
Author: Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Your first patient of the day is a 33-year-old female who presents with decreased vision in the right eye with eye pain that she describes as a deep, boring sensation. This pain has been gradually worsening over three days and is associated with photophobia and what she describes as “red doesn’t look like the normal red.”
Your next patient is a 62-year-old male who presents with two hours of sudden vision loss in the left eye. He states that over the past two weeks he has experienced bright lights and dark spots in the periphery of his vision, which sound like flashes and floaters to you. He has not had any pain, and there is no trauma with his symptoms. He has a history of severe near-sightedness and hypertension.
The final patient is a 57-year-old female with decreased vision in the right eye over one day with right-sided headache that worsens with chewing. In fact, she has been unable to chew her food properly due to the pain and fatigue she experiences with chewing. She has felt more tired than usual and has experienced unintentional weight loss over the past month.

These three patients have one item in common: acute decrease in vision. Ophthalmologic complaints are common in the ED, but many physicians are not comfortable with the evaluation and management of these conditions. This post seeks to provide an overview of the evaluation of vision loss in the ED and a summary of several common conditions.
Acute vision loss can have many etiologies with a large differential. Many of these are time-sensitive, and the emergency physician may improve patient outcome through the consideration of several acute conditions.
Definitions:
Acute visual loss is defined by visual deficit lasting less than 24 hours upon evaluation. Persistent visual loss is dysfunction lasting greater than 24 hours.1-3
To best evaluate vision loss and the multitude of causes, providers must understand the visual pathway. Three major anatomic areas including the media, retina, and neural pathways may be affected, resulting in visual deficits.
– Media: These include keratopathy, vitreous hemorrhage, uveitis, endophthalmitis, hyphema, and lens pathology.
– Retina: These include retinal detachment, vascular occlusion, and acute maculopathy.
– Neural Pathway: Malfunction in this category may occur at the optic nerve, optic chiasm, and retrochiasm, including posterior occipital lobe.
A second, and more common, means of differentiation include painful and painless sudden loss of vision.
– Painful includes acute glaucoma, optic neuritis, giant cell arteritis (GCA), uveitis, and migraine headache.
– Painless includes central retinal artery occlusion (CRAO), central retinal vein occlusion (CRVO), ischemic optic neuropathy, cataract, vitreous hemorrhage, amaurosis fugax, TIA, cortical blindness, retinal detachment, macular degeneration, diabetic retinopathy, CMV retinitis, methanol intoxication, and functional visual loss.
Before we explore this large differential diagnosis, a systematic approach should be followed with history and physical examination. Similar to many conditions managed in emergency medicine, the history and physical examination often will lead to the diagnosis.
Pearl 1: Know the history you need to obtain.
History: Several aspects of the history are important. First, a distinction should be made on whether the visual loss was acute, or if preexisting visual deficit was present before the onset of worsening vision loss.1-3
– Determine whether the visual deficit occurs in one eye or both eyes.
– Determine the quality and area of visual loss (is it both sides and one particular area of visual loss).
– Ask about pain. Acute glaucoma may present with deep, boring pain and nausea/vomiting, while endophthalmitis also presents with boring pain. Optic neuritis is associated with increased pain with eye movement.
– Evaluate for redness and discharge.
– Determine whether trauma was involved. Uveitis/Iritis can cause decreased vision, as can ruptured globe, hyphema, traumatic cataract, or retinal detachment.
– Evaluate for other symptoms such as neurologic deficit (including weakness accompanying a stroke).
The past medical history including vascular disease (diabetes, hypertension, hypercoagulability, etc.), refractive status (near-sighted individuals are at higher risk for retinal tears and detachment), use of contact lens (risk for keratitis, abrasion, ulcer), history of eye surgery (increased patient risk for uveitis, iritis, glaucoma, retinal detachment, and infection), and finally medications (which often have visual side effects) must be obtained.1-3
Medications affecting vision include anticholinergics (accommodation loss, glaucoma), bisphosphonates (uveitis), digoxin (yellow tinged vision), rifabutin (uveitis), sildenafil (blue tinged vision, ischemic neuropathy), sulfa agents (myopia), topiramate (glaucoma), OCPs (ischemic events), and cancer medications.
Pearl 2: Be comfortable with the full ophthalmologic exam, including slit lamp and ultrasound (US).
These evaluations can provide a great deal of information and narrow your differential.
Physical examination – After the focused history, a complete physical exam can provide a great deal of vital information. Many emergency physicians are uncomfortable completing ophthalmologic exams, but this is an essential aspect of the care we provide. The following should be assessed in the patient with visual loss.1-3
- General Inspection: evaluate the lids and sclera closely for erythema, tearing, light sensitivity, proptosis, and ptosis.
- Visual acuity can be assessed before the patient is roomed for provider evaluation. Acuity should be completed with correction based on a Snellen Eye Chart, each eye separately and then together. If the patient does not have glasses with them, a pinhole can be used to assist with correction. If unable to see the letters, hand motion or movement should be assessed.
- Pupils for symmetry, light reactivity, and pupillary reflex.
- Extraocular movements including cranial nerves III, IV, and VI.
- Confrontation visual fields.
- Apply fluorescein and evaluate for abrasion, ulcer, and Seidel’s sign.
- Evaluate intraocular pressure by tonometry. Normal values are 10-20 mm Hg.
- Slit lamp evaluating the anterior and posterior chambers is important for visualization of cell and flare.
- Ocular US is a high yield test for emergency physicians. The anterior chamber, lens, posterior chamber/retina, and optic nerve can be evaluated using US, making this essential in ocular evaluation.
Pearl 3: Know the indications for and conditions that require emergent and urgent ophthalmologic evaluation.
What conditions require immediate evaluation/treatment, and along the same lines, what conditions require ophthalmologist evaluation the same day?
Immediate treatment is needed for acute central retinal artery occlusion, acute glaucoma, and giant cell arteritis. Emergent referral to ophthalmology is required for open globe, chemical burn, endophthalmitis, hyphema, retinal detachment, and infectious keratitis. Urgent referral, or evaluation within 24-48 hours, is needed for uveitis, vitreous hemorrhage, acute maculopathy, central retinal vein occlusion, and optic neuritis.1-3
This post will discuss several conditions emergency physicians will commonly evaluate and manage. Keep in mind this list with descriptions is not all encompassing.
Pearl 4: Use a systematic approach to the differential in acute vision loss: either by anatomy or whether pain is present.
