
Author: Christina Smith, MD (EM Resident Physician, UTSW/Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
Case Presentation
A 62 year-old male with PMH significant for CAD, CHF, COPD, ESRD, and prior PE presents with worsening shortness of breath since this morning. He called EMS after he noticed he was experiencing difficulty catching his breath. He is on several medications that he cannot remember, but one “blood thinner” and “some sort of puffer.” He also receives hemodialysis three times a week, and he states he has been compliant.
On first appearance, he is diaphoretic in a hunched over position trying his best to breath. His vital signs include: HR 121, BP 190/107, RR 25, Temp 38, and O2 Saturation 94% on room air.
An ECG is obtained and shows no change compared to prior: sinus rhythm with tachycardia to 120 and no ST or T wave abnormalities. CXR shows mild bilateral pulmonary edema. BNP is mildly elevated to 1,200 (baseline on prior labs 500). Troponin is 0.05 (baseline on prior labs is 0.03).
The differential for dyspnea and his laboratory findings is extensive, and this patient could have numerous confounders contributing to his elevated troponin. But first, what is troponin, and what does an elevation mean?
Background
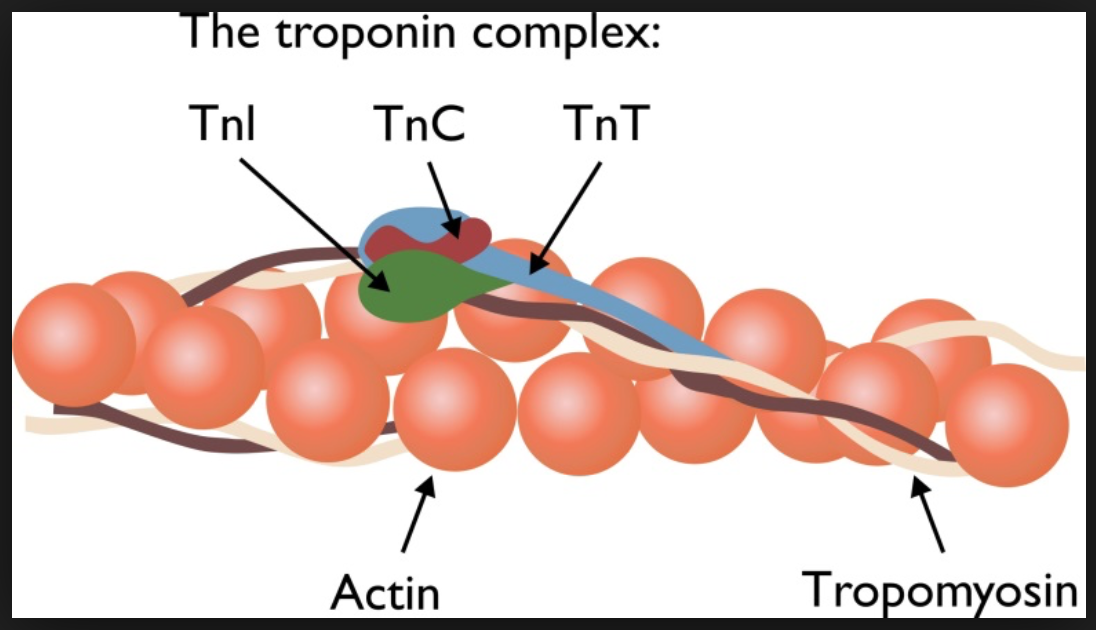
Cardiac troponins consist of three proteins: cTnC, cTnI, and cTnT1. These proteins interact with tropomyosin to form a complex that functions as the backbone of striated muscle. This functions in the excitation and contraction coupling of the heart through modulation of actin-myosin interaction in muscle.
How do these types of troponin differ? Cardiac troponin I is specific for cardiac tissue, as it is not expressed in injured or regenerating skeletal muscle elsewhere. cTnT and cTNI are comparable for use in cardiac ischemia, but cTnT is more likely to be elevated with renal failure.
Troponin elevation can occur immediately after cardiac injury, but labs may only pick it up after one hour of injury. Peak level is reached at 24 hours, and troponin will often stay positive for one week.
What about other causes of troponin elevation? Did CKD, COPD exacerbation, sepsis, pericarditis, aortic dissection, even pulmonary embolism cross your mind as a possibility for his elevated troponin, or did tunnel vision of ACS take over? Not every troponin elevation is due to ACS, and we must understand the pitfalls of troponin, causes of elevation, and appropriate uses of troponin to broaden our differential.(1) Sample causes of elevated troponin are shown in table 1.
