Originally published at CoreEM.net, who are dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Written by: Jeffrey Dela Cruz, MD // Edited By: Anand Swaminathan, MD
Traumatic Ocular Injuries
Definition: An injury to the eye occurring as a result of direct trauma. It may cause visual changes, eye pain/discomfort, and changes to the appearance of the eye.
Approach: Be methodical with your history and physical. If the patient describes trauma that occurred to the eye, ask about the mechanism of the injury. This will help differentiate possible pathologies. A patient will also describe their eye complaints in a way that will help lead you to a diagnosis, such as having a “foreign body sensation” or seeing “flashing lights.”
Initial exam components needed for diagnosis:
- Visual acuity
- Confrontational visual fields
- Extraocular movements
- Pupillary reactions
- Check for afferent pupillary defect
- Slit lamp exam identifying structures of eye
- +/- Ocular ultrasound (if globe rupture suspected, however, any increased pressure can worsen injury)
Several differential diagnoses to consider:
- Globe Rupture (Open Globe)
- Hyphema
- Retrobulbar hematoma
- Retinal detachment
- Corneal abrasion/ulceration
Globe Rupture

Penetrating Globe Injury – www.dailyem.wordpress.com
Definition: A traumatic injury involving the breakdown in the integrity of the wall of the eye, either the sclera or cornea.
Diagnosis:
- Suspect globe rupture based on mechanism (blunt trauma, projectile injury, laceration of eyelid/periorbital area, metal on metal, high-speed machinery, explosions)
- Physical Exam
- Protruding foreign body in eye
- Eccentric/teardrop pupil
- Decreased visual acuity
- Afferent pupillary defect
- Extrusion of vitreous
- External prolapse of the iris or ciliary body
- Tenting of the sclera or cornea at the site of globe puncture
- Volume loss of eye
- Seidel test à apply fluorescein dye to eye, which binds damaged corneal epithelium and turns green under light through a cobalt-blue filter or Wood lamp, and check for streaming of fluorescein-tinged aqueous humor; this indicates corneal laceration
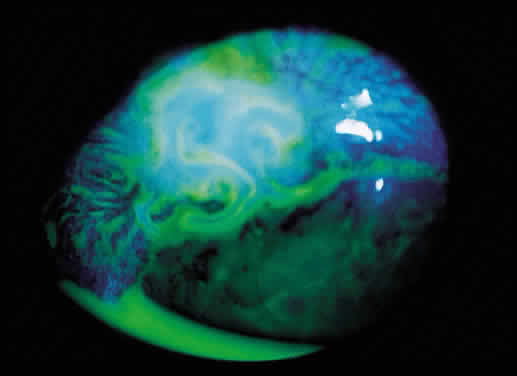
Positive Seidel Test – www.eyecalcs.com
- CT of orbit, sensitivity ranges from 56% to 70%, specificity 79% to 100% (Arey 2007, Hoffstetter 2010
- Prevent increased intraocular pressure (IOP)
- Head of bed at 30 degrees
- Avoid eye manipulation (do not measure eye pressure, retract lid, or perform ocular ultrasound)
- Cover with an eye shield (do not place eye patch as it exerts pressure on globe) – A paper cup can be used if an eye shield is not available
- Administer topical and systemic broad-spectrum antibiotics (Soheilian 2007)
- Update tetanus
- Give antiemetics to prevent nausea (which increases IOP)
- Give pain medicine
- Consult ophthalmology à even if CT negative, formal surgical evaluation may be needed if occult injury suspected
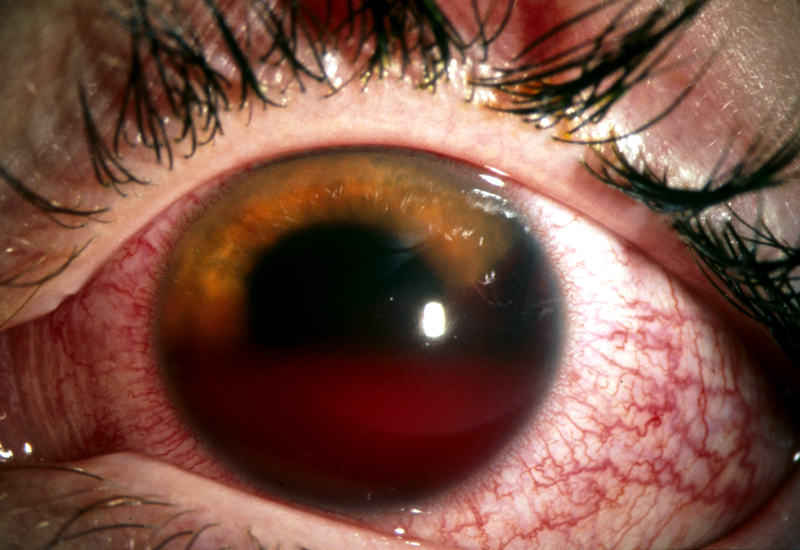
Hyphema
Definition: Blood in the anterior chamber of the eye occurring usually as a result of a ruptured iris root vessel, if secondary to trauma.
Diagnosis:
- Gross inspection of blood in anterior chamber
- Slit lamp exam à check anterior chamber for blood
People at risk:
- Sickle cell disease
- Bleeding diatheses
- Anticoagulant or antiplatelet medications
Management:
- Interventions aimed preventing secondary hemorrhage
- Elevate head of bed
- Dilate pupil
- Control intraocular pressure with topical beta-blockers, topical alpha-adrenergic agonists, or topical carbonic anhydrase inhibitors
- Although recommended, no solid evidence supports the use of cyclopegics, corticosteroids, bed rest, or patching to decrease secondary hemorrhage or affect visual acuity (Gharaibeh 2011)
- Limited studies supporting tranexamic acid and other antifibrinolytics to decrease secondary hemorrhage (Gharaibeh 2011)
- Consult ophthalmology
Retrobulbar Hematoma/Orbital Compartment Syndrome
Definition: Blood found behind the globe but within the orbit, mostly occurring secondary to trauma,