- Media problems:
- Open globe is one ophthalmologic condition that requires immediate treatment. Any trauma including paintball or BB guns can cause open globe, and the majority of patients are male. This injury is normally apparent on exam, which reveals laceration, volume loss of eye, uveal prolapse, peaked/eccentric pupil, 360 degree subconjunctival hemorrhage, or a foreign body. Visual acuity is often significantly decreased. Ophthalmology should be immediately consulted, and CT scan is often required for foreign body evaluation. Treatment requires keeping the patient NPO, avoiding FB removal, avoiding eye manipulation, eye shield placement, head of bed elevation to at least 30 degrees, aggressive nausea treatment, analgesia, and IV antibiotics including vancomycin plus fluoroquinolone or ceftazidime. Urgent surgical repair within 24 hours of injury is associated with the best outcomes.1-3,4-6


Globe injury with eccentric pupil, foreign body, corneal irregularity. Image from https://dailyem.wordpress.com/2012/06/27/ruptured-globe-management-in-the-ed/
- Conjunctivitis is rarely a cause of vision loss, except in the case of chlamydia trachomatis. On the other hand, keratitis can contribute to vision loss. Infectious causes include bacteria, herpes simplex, and adenovirus.1-3,7,8
- Hyphema is a collection of blood in the anterior chamber, most commonly resulting from blunt trauma. Hyphema size is related to outcome. Vision loss occurs in the setting of large hyphema (as the visual axis is obstructed), as well as the development of rebleeding or acute glaucoma. Evaluate for other signs of trauma, including other ophthalmologic trauma. Emergent ophthalmology consultation is needed in the setting of marked decreased VA, signs of open globe, or large circumferential hemorrhage. Same day evaluation is recommended for patients with hyphema and intense eye pain, grossly visible blood in the anterior chamber, or damage to adjacent structures. In the setting of significant hyphema, labs (CBC, coagulation panel, sickle cell testing), and CT should be completed. Treatment is similar to patients with open globe. Nausea should be treated, and pain controlled with topical pain treatment including cycloplegics if open globe has been excluded.1-3,9-12
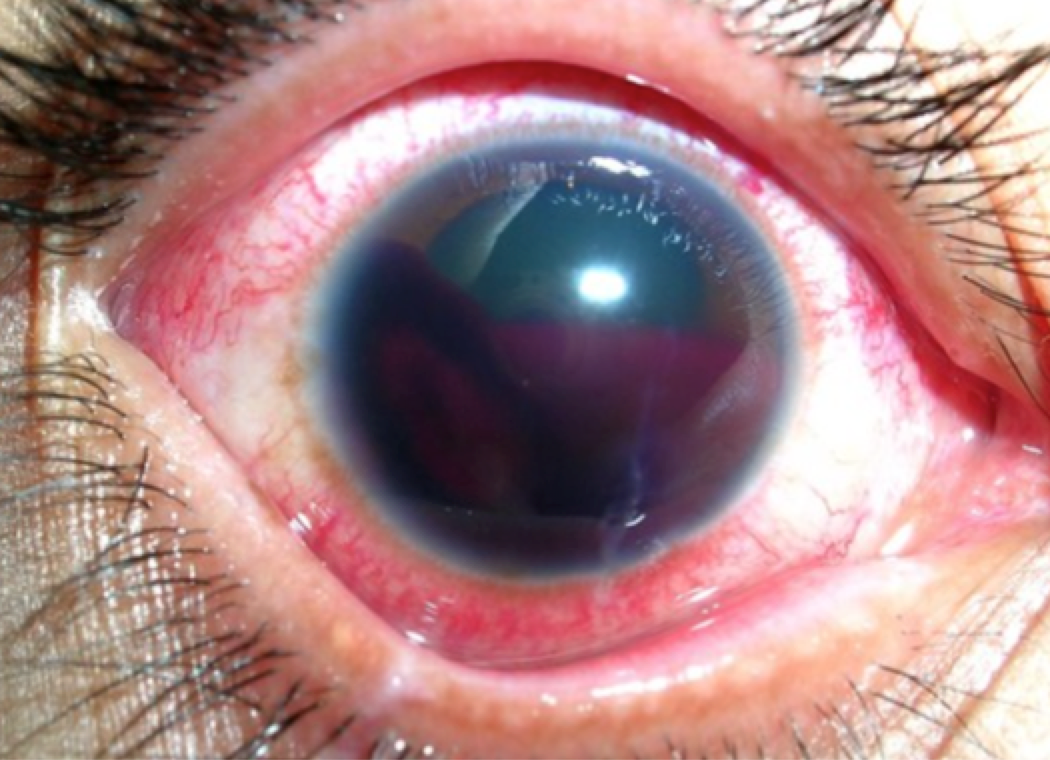
Severe hyphema with RBC layering. Image from http://firstaidtrainers.ca/wp-content/uploads/2013/03/hyphema.jpg
