
Authors: Karan Gadhok, MD and Hilary E. Fairbrother, MD, MPH, FACEP // Edited by: Alex Koyfman, MD (@EMHighAK) & Justin Bright, MD
Injury is a leading cause of mortality for children and adults from 1-44 years of age1. Abdominal injuries are found in 20-30% of patients with multi-organ injuries. Common causes of abdominal injury include blunt trauma (motor vehicle accidents (MVAs) and falls), and penetrating trauma (gunshot wounds (GSWs) and stabbings). Common abdominal organ injuries involve the liver, spleen, kidneys, intestines and vasculature. This review examines the latest literature in management of abdominal trauma.
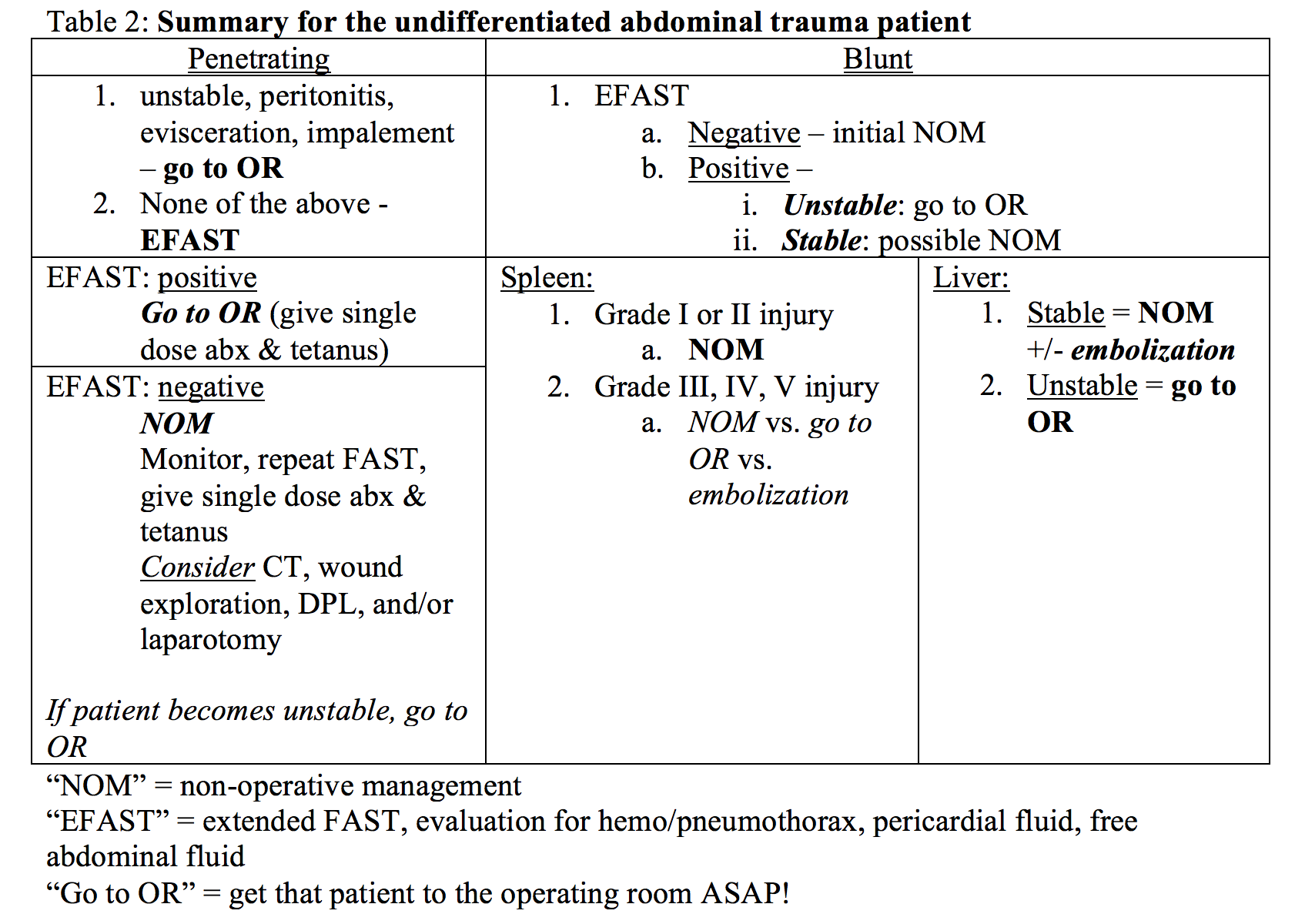
Blunt trauma
The spleen is the most frequently injured organ in blunt abdominal trauma with involvement in up to 46% of blunt trauma cases. Injuries to other organs include: liver (41.7%), kidneys (16.4%), mesentery (15.1%), small bowel (10.1%), large bowel (6.3%), and pancreas (5%). If the pancreas and omentum are involved, typically the spleen is injured as well. Current emphasis in trauma literature is on increasing observation and expectant management. Some of the advantages of non-operative management (NOM) include lower hospital cost, earlier discharge, avoidance of non-therapeutic celiotomies, fewer intra-abdominal complications, and reduced transfusion rates2.