Table 1 – Causes of Elevated Troponin
| Noncardiac Causes | Cardiac Causes |
| Acute Noncardiac Critical Illness | Acute and Chronic Heart Failure |
| Acute Pulmonary Edema | Acute Inflammatory Myocarditis or Endocarditis/Pericarditis |
| Acute Pulmonary Embolism | Aortic Dissection |
| Cardiotoxic Drugs | Aortic Valve Disease |
| Stroke, Subarachnoid hemorrhage | Apical Ballooning Syndrome |
| Chronic Obstructive Pulmonary Disease | Bradyarrhythmia, Heart Block |
| Chronic renal failure | Cardiac contusion from trauma |
| Extensive Burns | Cardiac surgery, Post-percutaneous Coronary Intervention, Endomyocardial biopsy |
| Infiltrative Disease (Amyloidosis) | Cardioversion |
| Rhabdomyolysis with Myocyte Necrosis | Direct Myocardial Trauma |
| Sepsis | Hypertrophic Cardiomyopathy |
| Severe Pulmonary Hypertension | Tachycardia/Tachyarrhythmia, Bradyarrhythmia |
| Strenuous Exercise/Extreme Exertion |
Noncardiac Causes
Acute Noncardiac Critical Illness(2,3,4,5)
Patients in the intensive care unit are by definition critically ill. These patients may be ventilated, on inotropic support, have a high core temperature, tachycardic, hyper- or hypotensive, and most likely are not healthy at baseline. All of this increased myocardial demand leads to a pathologic process. And in result, troponin elevation can be seen with increased cardiac demand (type II NSTEMI) and unfortunately is associated with higher morbidity and mortality rates.
Pitfall: Do not conclude that patients with noncardiac critical illness and elevated troponin without other manifestations of ACS have AMI. ECG and history are vital.
Pearl: Troponin elevation in the critically ill has a correlation with mortality and morbidity. However, utilization of ECG and history are important in differentiating demand ischemia and another cardiac event.
Acute Pulmonary Embolism (PE) (2,3,6)
Cardiac troponin elevation can occur anywhere from 10-50% of pulmonary embolism patients and can signify the degree of myocardial injury likely from right heart strain, hypoxia, release of endothelial mediators, and decreased coronary blood flow. Increase in troponin correlates with increased morbidity and mortality in patients with acute PE.
Pitfall: Do not conclude in a patient with positive troponin that they have an NSTEMI without considering the diagnosis of PE. Strongly consider patient risk factors and your history and exam. If suspicious of PE, use a clinical scoring system to risk stratify the patient and consider imaging.
Pearl: Troponin elevation in setting of PE signifies a worse clinical picture. These patients with PE and elevated troponin likely warrant admission for close monitoring and treatment.
Stroke and Subarachnoid hemorrhage (SAH) (2,3,7)
In patients with intracranial bleeding, catecholamine release, either in plasma concentration or stimulated specifically in cardiac nerves, causes “contraction band necrosis” in the myocardium. This necrosis of cardiac cells releases troponin. It has also been suggested that the higher level of troponin elevation in subarachnoid hemorrhage suggests a higher severity of injury and a poorer prognosis. However, in patients with ischemic strokes, there are not as strong of studies to correlate with prognosis.
Pitfall: When you see an elevated troponin result, do not forget to consider stroke or SAH as the cause in the right clinical setting.
Pearl: Remember the catecholamine hypothesis. Sudden neurologic deficit or headache that points to stroke or SAH are key.
Chronic Obstructive Pulmonary Disease (COPD)( 3,8,9)
Myocardial damage occurs during a COPD exacerbation secondary to increased left ventricular afterload, increased RV demand, pulmonary hypertension, hypercapnia, and hypoxia that puts more demands on energy needs from the body. Elevated troponin in this setting has actually been proven to be a strong independent predictor of mortality in those admitted and following discharge. It is also a predictor of increased need for noninvasive mechanical ventilation. Unfortunately, these patients often have other comorbidities that predispose them to ACS.
Pitfall: Do not fall into the trap that an elevated troponin in a COPD flare is of no significance. These patients must be monitored closely for decompensation.
Pearl: Elevated troponin in COPD is predictive of mortality and need of further intervention such as noninvasive ventilation. Carefully evaluate these patients for chest pain as well, and look closely at the ECG for other signs of ischemia.