- Iritis often results in pain, photophobia, and vision loss in the extreme form. This is often deep, aching pain that radiates to the temporal regions. Trauma, infection, and rheumatologic conditions may result in iritis. Exam will reveal ciliary flush (erythema closer to the iris as opposed to the periphery), consensual photophobia, and slit lamp with cells and flare with hypopyon. Treatment requires cycloplegics (homatropine 1 drop TID, cyclopentolate 1 drop TID) and ophthalmology evaluation. Steroids can be used but only in association with ophthalmologist consultation. 1-3,13-15
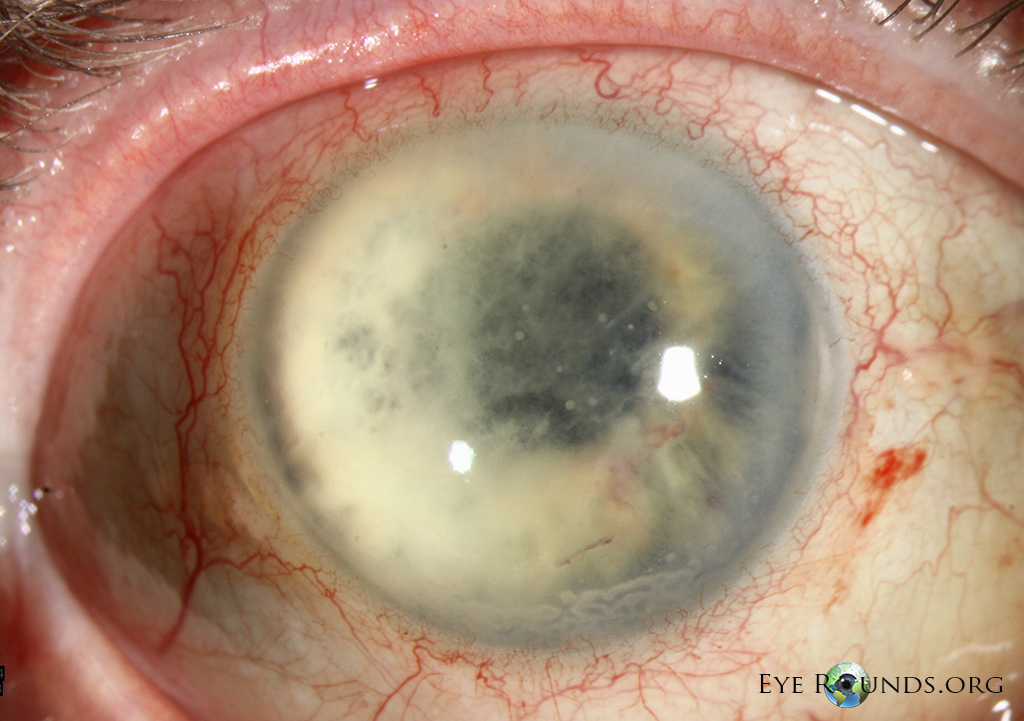
- Glaucoma, particularly acute angle closure, often presents with acute painful vision loss. Nausea/vomiting, blurry vision with halos around lights, and photophobia are other common symptoms. Diagnosis requires intraocular pressure > 21 mm Hg (usually greater than 40 mm Hg), conjunctival injection, corneal edema with hazy/fixed/dilated pupil, and shallow anterior chamber. Risk factors include far-sighted patients, transition from light to dark environments, and dilating medications. Management requires immediate ophthalmologic consultation, followed by medications including topical beta-blocker (timolol 0.25-0.5%), topical cholinergic agent (pilocarpine 1 drop) after timolol, and parenteral acetazolamide 500 mg IV with mannitol 1.25-2g/kg IV if required.1-3,16,17
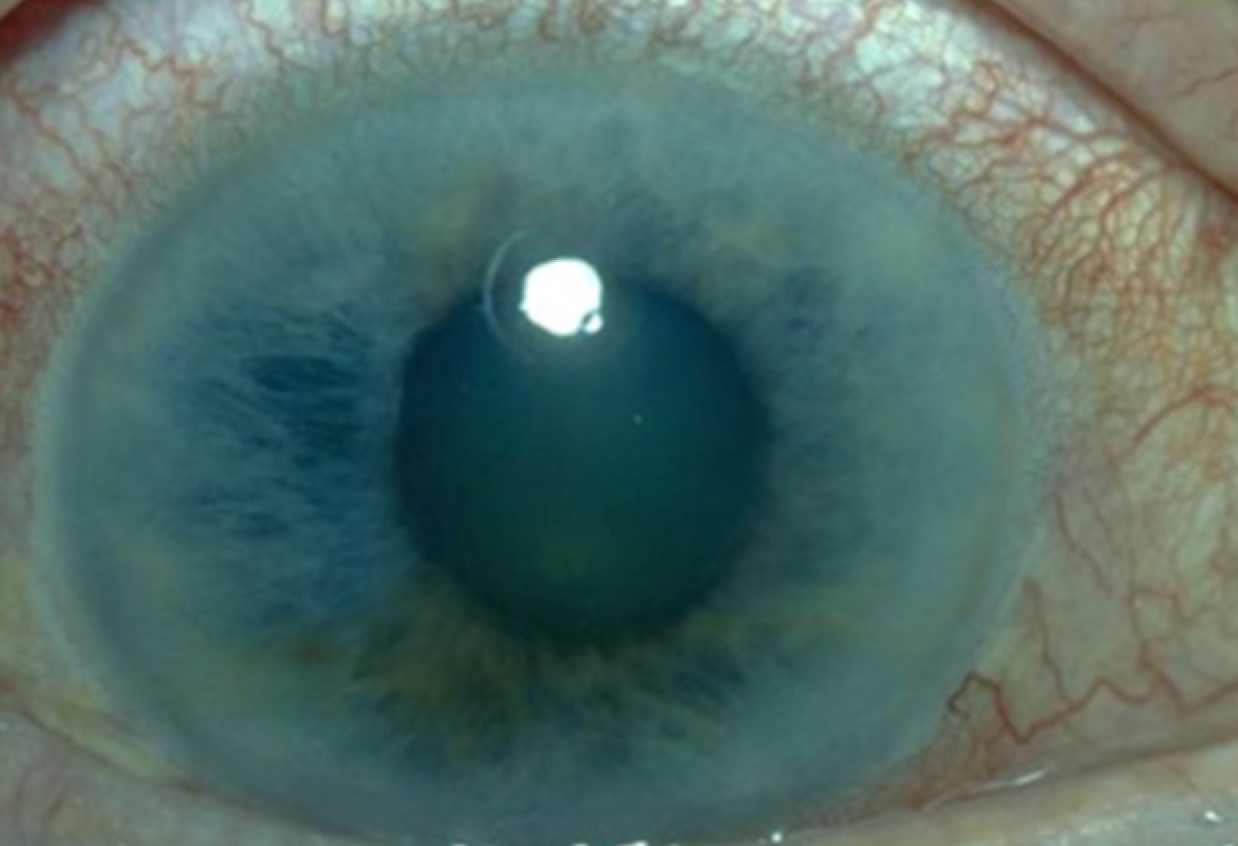
Acute angle closure glaucoma with hazy cornea and mid-dilated pupil. Image from http://images.medicinenet.com/images/slideshow/eye_diseases_and_cond_s3_glaucoma.jpg
- Vitreous hemorrhage often occurs with trauma, though spontaneous vitreous detachment and retinal tear can also result in this condition. The amount of blood contained in the vitreous is proportional to the amount of vision loss. Symptoms include floaters, reddish tint to vision, and brief flashes of light seen by the patient in peripheral vision fields (known as photopsia). Decreased red reflex is often seen on exam, and the retina may not be visible on fundoscopy due to the presence of blood. US will reveal horizontal, minimally echogenic structures behind the lens. Treatment includes ensuring patient head elevation to 30–45° and ophthalmologic consultation for definitive treatment. Anticoagulation should be avoided. It often takes months to completely clear the hemorrhage.1-3,18,19
*Of note, it is often difficult to differentiate on US vitreous hemorrhage and retinal detachment. However, there are three distinct findings that will help distinguish the two: retinal detachments can be followed posteriorly to the optic disk, vitreous hemorrhages remain horizontal when the patient moves the eye side to side, and vitreous hemorrhages are often seen in the middle section of the posterior eye.
