
Authors: Kelsey Martin, MD, Jeffrey Uribe, MD (Lincoln Medical Center Bronx New York), Muhammad Waseem, MD, MS (Lincoln Medical Center & St. Georges University Grenada West Indies), Joel Gernsheimer, MD (SUNY Downstate Medical Center, New York) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case 1
A 65-year-old male presents with sudden weakness and pain in the left leg. He denies trauma. He states that this weakness began suddenly two hours ago, but he was able to ambulate normally without any assistance earlier this morning before his symptoms began. He is now unable to ambulate, which brought him to the ED. What is the most likely cause of his inability to walk?
Introduction
A patient may be unable to walk for many reasons. The patient may not be able to walk because of severe pain in an extremity that may be due to a fracture or dislocation or other muscle-skeletal problem, or because of weakness. Weakness is a common complaint in the ED, and a most challenging one. The first priority with a patient presenting with acute weakness should be to evaluate and stabilize, if necessary, the patient’s airway, breathing, and circulation. Even if initially the patient appears to be stable, the patient’s underlying etiology of the acute weakness may cause the weakness to be progressive and eventually interfere with the patient’s airway and/or breathing. Therefore, the ABCs of these patients must be closely monitored, reevaluated, and stabilized as necessary.
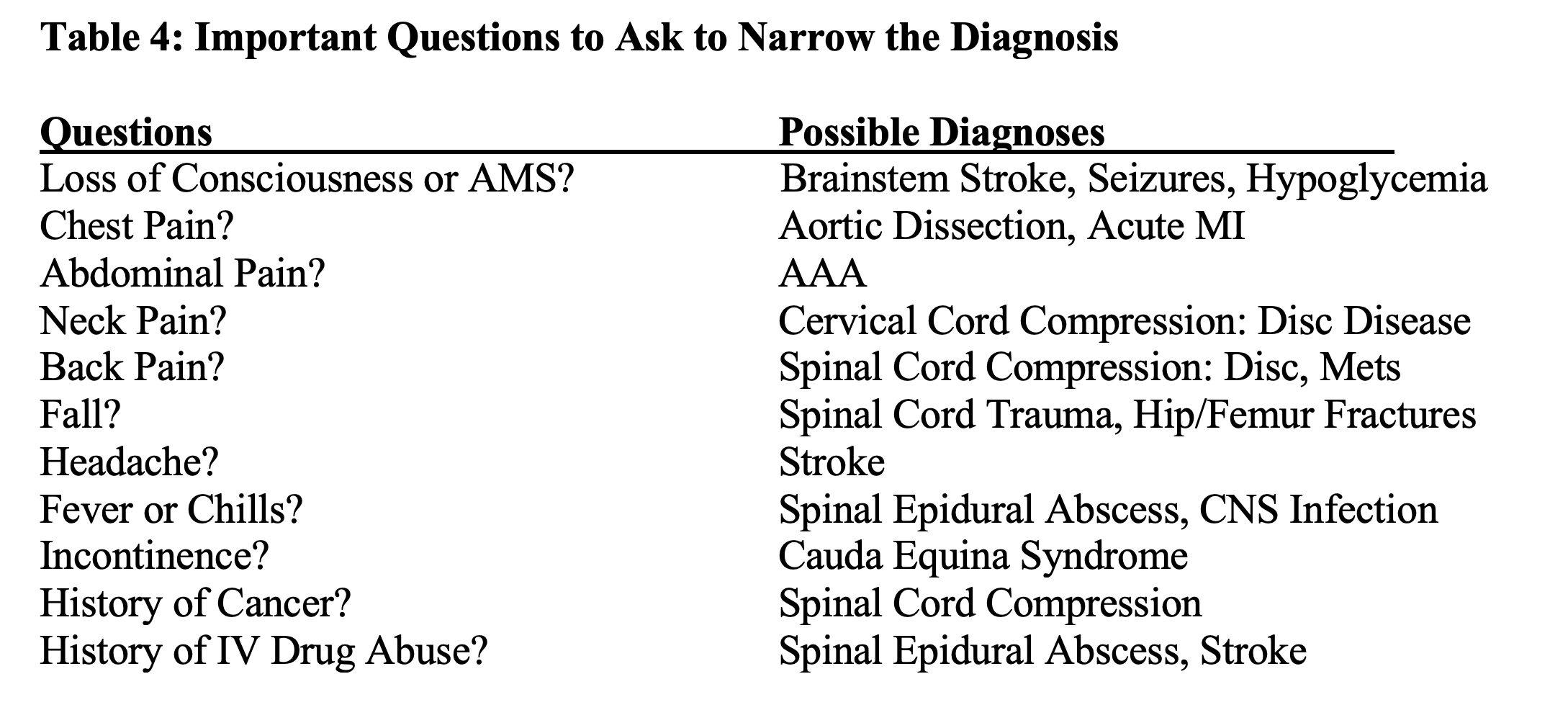
Once the patient is stabilized, an accurate and thorough history of the present illness is needed (1). If the patient states that the main problem is weakness, what does the patient mean by weakness? The patient may have fatigue or generalized weakness that may be due to a systemic illness, including metabolic, infectious, endocrine, toxic, and cardiac causes. On the other hand, weakness may affect specific sites: one lower extremity, both lower extremities, bilateral weakness from the neck down, or weakness on one half of the body. Etiologies that may cause these types of weakness can be neurologic, traumatic, infectious, or vascular. Obtaining a good time line