
Authors: Jacob Kirkland, MD (EM Resident Physician, UTSW – Dallas, TX); Steve Field, DO (Assistant Professor of EM/Attending Physician, UTSW – Dallas, TX) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 35-year-old right handed male with no significant past medical history presents with a deep hand laceration. The patient states they suffered a cut with a box cutter at a construction site. He presents to the ED with profound difficulty extending his middle and ring finger. Examination reveals the following:

What is the diagnosis?
Answer: Extensor tendon laceration
Epidemiology:
- Hand extensor injuries make up >25% of orthopedic soft tissue injuries2, 3
- Common in young men in manual labor
- Dominant hand more likely to be injured4
- 2012 study on 86 patients reported 83% men with a mean age of 34.2 years and the dominant hand involved 60% of the time4
- Most common finger injuries are thumb (25.7%), index (24.8%), middle (23.8%) fingers, respectively4, 5, 6
Anatomy:
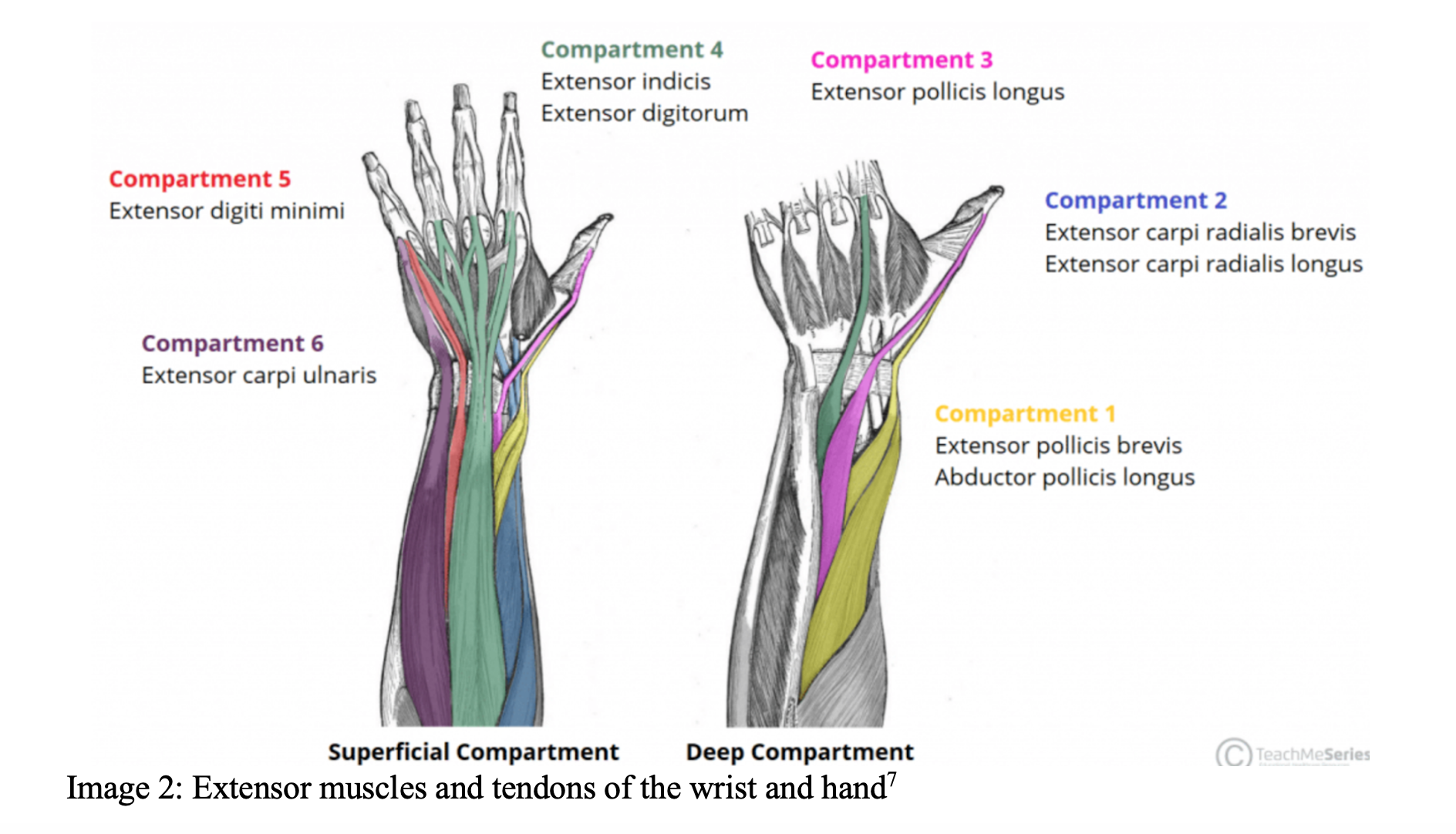
- Tendons are more superficial on the dorsal hand and are therefore more commonly injured8
- Extensor retinaculum overlays the wrist, which can make tendon repair difficult9
- Primary muscles of hand extension
- Primary wrist extensors: Extensor carpi radialis longus/brevis, extensor carpi ulnaris
- Primary thumb extensors: Extensor pollicis longus/brevis, abductor pollicis longus
- Primary finger extension: Extensor digiti minimi, extensor digitorum, extensor indicis
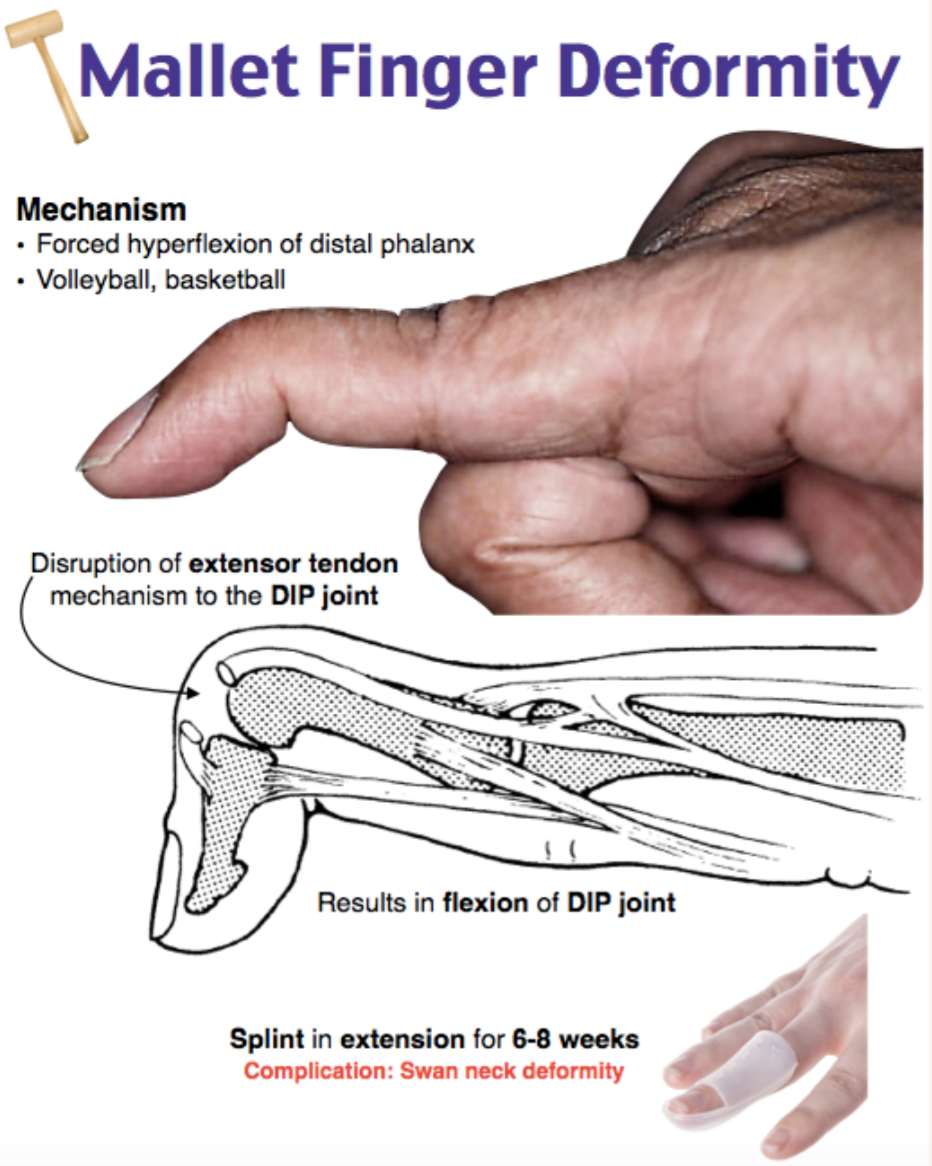
Classic injuries:
Mallet finger
- Forced flexion of the DIP while extended
- May include bony avulsion fracture10, 11
Clinical Presentation:
- Extensor injuries typically from more superficial lacerations to the dorsal surface of the hand
