
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University School of Medicine, St. Louis, MO); Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine, St. Louis, MO) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 64-year-old male presents by EMS to the ED with shortness of breath. He is hypotensive to 80/50 mm Hg with EMS and hypoxic in the high 80s% on room air.
His vital signs on arrival include HR: 67 bpm, BP: 101/74 mm Hg, RR: 18 bpm, T: 98.3 F, O2 sat: 95% RA
The patient reports that he developed gradually worsening dyspnea over the past month after running out of his medications. He also developed a cough and diffuse abdominal pain over the past few days. You review his chart and note that he had a heart transplant in 2014 but has not followed up with a cardiologist for at least 3 years. The patient also has a distant history of abdominal aortic aneurysm, left above-knee amputation 2/2 peripheral artery disease, atrial fibrillation, and deep vein thrombosis on coumadin.
On physical exam he is awake and alert but ill-appearing. There is pitting edema of the right lower extremity, abdominal distension, and diffuse tenderness. He has mildly increased work of breathing with diminished lung sounds on the right. His extremities are cool to touch.
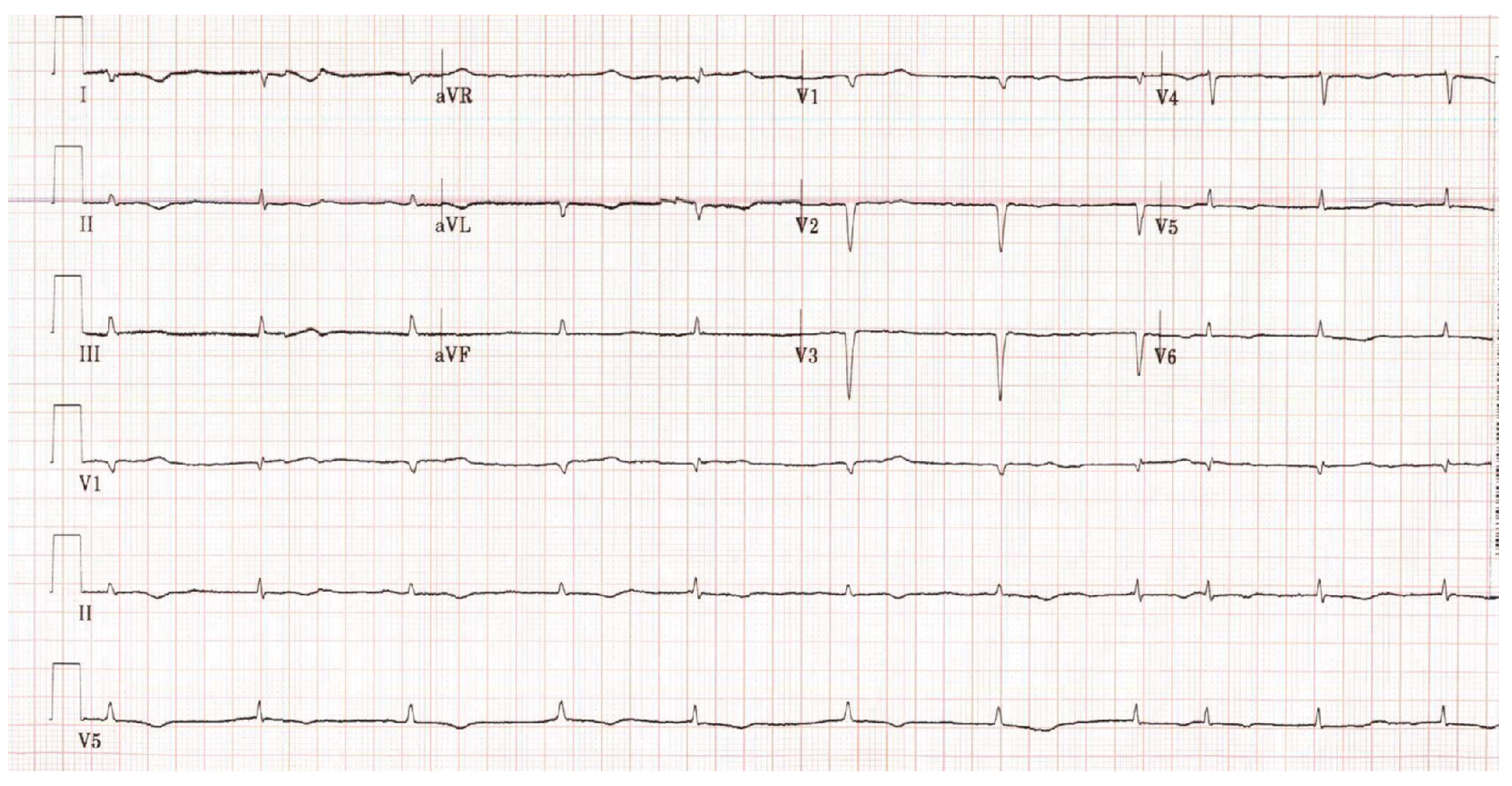
His electrocardiogram (ECG) is shown below:
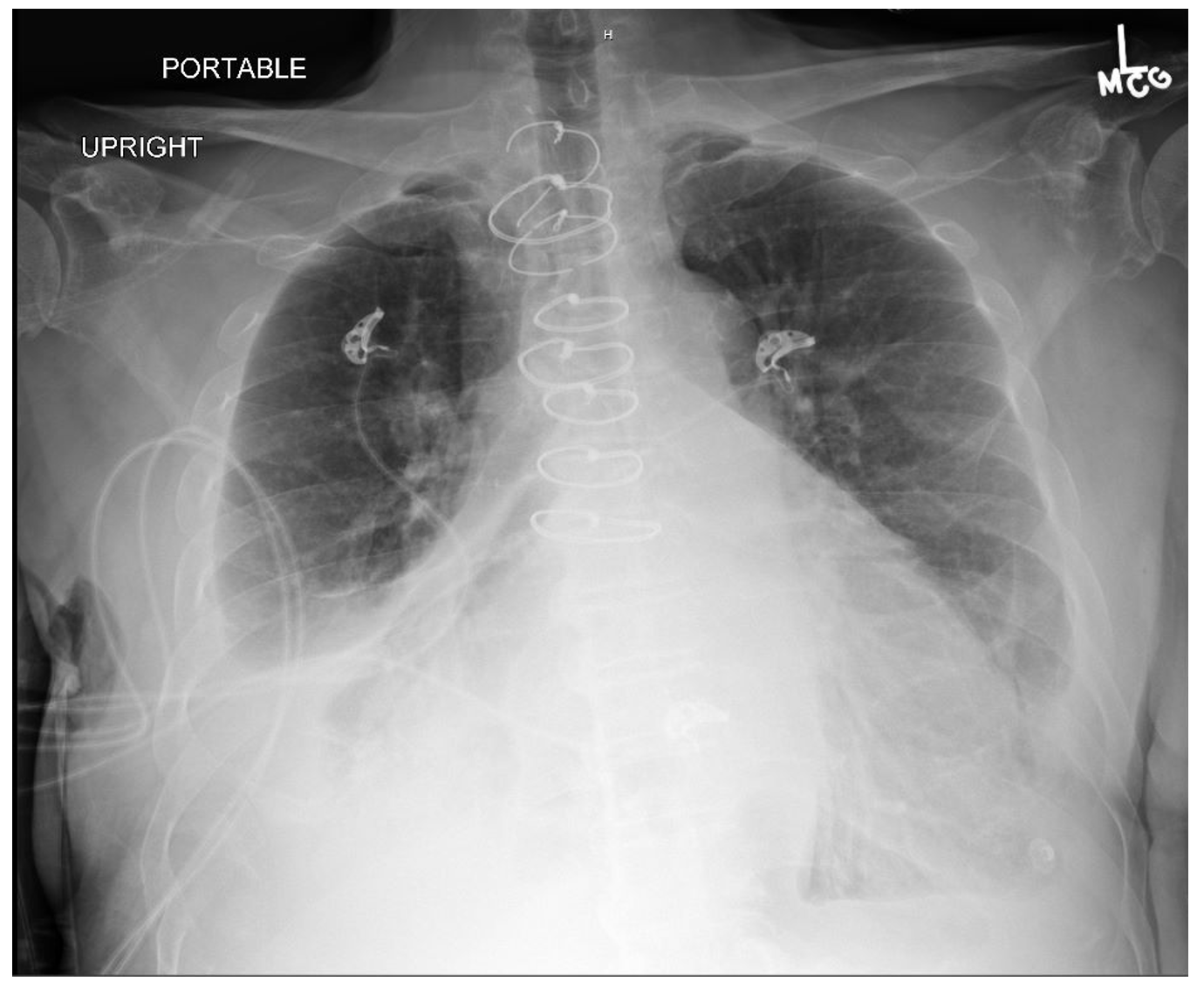
His chest x-ray is shown below:
The patient’s high sensitivity troponin I is elevated to 3,000, and his Brain-Natriuretic Peptide (BNP) is elevated to 14,000 ng/L. A bedside cardiac ultrasound is performed which shows biventricular failure with a dilated inferior vena cava.
What is most likely the cause for his symptoms?
Answer: Cardiac Transplant Complications
Epidemiology:
- There were over 3,000 heart transplants in North America in 2016.1
- Indications for transplant include:
- Non-ischemic cardiomyopathy (49%)
- Ischemic cardiomyopathy (35%)
- Restrictive cardiomyopathy (4%)
- Retransplantation following failed prior transplant (3%)
- Hypertrophic cardiomyopathy (3%)
- Congenital heart disease (3%)
- Valvular cardiomyopathy (3%)
- The median survival after heart transplant is over 12 years.1
- There are over 50,000 visits related to heart transplant in the United States each year and over half of these patients are admitted to the hospital from the ED.2
Anatomy and Physiology:
- There are a few key anatomical differences in our heart transplant patients that ED clinicians must be aware of.
- Most common transplant technique is the bicaval technique.
- Keeps donor right atrium and a portion of the atrial tissue of the recipient.3
- The vagus nerve is usually ligated when a heart transplant is performed.
- Most transplant patients will have a higher resting HR (80-110 bpm) than normal.4
Diagnostic and Treatment Considerations:
- Discuss patient treatment plans with their transplant team.
- Labs:
- Troponin may be elevated until about 3 months after the initial surgery and after that can be interpreted in a similar fashion to other patients.
- BNP should normalize after about 2 months.5
- Treatment of supraventricular tachycardia (SVT):
- Therapies such as vagal maneuvers or atropine are not usually effective.3
- Adenosine can be used, decreased dose of 3 mg in adults => atrioventricular (AV) node is more sensitive than in a native heart.3
- Electrocardiography:
- Depending on the transplant technique, there may be multiple distinct P waves as the native sinoatrial (SA) node is sometimes retained in the atrial tissue in addition to the transplant SA node presence.3
Specific Pathologies:
Acute Graft Failure (Rejection)
- Rejection is a common cause of death in the first month after transplant, with a variety of associated factors (donor vs. recipient factors, transplantation factors, etc.).