for the weakness is helpful in making the diagnosis. The patient may have a chronic problem, such as diabetic neuropathy, and even though symptoms have been progressing for some time, patients may not seek care until they are unable to ambulate. The onset of acute weakness may provide a valuable clue for making the diagnosis. Generally, weakness that develops minutes to hours prior to presentation is due to metabolic disorders, for example hypoglycemia, disorders of electrolytes, such as hypo and hyperkalemia, toxic disorders, such as organophosphate poisoning, acute severe trauma, such as a cervical spine injury, or vascular disorders, such as a stroke. Rapid onset of weakness over minutes strongly suggests a vascular pathology.Weakness that began within the last 24 hours, include etiologies such as Guillain-Barre syndrome (GBS), myasthenia gravis, botulism, and tick paralysis.An onset of weakness over hours or days is more indicative of an infection, such as an epidural abscess or an inflammatory condition, such as myelitis (2,3).
The history should also include associated symptoms such as fever, pain, trauma, numbness, and possible risk factors. A detailed physical exam, with neurologic assessment, is needed. If possible, closely observing the patient’s gait as part of the neurologic exam may help pinpoint where the problem is. The patient must be stable and strong enough to stand, and precautions must be taken to keep the patient from falling. A good exam will usually help distinguish if the difficulty walking is mainly from pain or weakness or both. If the difficulty walking appears to be mainly from pain, giving the patient analgesia and then reexamining the patient may help decide if the problem ambulating was probably due to pain or was weakness also present.
Further workup, including lab tests and imaging should be based on the history and physical exam and suspected conditions.
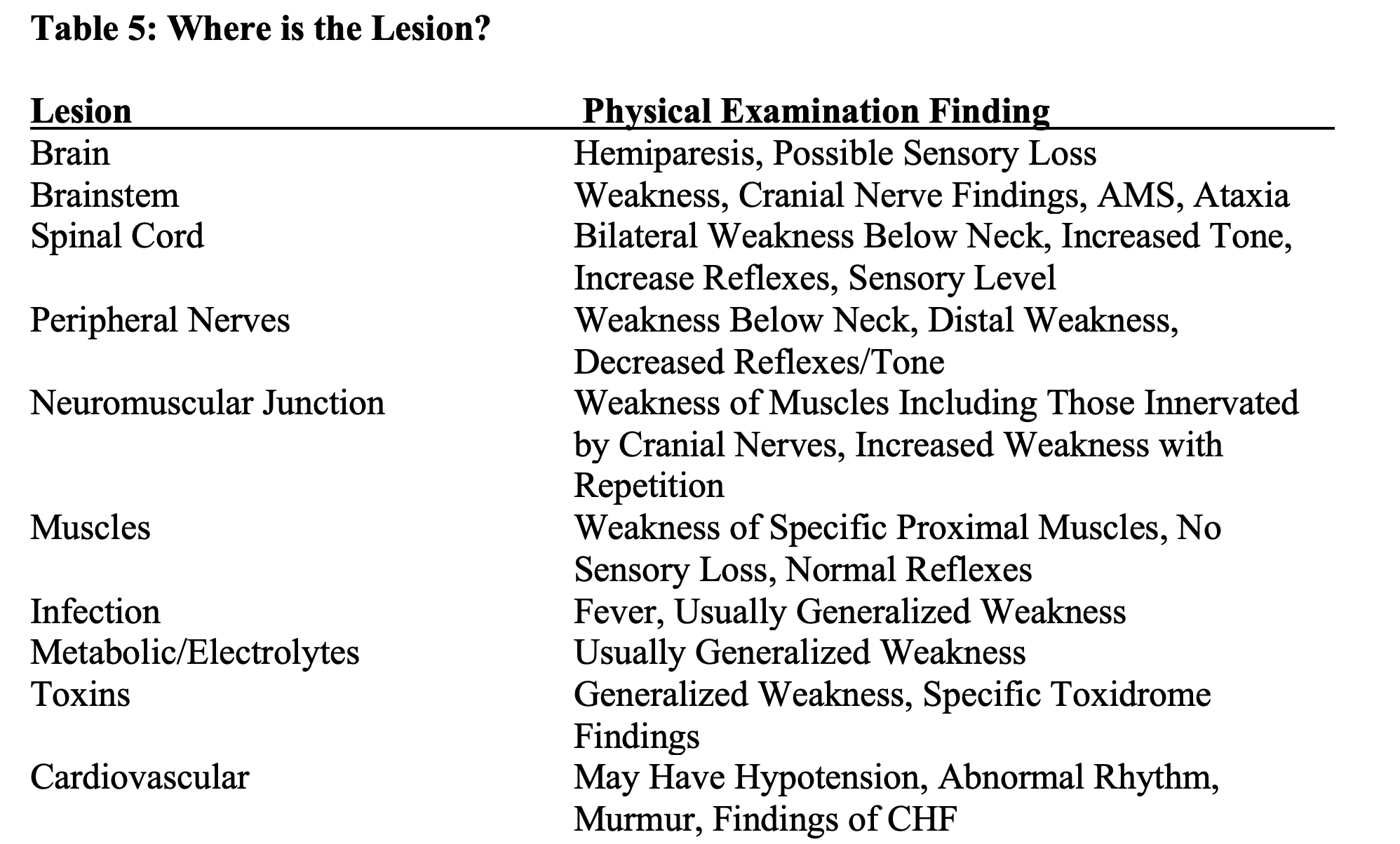
Attention should first be directed towards life-threatening and then serious causes. These disabilities can be caused by lesions in any of the following areas of the nervous system: brain, spinal cord, peripheral nerves, the neuromuscular junction (NMJ), or muscles (4).