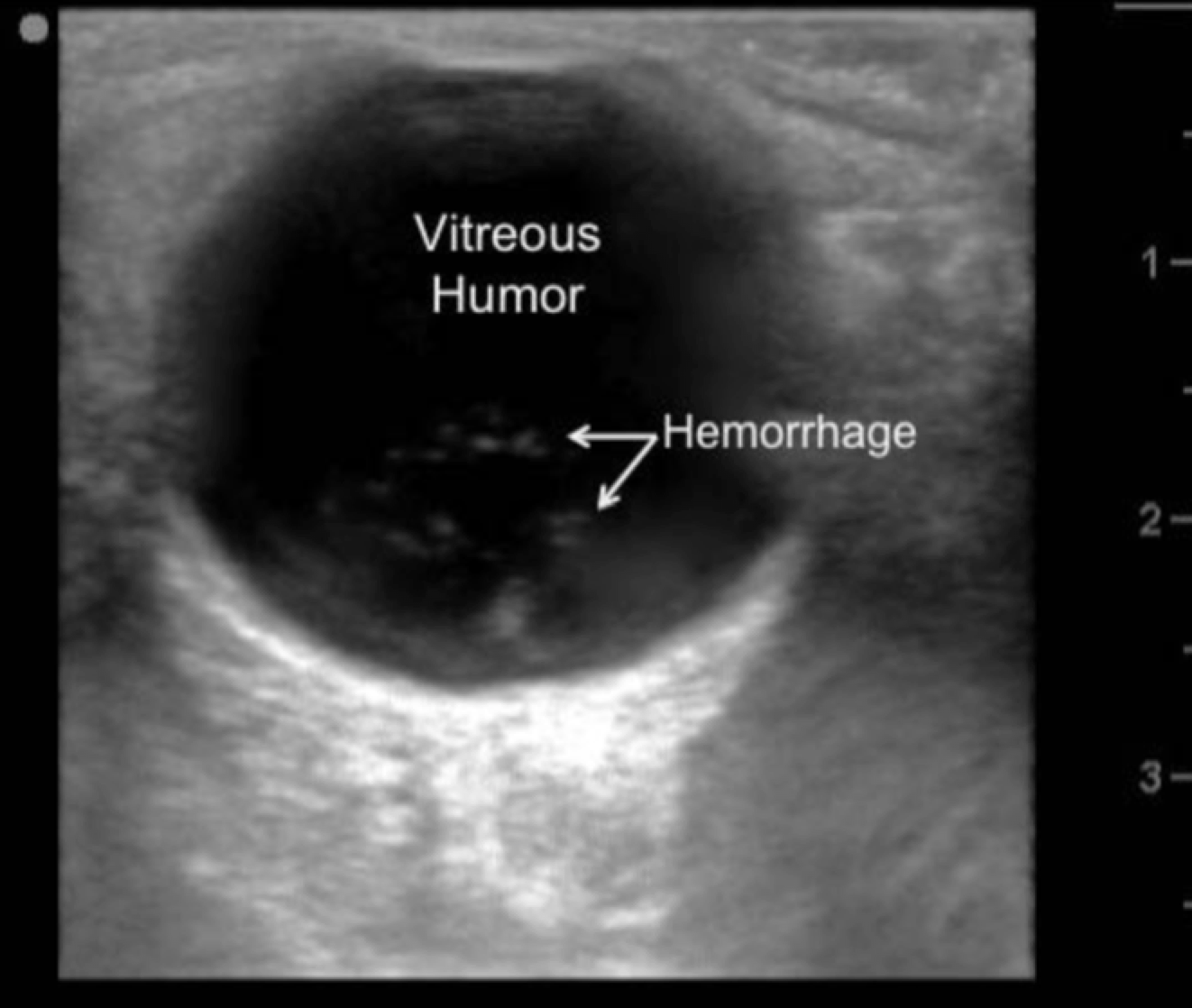
US demonstrating echogenic material in vitreous. Image from http://www.ahcmedia.com/articles/129926-advanced-emergency-ultrasound-applications.
- Posterior vitreous detachment (PVD) is common in patients over 60 years and occurs with vitreous gel pulling away from the retina. . Patients with nearsightedness (myopia) are at greater risk, similar to retinal detachment. This can also occur after cataract surgery. Symptoms include flashes of light and floaters. This may lead to retinal detachment, with greatest risk within the first 6 weeks of symptom onset. These patients require ophthalmology consultation.1-3,19
- Endophthalmitis refers to infection in the eye, particularly of the vitreous and aqueous humor. This is usually due to inoculation of organisms through trauma, surgery, or keratitis. Symptoms progress quickly over 12 to 24 hours including decreased vision and dull eye pain, though patients commonly display no signs of sepsis (SIRS negative). The lids are often normal, but the conjunctiva will be injected and edematous. Decreased VA with hypopyon is often found with haziness of the retinal view. Cells and flare will be seen on slit lamp. US may demonstrate increased echogenicity within the vitreous material. This disease is a medical emergency requiring ophthalmologic evaluation for vitrectomy and antibiotics (vancomycin and ceftazidime) injected into the vitreous material. Intravenous antibiotics can be provided, but they will not be effective in clearing infection.1-3,16,20

Endophthalmitis with hazy cornea and hypopyon. Image from http://www.eyerounds.org/atlas/pages/endophthalmitis-sp/Fungal-Endo-LRG.jpg