Chronic renal failure(2,3,6)
There are many possibilities as to why the troponin is elevated in this patient population including decreased clearance of normal cardiac myocyte loss, heart failure without evidence of ischemia or infarct, chronic inflammation or damage to skeletal muscle, or a combination of them all. So how are we supposed to approach this clinically?
Providers must consider the entire picture of the patient from their presenting symptoms to their ECG and labs with comparison to prior if available.
It is thought that cardiac troponin I holds advantages over troponin T because it is cleared more by dialysis and undergoes more chemical conversions in serum due to its instability. Troponin I should be less elevated than troponin T in the setting of chronic renal failure.
Pitfall: Do not make a clinical decision on troponin alone in a CKD patient. Scrutinize the ECG and take a careful history. Look at baseline labs if possible.
Pearl: Troponin can be elevated in patients with CKD in the absence of acute coronary syndrome, especially troponin T. There is not an easy solution to this conundrum. ECG and lab results cannot be trusted and therefore you have to keep your clinical suspicion high. Carefully evaluate the clinical picture with history, exam, and ECG.
Sepsis(2,6)
Sepsis results in an inflammatory response, releasing mediators that depress the myocardium. Myocardial depression may lead to increased membrane permeability, resulting in troponin leak. Fortunately, this damage is usually not due to necrosis and is reversible. In other instances, a troponin increase can result from increased oxygen demand on the myocardium in the setting of reduced oxygen supply that does in fact lead to myocardial injury. Overall, increased troponin in the setting of sepsis is associated with increased morbidity and mortality.
Pitfall: Do not conclude that a positive troponin is ACS in the setting of sepsis.
Pearl: Troponin leak in the setting of sepsis is associated with increased morbidity and mortality.
Cardiac Causes
Acute and Chronic Heart Failure(3,6,10)
Troponins may be elevated in acute or chronic heart failure patients in the absence of ischemia. Previous studies have suggested that chronically damaged myocardium leaks proteins, specifically muscle contraction proteins, when subjected to further stress. Other injuries to the myocardium including global wall stretch, coronary malperfusion, or hypoxemia are also responsible for troponin elevation. Although it might not be useful to determine if this patient is having ACS, high sensitivity troponin I can be useful to determine the mortality rate.
Pitfall: Do not fall into the trap of thinking an elevated troponin means an acute ischemic event in a heart failure patient.
Pearl: Troponin elevation in chronic heart failure is still significant, as there is likely myocardium protein damage, but it does not always mean ACS. If possible, compare to an old troponin level and evaluate for change. A significant change from baseline may be true ACS. Evaluate the ECG for changes from a baseline ECG.
Aortic Dissection(2,3,11)
The reason as to why troponin is elevated in aortic dissection is not fully understood, although coronary compromise and increased demand have been proposed as the most likely causes. And as one may predict, aortic dissection is frequently misdiagnosed as ACS. This has dangerous consequences including delay in diagnosis or treating for ACS with antithrombotic agents that cause increased bleeding in an aortic dissection patient. Studies have shown elevated troponin associated with type A aortic dissection, signifying myocardial loss, may indicate hemodynamic compromise.
Pitfall: Do not forget to consider aortic dissection in patients presenting with ACS-type signs and symptoms.
Pearl: Always consider aortic dissection as a possible cause of elevated troponin. Ask patients about pain that is sudden in onset, ripping/sharp/tearing pain, pain that moves or changes, chest pain with neurologic symptoms, or pain above and below the diaphragm.
Acute Inflammatory Pericarditis, Myocarditis, or Endocarditis(2,3,6)
Myocarditis closely resembles ACS, not just clinically but pathologically with necrosis being the cause of troponin elevation in both. Troponin elevation can correlate with heart failure one month after primary infection, as well as inflammation severity based on continued elevation.
Pericarditis also can resemble ACS, but normally there is a history of a recent viral illness. Troponins are found in the myocardium, but are not found in the pericardium. However, you can still see a troponin elevation if the epicardium, or even if the myocardium, is involved in the inflammatory process of pericarditis. Troponin elevation in this instance however does not correlate with poor prognosis.
In patients with endocarditis, troponin elevation does correlate with morbidity and mortality.
Pitfall: Do not conclude in a patient with positive troponin that they have an NSTEMI without considering diagnosis of endocarditis, pericarditis, and myocarditis.