Differentiating upper motor neuron lesions from lower motor neuron lesions depends on examination (2). The muscles of the upper face are innervated by motor neurons that receive bilateral projections from the motor cortex, whereas the motor neurons that innervate the muscles of the lower face receive projections only from the contralateral motor cortex. Upper motor neuron lesions present with an ipsilateral lower facial paralysis only, whereas upper facial function is preserved, and the patient will be able to wrinkle his forehead on the affected side. Peripheral lesions of the facial nerve, such as Bell’s palsy, will affect the whole side of the face including the forehead, and the patient will be unable to wrinkle his forehead on the affected side.
If the lesion involves the CNS pathways, the lower motor neurons are under the uninhibited influence of the spinal reflex. The motor units have an exaggerated response and present with increased tone (spasticity), clonus, and brisk reflexes. There is weakness, but usually not wasting. Primitive reflexes, such as the plantar extensor response (Babinski’s sign), may be present. A lower motor neuron lesion causes weakness and wasting of muscle fibers, reduced tone (flaccidity), fasciculation, and reduced or absent reflexes (4). One notable exception to the above is acute “Spinal Shock” due to acute cervical spine trauma. In this condition, the patient initially may have an acute flaccid paralysis from the neck down, but eventually the patient will develop a spastic paralysis (5).

Case 1 Continued:
When this patient was further evaluated, it was noted that he had weakness of his left leg and left arm, and drooping of the right side of his face. A “Stroke Code” was called, and he was taken to the CT scanner. The CT scan was normal, and because he was still in the “three-hour window” for treatment with fibrinolytic therapy due to the prompt evaluation by the ED staff, he was given TPA. He was subsequently admitted to the “Stroke Unit”, where he did very well. This case illustrates the importance of prompt and proper evaluation of patients who present with acute weakness.