Spleen:
Splenic injuries are the most common solid organ injury associated with blunt abdominal trauma due to its highly vascularized parenchyma and anatomical location. Surgery remains the gold standard for treating patients with splenic injury and hemodynamic instability (31-50% of cases). The general trend has been towards spleen-saving management. Minor splenic injuries (grade I and II) have been well studied; non-operative management (NOM) is used extensively in this patient population. The treatment of grade IV and V splenic injuries is still debated. A recent meta-analysis studying the safety and effectiveness of non-operative management in blunt splenic trauma concluded that no consensus in management for high-grade splenic trauma could be made due to the poor quality of retrospective studies currently published3.
Splenic Embolization: Patients with severe splenic injuries and active bleeding may benefit from splenic angioembolization4. These patients must be hemodynamically stable to be eligible for therapy but it does seem to work. A recent large meta-analysis (n=10,157) looked at patients with grade V spleen injuries with and without embolization and the rate of failure was 25% vs. 83.1% (w/o embolization vs. with, p = 0.0.16)5. Similar results were found for grade IV splenic injuries. This suggests grade IV and V spleen injuries could be considered for NOM with angioembolization or through operative management.

Liver:
The management of blunt liver injury has changed over time from expectant to operative, and now we have a mixed approach. Non-operative management was originally studied in hemodynamically stable children with success leading to further studies and now a paradigm shift in adults. NOM is currently the standard of care for blunt hepatic trauma for hemodynamically stable patients with success rates of 82% to 100%2. Surgery may lead to increased hepatic bleeding and increased incidence of iatrogenic complications.
Per the 2012 Eastern Association for Surgery of Trauma practice guidelines, routine laparotomy is not indicated in hemodynamically stable patients with isolated blunt liver trauma without peritonitis. An abdominal CT scan with IV contrast should be done to grade the severity (level II recommendation). There is also a strong emphasis on embolization as first-line treatment for transient responders to resuscitation. Before this paradigm switch, absolute indications for surgery included hepatic injury with concurrent head injury, any degree of hemoperitoneum, age greater than 55, large number of transfusions, or periportal tracking of blood/blush on CT. However, the current guidelines state that there are no absolute contraindications to a trial of NOM in hemodynamically stable patients2.
Penetrating Trauma
Penetrating trauma is also evolving from the rigid dogma of all penetrating abdominal injuries requiring mandatory laparotomy to selective conservatism7. Absolute indications for laparotomy in penetrating trauma include hemodynamic instability, peritonitis, evisceration, or impalement.
Stab wounds have been considered for selective non-operative management (SNOM) since the 1960s while gunshot wounds (GSWs) have only been considered for SNOM only recently. Patients presenting with abdominal penetrating trauma who are stable and do not meet the above criteria for laparotomy should be considered for SNOM. The only randomized controlled trial for patients with peritoneal penetration without immediate laparotomy showed no difference in outcomes8. In this study 24 patients were randomized to operative care and 27 to NOM. There was no statistical difference in morbidity between the two groups, no mortality in either group, and 15 of 27 patients in the surgical group had a nontherapeutic laparotomy.