Pearl: ACS can be seen simultaneously in patients with endocarditis, pericarditis, or myocarditis.
Conclusion
A troponin elevation does not mean it’s ACS. At the end of the day, troponin is a tool and nothing more. Physicians must take into account the entire clinical picture: history, exam, ECG, baseline labs, response to treatment, clinical gestalt, etc. Several studies have suggested that in ACS, the initial troponin I on average is higher than elevations in non-ACS cases, with a median troponin of 0.14 ng/mL.(12) This can be just another tool to decipher the diagnosis causing an elevated troponin in our patients.
However, the critical step is to realize that not every elevated troponin is cardiac in nature. We must be wary of tunnel vision and broaden our differential because if we don’t, we risk missing high morbidity/mortality entities.
References/Further Reading
[1] Mahajan, V. S., and P. Jarolim. “How to Interpret Elevated Cardiac Troponin Levels.” Circulation 124.21 (2011): 2350-354. Web.
[2] Kelley, W. E., J. L. Januzzi, and R. H. Christenson. “Increases of Cardiac Troponin in Conditions Other than Acute Coronary Syndrome and Heart Failure.” Clinical Chemistry 55.12 (2009): 2098-112. Web.
[3] Tanindi, Asli, and Cemri. “Troponin Elevation in Conditions Other than Acute Coronary Syndromes.” VHRM Vascular Health and Risk Management (2011): 597. Web.
[4] Koshkina, EV, MIa Krasnosel’skiĭ, NM Fedorovskiĭ, EV Goriacheva, AA Polupan, AA Aref’ev, and AG Katrukha. “Diagnostic Value of Cardiac Troponin T Increase in Critically Ill Patients.” Anesteziol Reanimatol 6 (2009): 42-46. Print.
[5] Guest, Thomas M. “Myocardial Injury in Critically Ill Patients.” Jama 273.24 (1995): 1945. Web.
[6] Korff, S. “Differential Diagnosis of Elevated Troponins.” Heart 92.7 (2006): 987-93. Web.
[7] Miketic, J. K., M. Hravnak, S. M. Sereika, and E. A. Crago. “Elevated Cardiac Troponin I and Functional Recovery and Disability in Patients After Aneurysmal Subarachnoid Hemorrhage.” American Journal of Critical Care 19.6 (2010): 522-28. Web.
[8] Fruchter, Oren, and Mordechai Yigla. “Cardiac Troponin-I Predicts Long-Term Mortality in Chronic Obstructive Pulmonary Disease.” COPD: Journal of Chronic Obstructive Pulmonary Disease 6.3 (2009): 155-61. Web.
[9] Baillard, C., M. Boussarsar, JP Fosse, E. Girou, P. Le Toumelin, C. Cracco, and S. Jaber. “Cardiac Troponin I in Patients with Severe Exacerbation of Chronic Obstructive Pulmonary Disease.” Intensive Care Med 29.4 (2003): 584-89. Print.
[10] Missov, E., C. Calzolari, and B. Pau. “Circulating Cardiac Troponin I in Severe Congestive Heart Failure.” Circulation 96.9 (1997): 2953-958. Web.
[11] Bonnefoy, Eric, Patrick Godon, Gilbert Kikorian, Sylvie Chabaud, and Paul Touboul. “Significance of Serum Troponin I Elevation in Patients with Acute Aortic Dissection of the Ascending Aorta.” Acta Cardiologica 60.2 (2005): 165-70. Web.
[12] Harvell, Bryan, Nathan Henrie, Amy A. Ernst, Steven J. Weiss, Scott Oglesbee, Dusadee Sarangarm, and Lorenzo Hernandez. “The Meaning of Elevated Troponin I Levels: Not Always Acute Coronary Syndromes.” The American Journal of Emergency Medicine (2015): n. pag. Web.





3 thoughts on “The Elevated Troponin: What else besides ACS could cause troponin elevation?”
A cardiologist once condescendingly asked an intern at my hospital whether they’d excluded sarcoidosis as a cause of elevated troponin. Context is everything when it comes to troponin levels!
Pingback: Länkar v6 | Internmedicin
A few more for your list (much less common to very rare):
Kounis syndrome
Takotsubo syndrome
Coronary artery anomalies
Spontaneous coronary artery dissection
Noncardiac:
heterophile antibodies interference with the troponin immuno-assay can cause elevated trop
conversely supra-pharmacologic po intake of biotin supplements can produce falsely low troponin