Case 2
A 60-year-old male presents with lower extremity weakness after a fall during a shower. After this event, he was unable to stand and crawled to his room.
It is very important to ask why the patient fell, especially in the case of elderly patients. Did the patient have a mechanical fall from slipping or tripping? Did the patient fall because he had a syncopal or pre-syncopal episode? Did he suddenly become weak and then fell? It must be determined what came first. Did the patient have a mechanical fall that caused trauma to his head, spine, or extremities that led to the weakness, or did sudden neuromuscular weakness from a major neurologic, cardiovascular, or metabolic event cause his fall?
Once the patient’s airway, breathing and circulation are evaluated and stabilized as necessary, it is very important to get a history as to why he fell. In this case, the patient stated that he fell because he suddenly became weak in both legs.
This presentation could be due to many neurologic conditions such as stroke, intracranial hemorrhage, spinal cord involvement or peripheral nerve diseases. Metabolic conditions, such as hypokalemic periodic paralysis and hypoglycemia, should also be considered (4).

The history and physical exam, including a good neurologic exam, will help you focus in on your top differentials.
Finding out the etiology is a necessary starting point.
Laboratory testing should be based on the history and physical exam findings. Tests that are usually done are a complete blood count, a chemistry profile that should include serum glucose, electrolytes, renal and liver function tests, and a coagulation profile. Other tests that may be included depending on the patient’s presentation are an electrocardiogram, cardiac enzymes, muscle enzymes, cultures, arterial blood gases and blood for type and screen.

Case 2 Conclusion
Further questioning of our patient revealed that he had had sudden severe chest pain that radiated to his back, and that he had had sudden weakness and numbness of his legs that caused him to fall. Although he was usually hypertensive, his BP now was 110/80 with a tachycardia of 110 beats/minute. He had bilateral loss of sensation or motor function below the knees. His upper extremity pulses were 2+ bilaterally, his femoral pulses were 1+ bilaterally, and no dorsalis pedis or posterior tibial pulses were noted by palpation or with Doppler ultrasound. His FAST Exam showed a possible pericardial effusion. CTA of the patient’s chest, abdomen, and pelvis showed a large Type A aortic dissection with a hemopericardium. The patient was immediately taken to the OR and survived, because the ED physician strongly suspected this life-threatening diagnosis from the history and physical examination and acted expeditiously.
Case 3
A 3-year-old boy is brought to the ED by his grandmother because he had difficulty walking. His grandmother reported that he had been complaining of leg pain for almost one week. Today he told her that he could not walk, and when she insisted that he try to walk, she noted that he had a clumsy gait. This is the child’s first visit to your hospital.

Differential diagnosis of pain causing difficulty walking:
Infection/infection-related:
Septic Arthritis
Osteomyelitis
Lyme disease
Toxic synovitis
Rheumatic fever
Trauma/Overuse:
Fracture
Soft-tissue injury
Osgood-Schlatter disease
Hypermobility
Malignancy:
Leukemia
Neuroblastoma
Bone Tumors
Hematologic:
Hemophilia
Sickle cell anemia
Inflammatory:
Juvenile idiopathic arthritis
Systemic lupus erythematous
Henoch Schonlein purpura
Reactive arthritis
Orthopedic/Mechanical:
Slipped capital femoral epiphysis
Legg-Calve-Perthes disease
Miscellaneous/Non-inflammatory:
Fibromyalgia
Reflex sympathetic dystrophy
Conversion reaction
A good history of the difficulty in walking in the time period leading up to the emergency department presentation may give you valuable clues that will help you in making the diagnosis, especially if the child was limping.
A good mnemonic for a child limping is: STOP LIMPING (6)
S: Septic arthritis
T: Toddler’s fracture (1-3 years, due to a minor fall with a rotational component)
O: Osteomyelitis (2% of those children presenting with limp)
P: Legg-Calve-Perthes disease
L: Limp length discrepancy
I: Inflammatory (transient synovitis)
M: Malignancy
P: Pyomyositis
I: Iliopsoas abscess
N: Neurologic/ stroke
G: Gastrointestinal /genitourinary
The history and physical exam, including an appropriately thorough orthopedic and neurologic examination, will help you make the correct diagnosis.
