm for the diagnosis and management of suspected pump thrombus. J Heart Lung Transplant 2013; 32(7): pp. 667-70.
- Gordon RJ, Weinberg AD, Pagani FD et al. Prospective, multicenter study of ventricular assist device infections. Circulation 2013; 127(6): pp. 691-702.
- http://emcrit.org/wee/left-ventricular-assist-devices-lvads-2/
- http://www.ncbi.nlm.nih.gov/pubmed/25441039





5 thoughts on “LVAD Patients: What You Need to Know”
Pingback: LVADs | First10EM
Pingback: What Is A Lvad Patient – jumpask.com
Pingback: Mechanical Heart: a basic approach to LVADs in the ED - CanadiEM
Pingback: LVAD Management in the ED – Found Down
Pingback: LVAD = Tight Sphincter – JournalFeed