- Loss of strength with extension effected digit(s)
- Deeper lacerations may have neurovascular injury with loss of sensation or motor control
Evaluation:
- History should include mechanism, occupation, handedness, time of injury, tetanus status, prior injuries10
- Examine prior to anesthesia to obtain accurate sensorimotor function10
- Isolate each joint to test strength against resistance
- Test for neurovascular deficits with light touch/pinprick sensation, doppler
- Evaluate for bruising, wounds, deformities
- Adequate anesthesia should be used for wound exploration and decontamination
- Painful nodule may be seen with tendon retraction
- X-ray should be used to identify fractures or retained foreign bodies
- Ultrasound is effective for identifying hand fractures and foreign bodies12
- Ultrasound may be useful to evaluate for tendon disruption13
- Evaluate the zone of injury
Zones of injury
- Tendon zones will help identify structures injured and guide further treatment
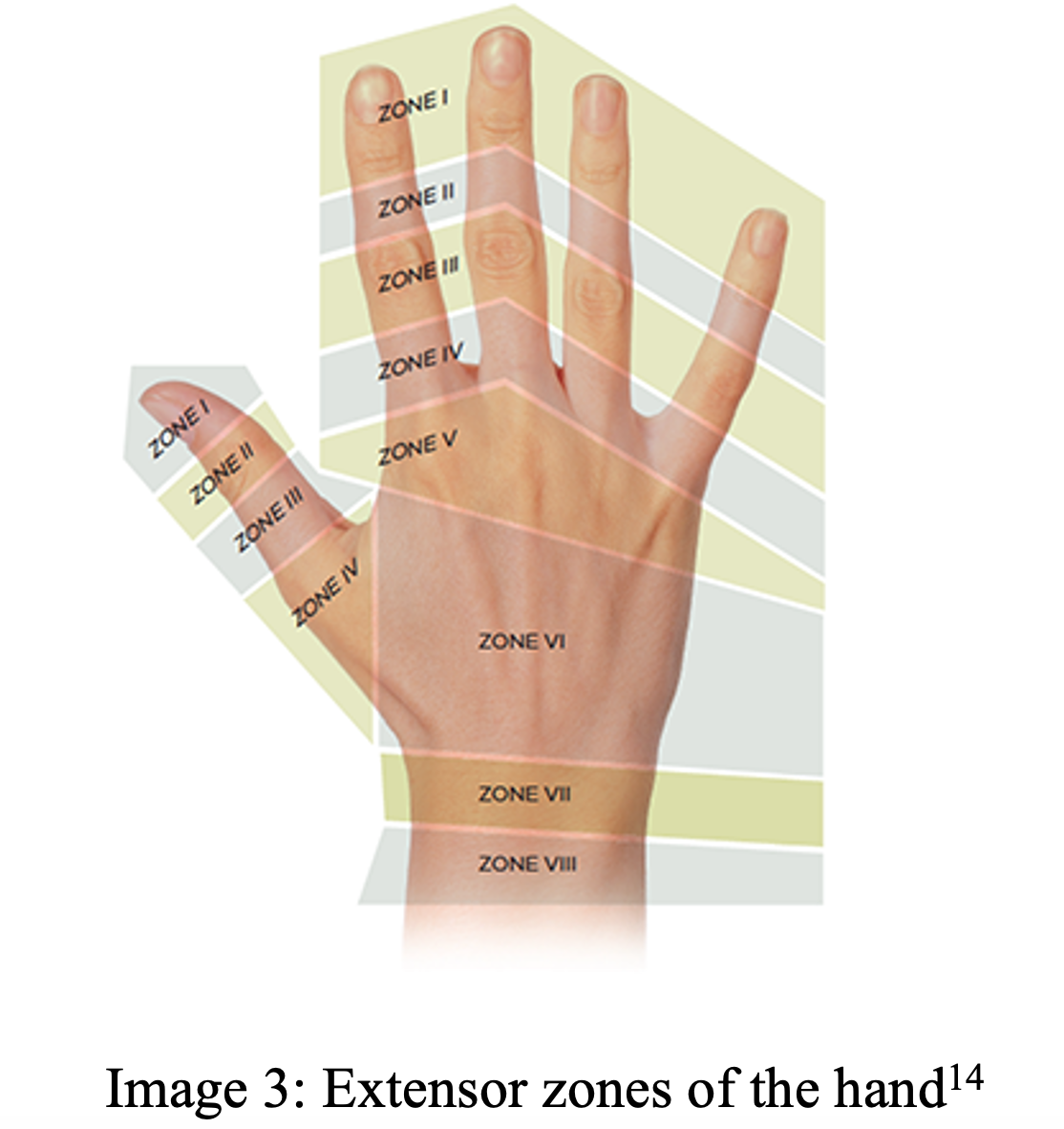
- More relevant as treatment may vary depending on zone
- I: DIP joint – injuries are typically closed injuries14, 15
- II: Middle phalanx
- III: PIP joint
- IV: Proximal phalanx
- V: Metacarpophalangeal (MCP) joint
- VI: Dorsum of the hand
- VII: Wrist
- VIII: Distal forearm
- TI: Interphalangeal (IP) joint of thumb
- TII: Proximal phalanx of thumb
- TIII: MCP of the thumb
- TIV: Carpometacarpal (CMC) joint
Treatment:
- Treatment depends on the zone of injury
- All tendon injuries, open or closed, should be referred to a hand specialist
- In general, patients with simple extensor tendon injuries should be followed up outpatient by a hand specialist, if one is not available in the area, transfer to a higher level of care should be considered