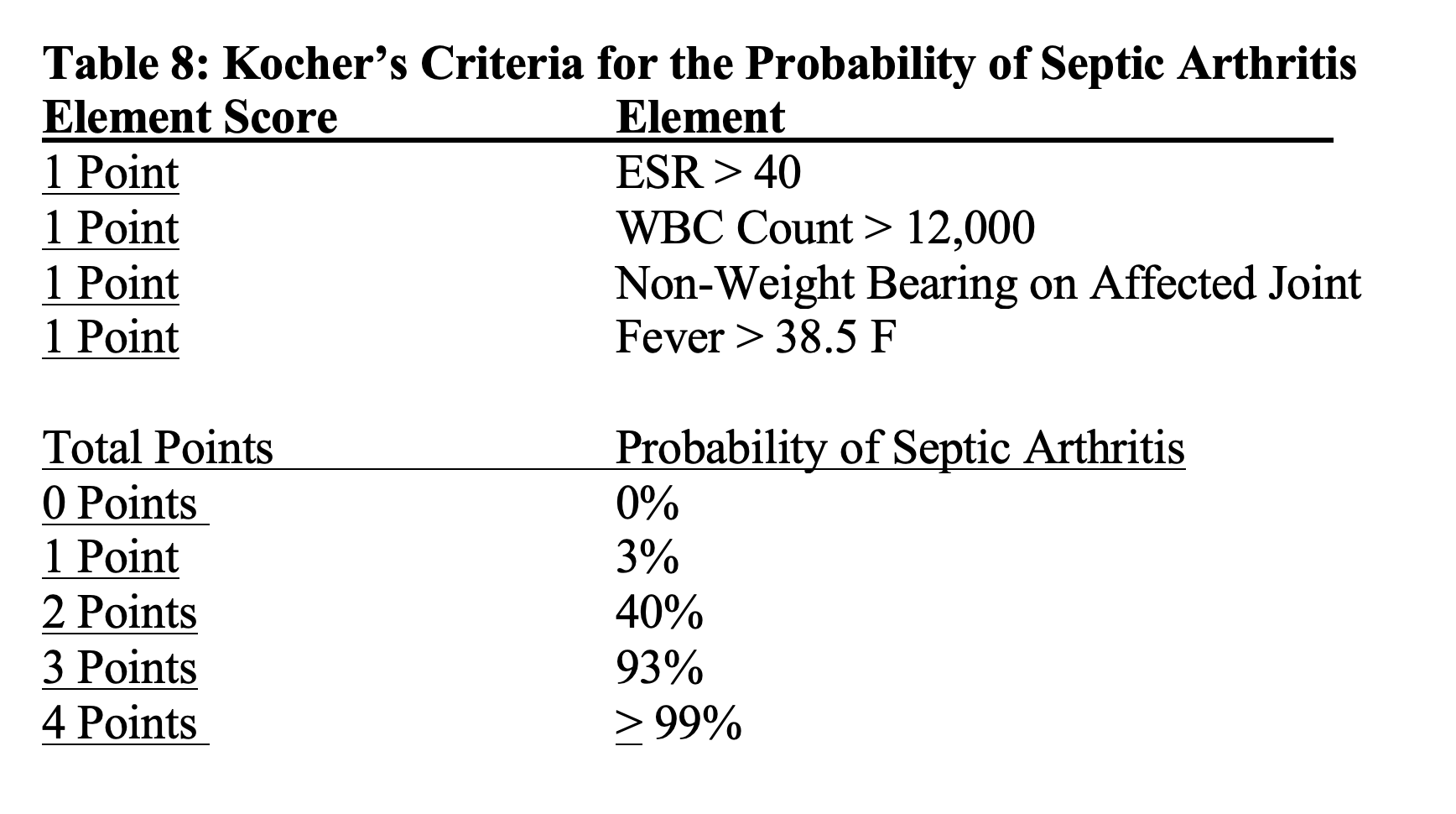
A common criterion used to determine the probability of whether the pediatric patient has septic arthritis is Kocher’s criteria (7). It is crucial not to miss the diagnosis of septic arthritis, is this infection can destroy the involved joint rapidly if not appropriately treated.
Appropriate imaging is important when evaluating the limping child and may include x-rays and ultrasounds of the involved joints. An MRI may be needed to confirm the suspected diagnosis. Laboratory tests can include CBC, ESR, and CRP if an infectious or hematologic/oncologic etiology is a possible cause, and Lyme titers should be sent if the patient is from an endemic area (8, 9).