- Cardiac transplant failure can manifest with a wide variety of symptoms; have a low threshold to initiate a screening workup on these patients.6-9
- Any cardiac transplant patient with new congestive heart failure (CHF) needs a workup for rejection, including an ECG, chest x-ray, troponin, and BNP followed by an echocardiogram.10
- Missed doses of anti-rejection medications such as corticosteroids, calcineurin inhibitors (tacrolimus, cyclosporine), or other immunosuppressants (Mycophenolate, Azathioprine) increase a heart transplant patient’s risk for rejection.10
- Dysrhythmias (more commonly ventricular), chest pain, dyspnea, acute CHF and shock are all possible.3
- Troponin and BNP are important screening tests and should be followed by an echocardiogram if concern for rejection is high.10
- Discussing the case with the cardiology transplant team early is important so that they can be involved in the decision-making regarding biopsy and immunosuppressant medications (generally methylprednisolone 500-1000 mg/day)) if there is a high probability of rejection.3,10
Coronary Allograft Vasculopathy
- Nicknamed “The Achilles Heel of Heart Transplantation,” this accounts for the majority of patient mortality in the 5-10 year range.12
- This is a variant of coronary artery disease in the allograft vessels, characterized by concentric intimal hyperplasia, as opposed to the eccentric pattern seen in atherosclerosis among non-transplant coronary arteries.10
- It affects the whole length of the vessel and all layers of the coronary vasculature rather than just the intima, which is seen in non-transplant atherosclerosis.10
- Although this is not the same pathophysiology seen in ACS from an acute plaque rupture leading to coronary artery occlusion, patients can have relatively abrupt coronary ischemia causing ACS due to acute, concentric vessel narrowing.3,11
- Recent clean cardiac cath does not rule out ischemia from allograft vasculopathy when these patients present with chest pain or shortness of breath.3
Acute Coronary Syndrome (ACS)
- ACS in heart transplant patients can be caused by (1) coronary allograft vasculopathy => coronary vessel narrowing and decreased blood flow, or (2) acute plaque rupture of atherosclerotic plaque.15
- The exact incidence or acute coronary syndrome in heart transplant patients is not well characterized.15
- Patients with a heart transplant can have ACS though they are unlikely to present with classic, crushing chest pain due to transplant-induced changes in cardiac innervation.3
- Many will experience vague, nonspecific symptoms such as weakness or fatigue.3
- Heart transplant patients with ACS have higher risks for cardiogenic shock and in-hospital mortality compared with the general population.15
- Consider ACS in the differential for transplant patients and have a low threshold for ordering screening ECG/troponin.
- It is difficult to distinguish this from ACS secondary to acute plaque rupture in the ED, and management would be similar with antiplatelet agents, anticoagulation until coronary angiography can be performed to assess for the underlying disease process.3
Infection
- This is a significant cause of mortality in any transplant patient due to high rates of resistant organisms and their immunosuppressed status.8
- They are also at higher risk for opportunistic fungal such as Pneumocystis jirovecii (PJP), Aspergillus fumigatus, and viral pathogens such as cytomegalovirus (CMV), Epstein-Barr virus (EBV), and BK virus.9
- Initial workup if infection is suspected should include blood cultures, lactate, CBC with differential, urinalysis with culture, chest x-ray and further labs and imaging directed towards the suspected source.3
- Empiric antibiotics for septic patients should be broad-spectrum and include coverage of Pseudomonas and MRSA.13
- Cefepime 2 g or Piperacillin-Tazobactam 4.5 g or Meropenem 1 g + Vancomycin 15 mg/kg or Linezolid 600 mg are generally appropriate for septic patients.13
- If there no clear source or there is a high suspicion for a fungal infection in a septic patient, an echinocandin such as Micafungin (100 mg) or Caspofungin (50-70 mg) can be administered.13
- Data demonstrate that early consultation with an infectious disease in cases of suspected infection carries mortality benefit.3
Anti-Rejection Medications
- Common anti-rejection medications include calcineurin inhibitors (Tacrolimus, Cyclosporine), Azathioprine, Mycophenolate mofetil, and corticosteroids.
- Transplant recipients require aggressive immunosuppressant medications and it is dangerous for them to miss doses.6
- Some of these medications, particularly calcineurin inhibitors, interact with commonly seen medications such as antidepressants, statins, antiplatelet agents, anti-epileptics, macrolide antibiotics, calcium channel blockers and amiodarone.3,14
- Always ensure that drugs administered in the ED do not interact with the patient’s transplant medications.