- Most patients get a short course of antibiotics in open tendon injuries, but not required
- Several prospective, randomized control trials show no statistical significance in wound infection with hand lacerations16,17,18
- Cephalexin 500mg for 5-7 days would be appropriate for open tendon injuries
- Consider extensive contamination, open fractures, which would warrant orthopedic consultation
- Type I: open fracture with <1cm clean laceration, minimal soft tissue damage
- Cefazolin 2g IV three times daily in adults
- 30mg/kg three times daily in children
- Cefazolin 2g IV three times daily in adults
- Type II: open fracture with 1-10 cm clean laceration without extensive injury
- Same as Type I
- Type III: open fracture >10cm with extensive soft tissue damage or heavily contaminated/farm injury
- Cefazoline 2G IV Three times daily
- Gentamicin 5-7 mg/kg IV once daily in adults; 2.5 mg/kg IV three times daily in pediatrics19
- Type I: open fracture with <1cm clean laceration, minimal soft tissue damage
- Zone I and II: For closed injuries, place DIP in hyperextension and immobilize finger with a splint for 6-8 weeks21
- Patient compliance with splint will determine success of treatment22
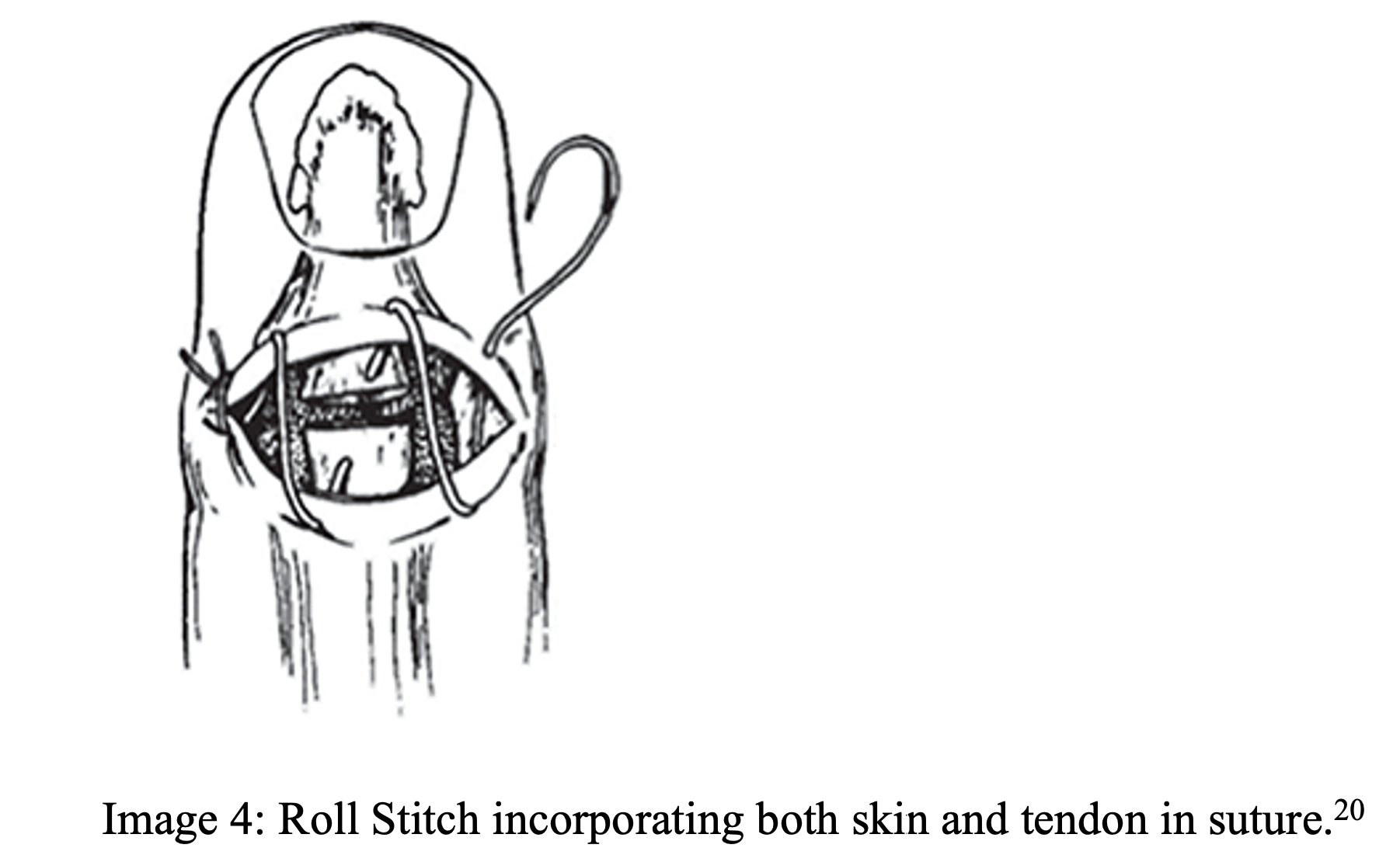
- Open injuries should be repaired with a roll stitch (see image 6)23
- 4-0 or 5-0 non absorbable suture used to involve both skin and tendon
- Zone III: Tendon should not be repaired in the ED
- Repair requires hand specialist to prevent Boutonniere deformity23, 24
- If in a community setting, suture overlying skin, splint wrist in 30° extension, MCP in 15° flexion and PIP in neutral24

- Zone IV: Tendons are larger and more amenable for repair in ED23