Case 3 continued: More history is obtained from the patient’s grandmother, and she reveals that very recently he has been dropping objects from his hands. She also states that he had a prior ED visit because of fever, vomiting and diarrhea 2 weeks ago, which resolved after 4 days.
The physical examination of the child is remarkable for bilateral weakness of the patient’s legs and hands. The ED physician is unable to elicit the patient’s ankle or knee reflexes in either leg. An evaluation of the patient’s respiratory function in the ED is normal. A presumptive diagnosis of Guillain-Barre Syndrome is made, and the patient is admitted to the Pediatric ICU for close monitoring of his pulmonary status. A lumbar puncture is performed, and his CSF demonstrated a normal WBC count, but his CSF protein is elevated, which further confirmed the diagnosis of Guillain-Barre Syndrome. The patient is treated with IVIG therapy and did very well, because of the correct and prompt diagnosis of this potentially fatal disease by the ED staff.
The combination of rapidly progressive difficulty in walking, pain, weakness and areflexia indicates an acute peripheral neuropathy. Guillain-Barre syndrome (GBS) is the most likely cause of this clinical presentation. (The physical finding of decreased or absent reflexes in a patient with acute weakness is an important neurologic finding that should strongly suggest this diagnosis to the examining clinician. The diagnosis also requires progressive ascending motor weakness. Leg pain is also a common complaint in children. Ataxia, due to difficulty with proprioception, is also common. GBS is an immune mediated neuropathy, which often follows an upper respiratory tract infection or gastrointestinal infection (10). Campylobacter jejuni infection is one of the most common precursory etiologies.
CSF studies are essential for confirming the diagnosis. It usually reveals albumin-cytologic dissociation, which is an increased protein level, without an increase in WBC counts. Usually, CSF protein is elevated to more than twice the upper limit of normal.

Key Points:
- “I can’t walk” is an important complaint that has many etiologies, including neurologic, orthopedic, and metabolic.
- Determining what the patient means by inability to walk is essential (ie, pain vs. weakness vs. focal deficit).
- While evaluating the patient for the cause of weakness with a good history, physical exam, and appropriate ancillary testing, it is critical to evaluate and stabilize the patient’s ABCs.
- Determining which part of the nervous system is involved will help make an expeditious and correct diagnosis that will lead to appropriate therapy, which may prevent further mortality and morbidity.
References/Further Reading
1) Swenson, Rand. “Evaluation of Patient with Weakness.” In Reeves & Swinton: Disorders of the Nervous System. Dartmouth Medical School. Available online: https://www.dartmouth.edu/~dons/part_2/chapter_12.html.
2) Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006;355(19):2012-2020.
3)Frohman EM and Wingerchuck DM. Transverse Myelitis. N Engl J Med 2010; 363:564-572.
4) Ganti L, Rastogi V. Acute Generalized Weakness.Emerg Med Clin North Am. 2016 Nov;34(4):795-809
3) Anderson RS and Hallen SAM. Generalized weakness in the geriatric emergency department patient. Clinics in Geriatric Medicine 2013, 29(1):91-100.
4) Weidauer S et al. Spinal cord ischemia: aetiology, clinical syndromes and imaging features. Neuroradiology 2015, 57(3):241-257.
5) Molliqaj G et al. Acute traumatic central cord syndrome: comprehensive review. Neurochirurgie 2014, 60(1):5-11
6) http://pemplaybook.org/podcast/please-just-stop-limping/
7) Kocher MS, Mandiga R, Zurakowski D, Barnewolt C, Kasser JR. Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children.J Bone Joint Surg Am. 2004 Aug;86-A(8):1629-35.
8) Edlow JA and McGillicuddy DC. Tick paralysis. Infectious Disease Clinics of North America 2008, 22(3):397-413.
9) Grattan-Smith PJ et al. Clinical and neurophysiological features of tick bite paralysis. Brain 1997, 120, 1975–1987.
10) Winer JB. Clinical Review: Guillain-Barre syndrome. BMJ 2008;337:a671





1 thought on “The Patient Acutely Can’t Walk: Pearls and Pitfalls”
Pingback: Länkar v20-23 | Internmedicin