- Lens pathology can affect vision. Any change in the size, clarity, or positioning of the lens changes the focus of light on the retina, which results in vision changes. Trauma causing lens dislocation is the most common cause of sudden vision loss due to lens pathology. Chronic cataracts will cause gradual vision loss.1-3

Dislocated lens found on US. Image from http://lifeinthefastlane.com/ophthalmology-befuddler-015/
2. Retina:
- Retinal detachment can occur in the setting of trauma but is often not associated with an instigating event. Three mechanisms exist: rhegmatogenous (most common), exudative, and tractional. Sudden onset of new floaters, black dots, and flashes of light are common symptoms. Early stages may present with visual field loss, but if the macula or central retina becomes involved, visual acuity is severely affected. This is not painful. Afferent pupillary defect may be present, but no signs of red eye will be present. US will be the key to diagnosis, which will demonstrate a highly reflective, mobile undulating membrane. Treatment requires emergent ophthalmology consultation and evaluation.1-3,16,18,21
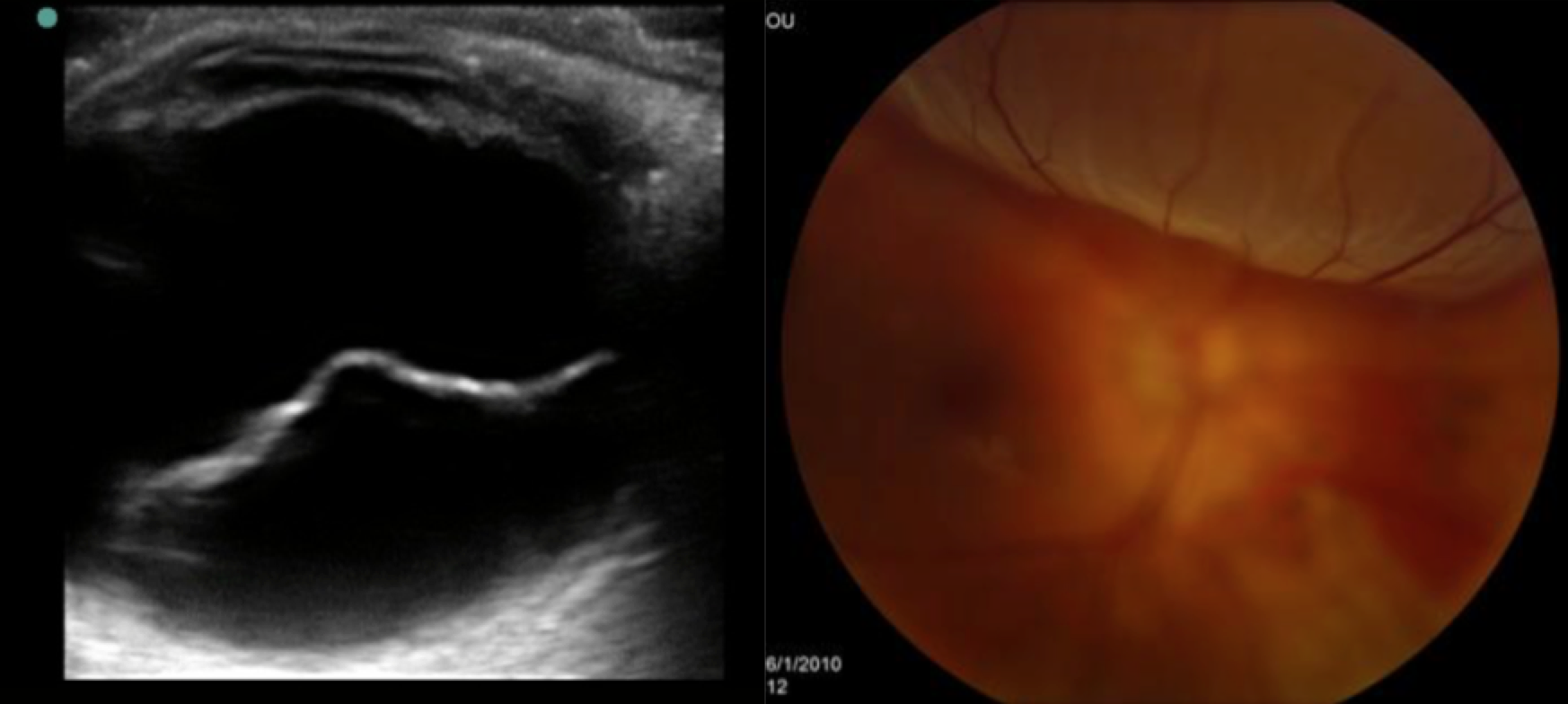
US (left) and fundoscopy (right) of retinal detachment. Images from http://emedicine.medscape.com/article/798501-overview
- Vascular occlusion consists of central retinal artery occlusion (CRAO) and central retinal vein occlusion (CRVO). CRAO presents with sudden, painless, severe vision loss, usually monocular and central. VA is seriously affected. This disease usually affects elderly patients with carotid vascular disease, though pediatric patients with blood disorders including leukemia or sickle