- Use modified Kessler/Bunnell technique with low tissue reactivity and high strength suture such as 4-0 ethibond or mersilene (see image 7)25
- Splint similar to zone III injuries
- Zone V: Have a high suspicion for fight bite injuries14, 22
- If physician suspects above, extensively irrigate and do not close skin
- Tendon repair similar to zone IV, splint wrist 45° extension, MCP 20° flexion22
- Patient will need antibiotics i.e. Augmentin if fight bite suspected22
- Amoxicillin/clavulanate 875 mg/125 mg by mouth twice daily in adults
- 25 mg/kg by mouth twice daily in children
- Amoxicillin/clavulanate 875 mg/125 mg by mouth twice daily in adults
- Patient should follow up within 24 hours
- Zone VI: Tendons are large and superficial on the dorsum, making for an easier repair
- Modified Kessler/Bunnell technique with 4-0 non-absorbable sutures similar to above1
- Splint wrist in 30° of extension, MCP neutral with digits free
- Zone VII and VIII: Beyond scope of ED repair
- Junctions with muscle bodies become involved24
- Close overlying skin, place in volar splint, ortho consultation vs urgent referral
- Consider consulting orthopedics or transfer to a center with hand specialist if extensor tendon injury is more proximal to wrist, as this eventually requires surgical repair
- Ensure the patient is up to date with their tetanus vaccination
- Past vaccination unknown or <3 total
- Wound is clean: Td
- Wound is dirty: Td + tetanus immunoglobulin
- At least 3 prior Td vaccinations
- Wound is clean: Td if last vaccine >10 years ago
- Wound is dirty: Td if last vaccine >5 years ago26
- Past vaccination unknown or <3 total
Disposition:
- If there is no extensive injury to soft tissue, patients can be discharged
- Ensure urgent follow-up with orthopedics if there is suspected flexor/extensor damage27