Prophylactic Antibiotics: There is still controversy about giving prophylactic antibiotics for penetrating abdominal trauma. To date there are no high quality studies on this subject and practice is primarily based on expert opinion. Current guidelines suggest initiating an antibiotic with aerobic and anaerobic broad-spectrum coverage9 when hollow viscous injury is suspected.17
Tetanus: Don’t forget your tetanus booster. If you or your patient doesn’t know the tetanus status, give the 0.5 mL, intramuscular. Always important in life (and for your oral boards).
FAST/EFAST exam
The Focused Abdominal Sonography of Trauma (FAST) exam has been well established in trauma protocols. The advantages of sonography include speed of assessment, being able to resuscitate the patient while performing the exam, and repeatability. It is non-invasive, which has allowed it to supplant diagnostic peritoneal lavage as the investigative tool to identify blood in the abdomen. A FAST exam can rapidly identify free fluid in the peritoneum and pericardial space. The FAST exam has also been expanded to the EFAST to look for hemothorax and pneumothorax with sensitivity greater than x-ray10.
Blunt: The literature for using FAST in blunt abdominal trauma is insufficient to justify ultrasound being used solely in diagnosis11. The relative risk of mortality is one between those in the ultrasound group and those in the control group based on a Cochrane review. However, ultrasound did significantly reduce the number of CT scans and is a low risk and rapid procedure. It is standard of practice in most institutions to be used on initial exam of the blunt trauma patient. The sensitivity of US in blunt abdominal trauma is not high enough to be a rule-out examination.
Penetrating: The FAST exam for penetrating trauma however has been demonstrated to be more useful. Based on a literature review involving 565 patients, the FAST exam is highly specific (94.1-100%) but not very sensitive (28.1-100%)12. This confirms current understanding of a positive FAST exam having a high incidence of intra-abdominal injury with need for laparotomy. In the case of a negative FAST exam, local wound exploration (LWE), DPL, laparotomy, or CT should be considered.
CT
Thoraco-abdominal CT: CT is used liberally in diagnosing internal injury in both penetrating and blunt trauma in hemodynamically stable patients. Patients who are unstable need resuscitation, immediate surgical management, and should not wait for CT. The question is for stable patients with major trauma, is a routine CT necessary? Based on a literature search in the setting of blunt high-energy trauma, there are no good studies to date to help determine the need for selective thoraco-abdominal CT13.
Whole body CT: There is also a practice of utilizing whole body CT (WBCT) consisting of non-contrast brain and neck CT along with contrast-enhanced scan of the chest, abdomen and pelvis. Based on a recent review of the literature comprising of 25,782 trauma patients receiving WBCT scan vs selective CT scan, there is an overall lower mortality rates in the WBCT group with a p < .000214. This suggests WBCT should be strongly considered in major trauma patients.
Diaphragmatic injury: Something in favor of laparotomy…
Diaphragmatic injuries are uncommon but easily missed in trauma patients and frequently have a delayed presentation. While significant intestinal injuries present themselves within 24-48 hours, diaphragm injuries can go undiagnosed for years. This can lead to organ herniation and bowel strangulation among other morbidities. Based on a recent study, laparotomy confirmed blunt traumatic diaphragmatic injuries were only found 57% of the time on CT scan15. Diaphragmatic injury cannot be ruled out by CT and laparotomy should be considered in high-risk patients.
DPL
Diagnostic Peritoneal Lavage (DPL) has been employed in unstable trauma patients with unclear etiology of their hemodynamic instability when a FAST exam is equivocal. DPL is an invasive test and its use has been significantly decreasing since the utilization of the FAST exam. There are no significant updates in the literature on the use of DPL.