- Discuss anti-rejection therapy modifications if there is a change in the patient’s status such as active infection, acute graft dysfunction, new pregnancy or any concern for drug toxicity with the transplant team.
- In boarding patients, anti-rejection medications may need to be ordered from the ED.
Malignancy
- Cancer, including lymphoma, is a common cause of death 5 years after transplantation.
Take Away Points:
- Discuss all medication changes with the patient’s cardiac transplant team.
- For SVT, avoid vagal maneuvers and use a lower dose (3 mg) of adenosine.
- ACS or acute worsening of coronary allograft vasculopathy may have vague symptoms; order a screening ECG and troponin.
- Cardiac transplant patients are at high risk for infection, including atypical pathogens; consult ID early.
- Any cardiac transplant patient with new CHF needs a workup for rejection.


A 63-year-old man presents to the emergency department for dyspnea on exertion. He has had worsening dyspnea for the last 4 days, which has been most noticeable when climbing stairs, but reports no chest pain. His medical history includes a heart transplantation 10 months ago for cardiac amyloidosis. He now takes mycophenolate daily but notes that he ran out roughly 1 week ago and was unable to refill the prescription due to travel. Vital signs are within normal limits. A chest X-ray is shown above. Which of the following is the best management of this condition?
A) Cardiology consultation for transesophageal echocardiogram
B) Continuation of his home mycophenolate dose and admission for observation
C) IV dobutamine infusion and admission to the cardiovascular ICU
D) IV furosemide and close monitoring of urine output
E) IV methylprednisolone and cardiology consultation for endomyocardial biopsy
Answer: E
Acute cardiac allograft rejection remains a prominent complication of heart transplantation despite recent advances in immunosuppressive therapy. All cardiac transplant recipients are at risk, but the risk increases in the presence of several known donor and recipient factors, including recipients who are younger (< 24 years) and female, donors who are female, and the presence of recipient antibodies against donor antigens. Nonadherence to immunosuppressive therapy is another prominent risk factor that is thought to underlie many cases of rejection in adolescent and young adult recipients (age 17–24 years).
Patients often undergo routine surveillance after cardiac transplantation due to high rates of asymptomatic rejection. Reported clinical symptoms range from mild heart failure and palpitations to cardiogenic shock. Atrial dysrhythmias are a common manifestation. Acute rejection should be suspected in patients in the first year post-transplantation presenting with new cardiac symptoms or objective findings, and endomyocardial biopsy should be performed in cases of high suspicion. While biopsy is the gold standard for diagnosis, many patients will be started on empiric treatment, commonly in the form of corticosteroids. Severe rejection is characterized by hemodynamic compromise and shock and is typically treated with antithymocyte globulin. Hemodynamic support in the form of inotropic or vasopressor agents may also be required in such cases. Additionally, patients who receive high-dose corticosteroids or antithymocyte globulin should be given prophylaxis for opportunistic infections. This often consists of clotrimazole for candidiasis, acyclovir for herpesviruses, and trimethoprim-sulfamethoxazole for Pneumocystis jirovecii.

Transesophageal echocardiogram (A) has higher sensitivity than transthoracic echocardiogram for conditions such as atrial thrombus and vegetations in endocarditis but is not useful in the diagnosis of acute rejection.
Though this patient will eventually require the continuation of his immunosuppressive regimen (B), he requires high-dose corticosteroids or antithymocyte globulin to treat his acute rejection.
Cardiogenic shock in the setting of acute rejection would warrant inotropic agents and ICU admission (C), but these would not be indicated in cases of mild rejection, such as in this patient.
IV furosemide (D) may be a useful adjunctive therapy in the treatment of this patient’s rejection, but corticosteroids are the most important step in definitive treatment and should be instituted at this time.
Further Reading
Additional FOAM Resources:
- https://emcrit.org/ibcc/hyperthermia/#(1)_internal_cooling:_crystalloid
- https://litfl.com/hyperthermia-associated-toxidromes/
- https://litfl.com/hyperthermia/