- Concern for open fractures/joints should prompt orthopedics consultation
- Depending on extent of injury/local practice, orthopedics may need ED consultation
Pearls:
- Complete a thorough physical exam, noting neurovascular status as well as isolated joint mobility and strength
- Extensor injuries should be repaired based on location of injury zone
- Use non-absorbable 4-0 suture with modified Kessler or Burnell technique when repairing extensor tendons
- Patients generally have tendon repair, splinting, and outpatient hand specialist follow-up, but consider hand consultation if damage is extensive or consider transferring if no hand specialist for follow up

A 35-year-old woman presents with a left ring finger injury after being kicked in the fingertips while sparring. On exam, the patient is unable to straighten the distal joint of the affected finger. The fingertip remains flexed when the fingers of the left hand are extended. There is pain and swelling around the distal interphalangeal joint. Which specific complication can be prevented if this injury is recognized early?
A) Boutonniere deformity
B) Dupuytren contracture
C) Post-traumatic arthritis
D) Swan-neck deformity
Answer: D
The exam findings are indicative of mallet finger, an injury to the extensor tendon of the distal interphalangeal (DIP) joint. Improper or delayed treatment may lead to the complication of swan-neck deformity. This results in a permanent abnormal flexion of the DIP and involves the central slip. Symptoms often include pain, decreased grip strength, and difficulty with fine motor tasks. Conservative approaches may involve splinting and exercises to strengthen surrounding muscles. Immobilization of the DIP in full extension or 5–15 degrees of hyperextension is recommended. An