cell disease can experience this. A pale retina with cherry red macula is seen on fundoscopic exam. Evaluation with ECG, CBC, coag panel, echocardiogram (for emboli), and carotid US is needed. Ophthalmology emergent evaluation is needed. Ocular massage with intermittent pressure applied, timolol ophthalmic drops, increase PCO2 (rebreathing or carbogen), and acetazolamide IV are standard ED treatments, but ophthalmology consultation is required.1-3,16,23,24
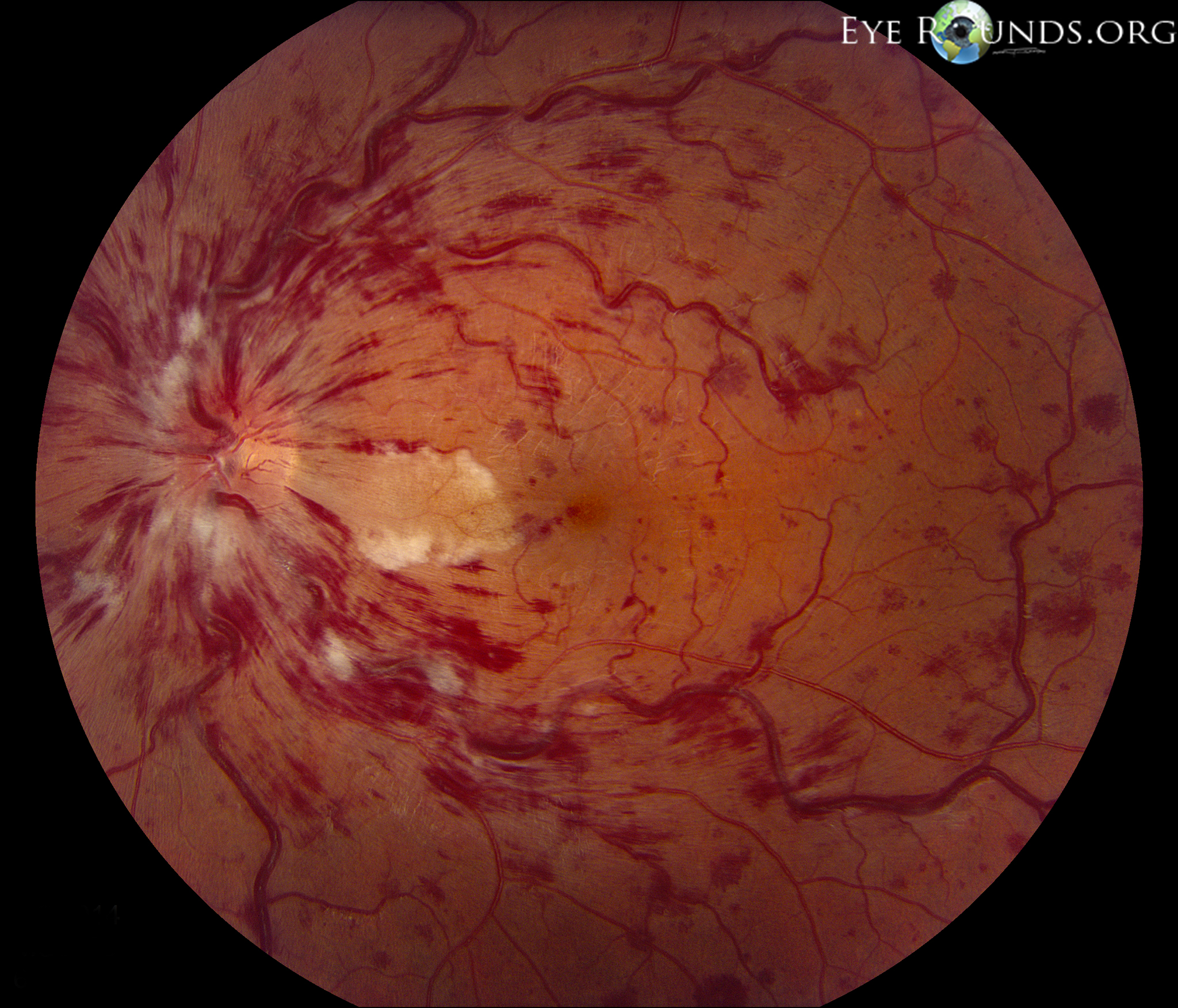
- CRVO is due to thrombosis of the central retinal vein with disc swelling, preretinal hemorrhage, and cotton wool spots with the classic “blood and thunder” appearance. The onset is typically subacute as opposed to the sudden onset vision loss of CRAO. A relative pupillary defect is common. Risk factors include HTN, DM, vasculitis, and glaucoma. Diagnosis is with fundoscopy. Ophthalmology should be consulted, but unfortunately no treatment regimen provides consistent results. Possible treatments include aspirin, anticoagulation, photocoagulation, and intravitreal injections.1-3,16,24,25
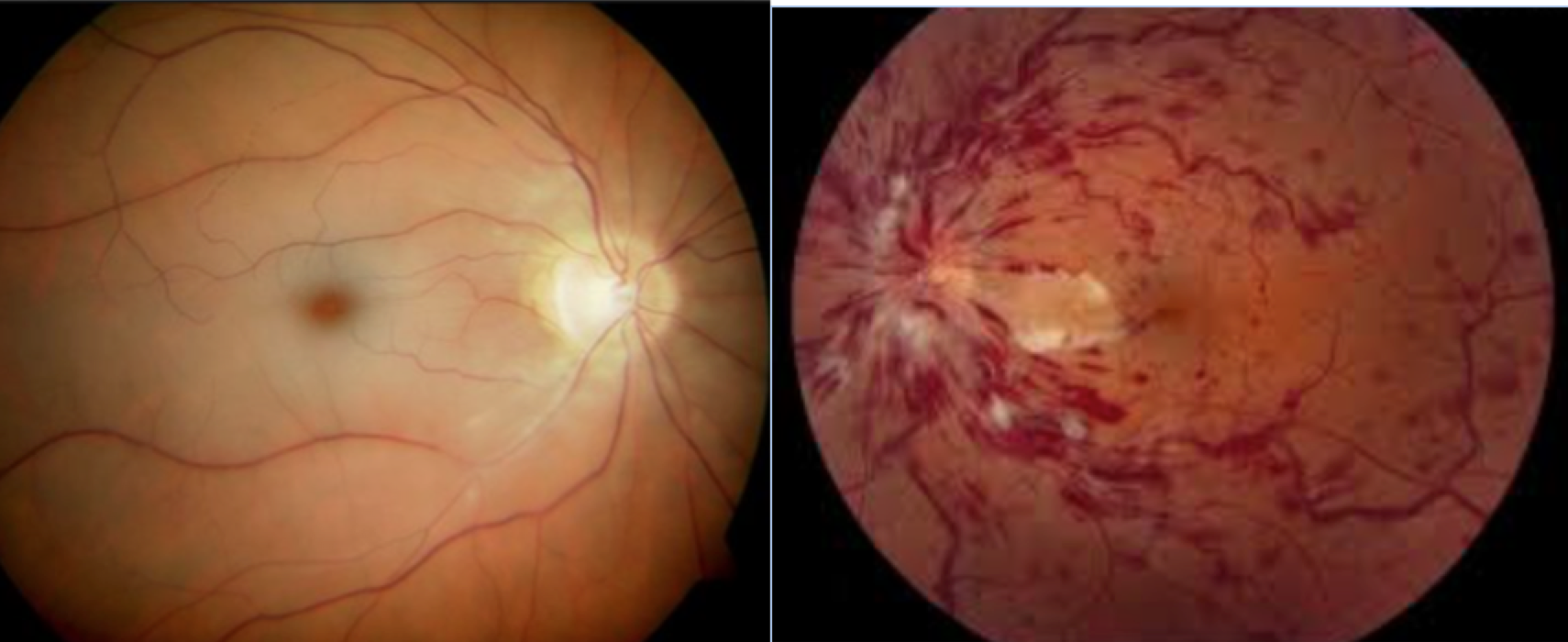
Fundoscopic exam revealing CRAO (Left) and CRVO (Right). Images from http://coloradoretina.com/wp-content/uploads/2008/10/crao1.jpg and http://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/CRVO-w-CLRAO/CRVO-CLRAO-LRG.jpg.
- Acute maculopathy often results in central field vision loss with distortion in other fields. This is usually common and progressive, as opposed to sudden onset. Macula pathology including macular degeneration and diabetic retinopathy are the usual causes. Diagnosis requires dilated ophthalmologic examination.