which can lead to optic nerve and retinal ischemia and ultimately, vision loss.
Diagnosis:
- Physical findings
- Proptosis
- Decreased visual acuity
- Afferent pupillary defect
- Decreased extraocular movements
- Increased intraocular pressure (> 40 mmHg)
- CT scan (do not delay management for CT scan if orbital compartment syndrome highly suspected)
Management:
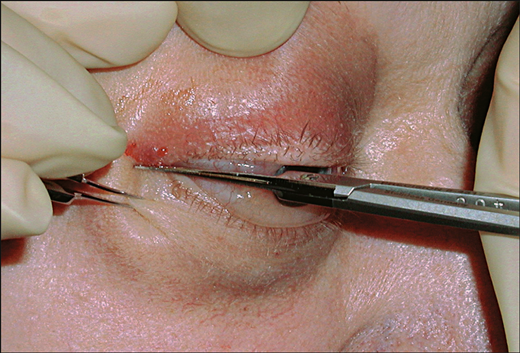
- Consider lateral canthotomy if any of the following (Rowh 2015)
- Decreased visual acuity
- Restricted extraocular movement
- Afferent pupillary defect
- Proptosis
- Intraocular pressure > 40 mmHg
- Expeditious performance of a lateral canthotomy is vision saving. Do not delay.
- Consult ophthalmology emergently
Retinal Detachment
Definition: Retina separates from the underlying retinal pigment epithelium and choroid, either from accumulation of fluid between the two layers or vitreous traction on the retina.

Retinal Detachment on US – sonoguide.com
Diagnosis:
- History (trauma followed by flashing lights/floaters/dark veil/curtains, or history of diabetes/sickle disease with the same complaints)
- Decreased peripheral or central visual acuity
- Direct fundoscopic exam à pale billowing parachute with a large retinal detachment
- Dilated indrect ophthalmoscopic evaluation by ophthalmologist
- Ocular ultrasound à retinal detachment seen as hyperechoic membrane is posterior part of eye, sensitivity ranges from 97% to 100%, specificity 83% to 100% (Vrablik 2015)
Management:
- Consult ophthalmology for surgical repair
Take Home Points:
- Have a low threshold for suspecting globe injury especially if the mechanism is concerning.
- Retrobulbar hematoma/orbital compartment syndrome is a clinical diagnosis; perform a lateral canthotomy if any high-risk findings are present.
- Consult ophthalmology emergently for any traumatic eye injury
References:
- Arey ML et al. Computed tomography in the diagnosis of occult open-globe injuries. Ophthalmology 2007; 114(8):1448-1452. PMID: 17678689
- Hoffstetter P et al. Multidetector CT (MD-CT) in the diagnosis of uncertain open globe injuries. Rofo 2010; 182(2):151-154. PMID: 19859864
- Soheilian M et al. Prophylaxis of acute posttraumatic bacterial endophthalmitis: a multicenter, randomized clinical trial of intraocular antibiotic injection, report 2. Arch Ophthalmol 2007; 125(4):460-465. PMID: 17420365
- Gharaibeh A et al. Medical interventions for traumatic hyphema. Cochrane Database Syst Rev 2011; 19(1): CD005431. PMID: 21249670
- Rowh AD et al. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. J Emerg Med 2015. 48(3):325-330. PMID: 25524455
- Vrablik ME et al. The diagnostic accuracy of bedside ocular ultrasonography for the diagnosis of retinal detachment: a systematic review and meta-analysis. Ann Emerg Med 2015; 65(2):199-203. PMID:24680547





2 thoughts on “Core EM: Traumatic Ocular Injuries”
Pingback: Weekly Review | theNursePath
Pingback: Weekend Knowledge Dump- October 2, 2015 | Active Response Training