aluminum splint can be applied, or a custom-made splint may be used. The metal ring splints are generally not recommended due to patient discomfort. In more severe cases or cases that are refractory to conservative measures, surgical intervention may be required. Given the high incidence of complications from mallet finger, referral to hand surgery is recommended.
Boutonniere deformity (A) involves flexion of the proximal interphalangeal (PIP) joint and hyperextension of the DIP, not hyperflexion of the DIP. This is the result of a rupture to the insertion of the extensor expansion into the base of the phalanx. Dupuytren contracture (B) is a progressive thickening of the palmar fascia of the hand, leading to contracture of the fingers. While post-traumatic arthritis (C) may be a common complication from any injury, it is not specific to injuries of the extensor tendon of the distal interphalangeal joint of the finger.
References
- Park CW, Juliano ML, Woodhall D. Tendon Lacerations. In: Knoop KJ, Stack LB, Storrow AB, Thurman R. eds. The Atlas of Emergency Medicine, 5e. McGraw Hill; 2021. Accessed June 24, 2023. https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=2969§ionid=250461424
- Dy CJ, Rosenblatt L, Lee SK. Current methods and biomechanics of extensor tendon repairs. Hand Clin. 2013;29(2):261-268. doi:10.1016/j.hcl.2013.02.008
- Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 2008;39(12):1338-1344. doi:10.1016/j.injury.2008.06.021
- Patillo D, Rayan GM. Open extensor tendon injuries: an epidemiologic study. Hand Surg. 2012;17(1):37-42. doi:10.1142/S0218810412500062
- Moore A, Stevens KA, Fallahi AKM, Marappa-Ganeshan R. Hand Extensor Tendon Lacerations. In: StatPearls. Treasure Island (FL): StatPearls Publishing; November 15, 2022.