3. Neural pathway:
- Giant cell arteritis or temporal arteritis can be a cause of CRAO or ischemic optic neuropathy. This disease is predominantly seen in older patients over 50 years. Women and Caucasians are the classic patient population, and the presentation usually entails headache (temporal location), jaw claudication, fever, weight loss, general fatigue, and tenderness to palpation along the temporal artery with decreased pulsation. Jaw claudication and diplopia are most predictive symptoms, with prominent/tender temporal artery the most predictive sign. Elevated ESR and CRP can help suggest diagnosis, but normal values should not rule this out. Definitive diagnosis requires biopsy of the temporal artery. Treatment should be started with high dose methylprednisolone 1g IV in those with vision changes. Vision loss unfortunately is usually complete and irreversible.1-3,26-28
- Optic Neuritis is due to inflammation, demyelination, or degeneration of the optic nerve. It is most commonly seen in females ages 15-45 years. This disease is usually monocular and causes severe eye pain with brief flashes of light. The patient often experiences severe photophobia and decreased red vision, or dyschromatopsia. In children, this may follow bacterial or viral infections, as well as Lyme disease. This can also be a presenting sign of multiple sclerosis, especially in adults. Exam will reveal marked VA decrease with positive afferent pupillary defect. Otherwise, the exam is often normal. Treatment requires IV steroids with methylprednisolone 250 mg IV TID, followed by PO steroids. Further workup requires ophthalmologic consultation and MRI of the head to evaluate for white matter plaque presence.1-3,29-32
- Orbital Infection, particularly orbital cellulitis, leads to visual loss in the later stages of disease. This disease of the posterior orbital septum begins in the sinuses most commonly. Clinical signs/symptoms of orbital cellulitis are fever, proptosis, down and out globe position, limited and often painful eye movements, double vision and later vision loss. Physical examination will reveal the diagnosis, though CT of the orbit is often needed for prognostication and to evaluate the extent of the infection. This disease can rapidly progress intracranially to form abscesses, meningitis, or cavernous sinus thrombosis. Treatment requires admission, IV antibiotics, and ophthalmology/ENT consultation.1-3,33-36
- Cavernous sinus thrombosis may lead to visual loss through thrombosis of ophthalmic vasculature or vessel compression of the optic nerve. This disease often begins with infection in the sinuses. Diagnosis requires MRI/MRV or CTA/venography. Antibiotics with anticoagulation are often needed.1-3,37,38
- Idiopathic intracranial hypertension is due to increased ICP with compression of the optic nerve. No space occupying lesion or infection is present in this disease. Obesity and medications (steroids, tetracycline, vitamin A, ddAVP) are associated with development of this disease. Patients often have headache, transient visual defects, and papilledema. Diagnosis requires imaging with lumbar puncture, which demonstrates elevated pressures. Complete vision loss may occur and starts with transient visual loss.1-3,39,40
- Optic nerve ischemia and nerve avulsion in the setting of trauma may cause blindness. Occipital lobe lesions in the setting of ischemic or hemorrhagic infarction can lead to vision loss acutely as well. This wound be due to ischemia in the posterior circulation of the cerebral vasculature.1-3,16,41
- Optic pathway tumors such as glioma may present with sudden visual loss, but usually visual deficits are progressive over time. The optic chiasm may also be affected, causing bitemporal hemianopia.1-3,42
Pearl 5: Keep in mind other conditions that can lead to blindness beyond intrinsic eye pathology.
4. Ingestions
- Several toxins can lead to blindness. Thus, this must be considered in the ED evaluation of sudden visual loss, especially bilateral. This is often not at the forefront on the ED differential. Methanol overdose causes direct optic nerve toxicity from formate production and can occur up to 72 hours after ingestion. Symptoms often begin with blind spots, decreased color vision, and blurriness. Eye exam may reveal mydriasis, retinal edema, and hyperemia of the optic disk. Afferent pupillary defect is a late finding and poor prognostic finding. Treatment includes fomepazole and ophthalmology consultation.1-3,43,44
- Other toxins or medications leading to cerebral ischemia or hypoxia can contribute to cortical blindness. Optic ischemia with carbon monoxide, direct neurotoxicity from cisplatin, local vasospasm from amphetamines or cocaine, and shock from anti-hypertensive agents (beta and calcium blockers) are associated with blindness. Other toxins affecting vision include barbiturates, chloramphenicol, emetine, ethambutol, isoniazid, and heavy metals.1-3
- Functional vision loss is a diagnosis of exclusion and not a diagnosis in the ED. This is defined as vision loss without organic pathology or disease. Purposeful feigning of blindness occurs with malingering, while patients with conversion disorder perceive true blindness but lack concern for their symptoms. The exam of the eye will be normal. Nystagmus with optokinetic drug can prove vision presence. A second way of evaluating vision is placing a mirror in front of the patient and having the patient open his/her eyes. If the patient tracks the mirror, vision loss is not present.1-3
Case resolutions
Patient 1: Due to concern of optic neuritis, you consult ophthalmology and neurology. MRI brain and C-spine is completed, revealing several white matter lesions. She is admitted and placed on IV steroids.
Patient 2: A quick bedside US confirms retinal detachment. Ophthalmology is consulted.
Patient 3: Labs reveal elevated ESR and CRP. You consult ophthalmology and rheumatology, provide IV steroids, and admit the patient with a diagnosis of temporal arteritis.
Summary:
Ophthalmologic complaints involving sudden vision loss are something many physicians shy away from. However, these conditions can cause significant patient morbidity.
- History including specific eye involvement, sudden vs. chronic loss, pain, redness and discharge, trauma, other symptoms, and medication use are vital.
- Physicians should be comfortable completing an appropriate history and physical examination including general inspection, visual acuity, pupils, EOMs, visual fields, fluorescein, lids, IOP, slit lamp, and US.
- Emergent consultation is required for acute angle closure glaucoma, retinal detachment, CRAO, open globe, endophthalmitis, chemical burn, infectious keratitis, and giant cell arteritis.
- Urgent referral is needed for uveitis, vitreous hemorrhage, acute maculopathy, CRVO, and optic neuritis.
- Keep in mind other etiologies of vision loss including ischemia, stroke, toxin, infection, and functional.
References/Further Reading:
- Burde R, Savino P, Trobe J. Clinical Decisions in Neuro-ophthalmology, 3rd ed, Mosby, 2002.