Here is a video from the University of California, San Diego on the DPL => http://youtu.be/O9BZamRlXVA
Efficacies, uses/misuses, what we think they tell us and what they really do
There is a clear trend of change in management from mandatory laparotomy to selective surgery in both penetrating and blunt abdominal trauma. Helping decide the need for laparotomy can include diagnostic modalities. A FAST exam is most helpful in penetrating abdominal trauma patients while whole body CT should be considered in stable major trauma patients with significant mechanisms. However, even a stable patient with negative imaging work-up could have underlying abdominal injury (i.e. don’t forget the diaphragm). The risks and benefits of laparotomy should always be considered in patients with major trauma for possible missed injury on imaging.
References / Further Reading:
- “Leading Causes of Death.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention, 22 Oct. 2014. Accessed November 30th, 2014.
- Stassen NA et al. Nonoperative management of blunt hepatic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012 Nov;73(5 Suppl 4):S288-93.
- Cirocchi R. et al Is non-operative management safe and effective for all splenic blunt trauma? A systematic review. Crit Care. 2013 Sep 3;17(5):R185.
- Sosada K, Wiewióra M, Piecuch J. Literature review of non-operative management of patients with blunt splenic injury: impact of splenic artery embolization. Wideochir Inne Tech Malo Inwazyjne. 2014 Sep;9(3):309-14. Epub 2014 Jul 23.
- Requarth JA, D’Agostino RB Jr, Miller PR. Nonoperative management of adult blunt splenic injury with and without splenic artery embolotherapy: a meta-analysis. J Trauma 2011; 71: 898-903
- “Injury Scoring Scale.” American Association for the Surgery of Trauma, n.d. Web. 30 Nov. 2014.
- Biffl WL et al Management Guidelines for Penetrating Abdominal Trauma. World J Surg. 2014 Oct 15. [Epub ahead of print]
- Oyo-Ita A, Ugare UG, Ikpeme IA. Surgical versus non-surgical management of abdominal injury. Cochrane Database Syst Rev. 2012 Nov 14;11:CD007383.
- Brand M, Grieve A. Prophylactic antibiotics for penetrating abdominal trauma. Cochrane Database Syst Rev. 2013 Nov 18;11:CD007370.
- Kirkpatrick AW et al. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: the Extended Focused Assessment with Sonography for Trauma (EFAST). J Trauma. 2004 Aug;57(2):288-95.
- Stengel D, Bauwens K, Rademacher G, Ekkernkamp A, Güthoff C. Emergency ultrasound-based algorithms for diagnosing blunt abdominal trauma. Cochrane Database Syst Rev. 2013 Jul 31;7:CD004446.
- Quinn AC, Sinert R. What is the utility of the Focused Assessment with Sonography in Trauma (FAST) exam in penetrating torso trauma? Injury. 2011 May;42(5):482-7.
- Van Vugt R, Keus F, Kool D, Deunk J. Selective computed tomography (CT) versus routine thoracoabdominal CT for high-energy blunt-trauma patients. Edwards M. Cochrane Database Syst Rev. 2013 Dec 23;12:CD009743.
- Caputo ND, Stahmer C, Lim G, Shah K. Whole-body computed tomographic scanning leads to better survival as opposed to selective scanning in trauma patients: A systematic review and meta-analysis. J Trauma Acute Care Surg. 2014 Oct;77(4):534-9.
- Sprunt JM et al Computed tomography to diagnose blunt diaphragm injuries: not ready for prime time. Am Surg. 2014 Nov;80(11):1124-7.
- Moore EE1, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, Flint LM, Gennarelli TA, Malangoni MA, Ramenofsky ML, et al. Organ injury scaling: spleen, liver, and kidney. J Trauma. 1989 Dec;29(12):1664-6.
- Goldberg SR1, Anand RJ, Como JJ, Dechert T, Dente C, Luchette FA, Ivatury RR, Duane TM; Eastern Association for the Surgery of Trauma. Prophylactic antibiotic use in penetrating abdominal trauma: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012 Nov;73(5 Suppl 4):S321-5.
- http://www.ncbi.nlm.nih.gov/pubmed/24560871
- http://www.ncbi.nlm.nih.gov/pubmed/23706748