- Amirtharajah M, Lattanza L. Open extensor tendon injuries. J Hand Surg Am. 2015;40(2):391-398. doi:10.1016/j.jhsa.2014.06.136
- Jones, O. The Extensor Tendon Compartments of the Wrist. Teach Me Anatomy. Dec 21, 2022. Accessed June 8, 2023. https://teachmeanatomy.info/upper-limb/areas/extensor-tendon-compartments-wrist/
- Tuncali D, Yavuz N, Terzioglu A, Aslan G. The rate of upper-extremity deep-structure injuries through small penetrating lacerations. Ann Plast Surg. 2005;55(2):146-148. doi:10.1097/01.sap.0000168884.88016.e1
- Rosh AJ, Kwon NS, Wilburn JM, et al. Extensor tendon repair. Medscape. Accessed June 6, 2023. https://emedicine.medscape.com/article/109111-overview
- Hile D, Hile L. The emergent evaluation and treatment of hand injuries. Emerg Med Clin North Am. 2015;33(2):397-408. doi:10.1016/j.emc.2014.12.009
- Bloom JMP, Khouri JS, Hammert WC. Current concepts in the evaluation and treatment of mallet finger injury. Plast Reconstr Surg. 2013;132(4):560e-566e. doi:10.1097/PRS.0b013e3182a0148c
- Zhao W, Wang G, Chen B, et al. The value of ultrasound for detecting hand fractures: A meta-analysis. Medicine (Baltimore). 2019;98(44):e17823. doi:10.1097/MD.0000000000017823
- Rosskopf AB, Martinoli C, Sconfienza LM, et al. Sonography of tendon pathology in the hand and wrist. J Ultrason. 2021;21(87):e306-e317. doi:10.15557/JoU.2021.0052
- Emergency Department Management of Extensor Tendon Lacerations – Page 3 of 4. ACEP Now. Accessed June 7, 2023. https://www.acepnow.com/article/emergency-department-management-of-extensor-tendon-lacerations
- Griffin M, Hindocha S, Jordan D, et al. Management of extensor tendon injuries. Open Orthop J. 2012;6:36-42.
- Grossman JAI, Adams JP, Kunec J. Prophylactic Antibiotics in Simple Hand Lacerations. 1981;245(10):1055–1056. doi:10.1001/jama.1981.03310350043021
- Roberts AH, Teddy PJ. A prospective trial of prophylactic antibiotics in hand lacerations. Br J Surg. 1977;64(6):394-396. doi:10.1002/bjs.1800640605
- Haughey RE, Lammers RL, Wagner DK. Use of antibiotics in the initial management of soft tissue hand wounds. Ann Emerg Med. 1981;10(4):187-192. doi:10.1016/s0196-0644(81)80159-x
- Levine BJ. Open Fracture. In: EMRA Antibiotic Guide. Emergency Medicine Residents’ Association; 2022:10-11.
- Calabro J, Hoidal CR, Susini LM. Extensor tendon repair in the emergency department. J Emerg Med. 1986;4:217-225. Hanz KR, Saint-Cyr M, Semmler MJ, et al.
- Anderson D. Mallet finger—management and patient compliance. Aust Fam Physician. 2011;40:47-48.
- Johnson SP, Kelley BP, Waljee JF, Chung KC. Effect of Time to Hand Therapy following Zone II Flexor Tendon Repair. Plast Reconstr Surg Glob Open. 2020;8(12):e3278. Published 2020 Dec 21. doi:10.1097/GOX.0000000000003278
- Carl HD, Forst R, Schaller P. Results of primary extensor tendon repair in relation to the zone of injury and pre-operative outcome estimation. Arch Orthop Trauma Surg. 2007;127:115-119.
- Chapter 11: Hand. In: Simon RR, Sherman SC, eds. Emergency Orthopedics. 6th ed. New York, NY: McGraw-Hill Medical; 2011:207-211.
- Lin B. Extensor Tendon Lacerations, Part III. Closing the Gap. July 11, 2016. Accessed June 9, 2023. https://lacerationrepair.com/techniques/special-situations/extensor-tendon-lacerations-part-iii/.
- Centers for Disease Control and Prevention. Tetanus: For Clinicians. Centers for Disease Control and Prevention. August 29, 2022. Accessed June 7, 2023.https://www.cdc.gov/tetanus/clinicians.html
- Roberts, James R. MD. ED Treatment of Flexor Tendon Injuries. Emergency Medicine News 33(12):p 8,9, December 2011. | DOI: 10.1097/01.EEM.0000410106.40227.cc





{kind=link}
{kind=link}