- Walker RA and Adhikaris. Eye Emergencies. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. Ch. 241.
- Sharma R and Brunette DD. Ophthalmology. Rosen’s Emergency Medicine, Chapter 71, 909-930.e2
- Colby K. Management of open globe injuries. Int Ophthalmol Clin 1999; 39:59.
- Unver YB, Kapran Z, Acar N, Altan T. Ocular trauma score in open-globe injuries. J Trauma 2009; 66:1030.
- Thakker MM, Ray S. Vision-limiting complications in open-globe injuries. Can J Ophthalmol 2006; 41:86.
- Friedlaender MH. A review of the causes and treatment of bacterial and allergic conjunctivitis. Clin Ther 1995; 17:800.
- Weiss A, Brinser JH, Nazar-Stewart V. Acute conjunctivitis in childhood. J Pediatr 1993; 122:10.
- Walton W, Von Hagen S, Grigorian R, Zarbin M. Management of traumatic hyphema. Surv Ophthalmol 2002; 47:297.
- Brandt MT, Haug RH. Traumatic hyphema: a comprehensive review. J Oral Maxillofac Surg 2001; 59:1462.
- Pashby T. Eye injuries in Canadian amateur hockey. Can J Ophthalmol 1985; 20:2.
- Sankar PS, Chen TC, Grosskreutz CL, Pasquale LR. Traumatic hyphema. Int Ophthalmol Clin 2002; 42:57.
- Guly CM, Forrester JV. Investigation and management of uveitis. BMJ 2010; 341:c4976.
- Jabs DA, Busingye J. Approach to the diagnosis of the uveitides. Am J Ophthalmol 2013; 156:228.
- Rosenbaum JT. Nibbling away at the diagnosis of idiopathic uveitis. JAMA Ophthalmol 2015; 133:146.
- Pokhrel PK, Loftus SA. Ocular emergencies. Am Fam Physician 2007; 76:829.
- See JLS, Chew PTK. Angle-closure Glaucoma. In: Ophthalmology, 3rd, Yanoff M, Duker JS. (Eds), Mosby, 2009. p.1162.
- D’Amico DJ. Clinical practice. Primary retinal detachment. N Engl J Med 2008; 359:2346.
- Hikichi T, Trempe CL, Schepens CL. Posterior vitreous detachment as a risk factor for retinal detachment. Ophthalmology 1995; 102:527.
- Mandelbaum S, Forster RK. Exogenous endophthalmitis. In: Ocular Immunology and Infection, Pepose JS, Holland GN, Wilhelmus KR (Eds), Mosby, St. Louis 1996. p.1298.
- Eagle RC Jr. Mechanisms of maculopathy. Ophthalmology 1984; 91:613.
- Hayreh SS, Podhajsky PA, Zimmerman MB. Retinal artery occlusion: associated systemic and ophthalmic abnormalities. Ophthalmology 2009; 116:1928.
- Appen RE, Wray SH, Cogan DG. Central retinal artery occlusion. Am J Ophthalmol 1975; 79:374.
- Hayreh SS, Podhajsky PA, Zimmerman MB. Natural history of visual outcome in central retinal vein occlusion. Ophthalmology 2011; 118:119.
- Risk factors for central retinal vein occlusion. The Eye Disease Case-Control Study Group. Arch Ophthalmol 1996; 114:545.
- Smetana GW, Shmerling RH. Does this patient have temporal arteritis? JAMA 2002; 287:92.
- Younge BR, Cook BE Jr, Bartley GB, et al. Initiation of glucocorticoid therapy: before or after temporal artery biopsy? Mayo Clin Proc 2004; 79:483.
- Hunder GG. Giant cell arteritis and polymyalgia rheumatica. In: Textbook of Rheumatology, 5th, Kelly WN, Harris ED, Ruddy S, Sledge CB (Eds), WB Saunders, Philadelphia 1996.
- Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med 2006; 354:1273.
- Foroozan R, Buono LM, Savino PJ, Sergott RC. Acute demyelinating optic neuritis. Curr Opin Ophthalmol 2002; 13:375.
- Frohman EM, Frohman TC, Zee DS, et al. The neuro-ophthalmology of multiple sclerosis. Lancet Neurol 2005; 4:111.
- Arnold AC. Evolving management of optic neuritis and multiple sclerosis. Am J Ophthalmol 2005; 139:1101.
- Seltz LB, Smith J, Durairaj VD, et al. Microbiology and antibiotic management of orbital cellulitis. Pediatrics 2011; 127:e566.
- Nageswaran S, Woods CR, Benjamin DK Jr, et al. Orbital cellulitis in children. Pediatr Infect Dis J 2006; 25:695.
- Zhang J, Stringer MD. Ophthalmic and facial veins are not valveless. Clin Experiment Ophthalmol 2010; 38:502.
- Mills R. Orbital and periorbital sepsis. J Laryngol Otol 1987; 101:1242.
- Ferro JM, Canhão P, Stam J, et al. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke 2004; 35:664.
- Saposnik G, Barinagarrementeria F, Brown RD Jr, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011; 42:1158.
- Acheson JF. Idiopathic intracranial hypertension and visual function. Br Med Bull 2006; 79-80:233.
- Wall M, Kupersmith MJ, Kieburtz KD, et al. The idiopathic intracranial hypertension treatment trial: clinical profile at baseline. JAMA Neurol 2014; 71:693.
- Rucker JC, Biousse V, Newman NJ. Ischemic optic neuropathies. Curr Opin Neurol 2004; 17:27.
- Alvord EC Jr, Lofton S. Gliomas of the optic nerve or chiasm. Outcome by patients’ age, tumor site, and treatment. J Neurosurg 1988; 68:85.
- Barceloux DG, Bond GR, Krenzelok EP, et al. American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol 2002; 40:415.
- Sivilotti ML. Methanol intoxication. Ann Emerg Med 2000; 35:313.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
6 thoughts on “Acute Visual Loss in the Emergency Department: Pearls and Pitfalls”
Pingback: Asynchronous Learning: ENT, OMFS, Ophtho - Bold City Emergency Medicine
Pingback: A-Sync July Week 1: Eyes Gone Awry – Alamo City EM
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Central Retinal Artery Occlusion - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Corneal Ulcer - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Central Retinal Vein Occlusion - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationThe EM Educator Series: Hey Doc, I can’t see - emDOCs.net - Emergency Medicine Education