Today on the emDOCs cast with Brit Long, MD (@long_brit), we cover a significant biliary pathology: cholangitis.
Episode 52: Cholangitis
Background:
- Defined by presence of increased hepatic intraductal pressure with a concurrent infection of the obstructed bile.
- ‘Ascending’ refers to the migration of bacteria from the duodenum into the hepatopancreatic duct, which can then spread to the bloodstream.
- 15% of the U.S. has gallstones, 2-3% of these patients will develop a complication from these stones, like cholangitis. 9% of patients admitted due to gallstone disease have cholangitis.
- Cholangitis can quickly progress to septic shock.
- Mortality approaches 100% if untreated. Even with appropriate diagnosis and therapy in the current era, mortality remains high (2-30%).
Etiology:
- There are a variety of causes. The most common causes are bile duct stones and previous manipulation of the biliary tree (biliary calculi (28-79%), benign biliary stricture (5-28%), and malignancy (10-57%), ERCP (<2%), primary sclerosing cholangitis.
- Acalculous cholangitis (absence of bile duct stone or obstructive malignancy) usually occurs in severely ill patients.
- Special scenarios:
- Lemmel Syndrome – extrinsic compression of the bile duct due to a duodenal periampullary diverticulum.
- Inflammation due to pancreatitis.
- Mirizzi syndrome – impacted stone in the cystic duct or neck of the gallbladder.
- Intrinsic obstruction – thrombosis, parasitic infection.
Pathophysiology:
- In cholangitis, the infection is not just limited to the gallbladder (e.g., cholecystitis where the disease is contained), but the biliary system, which can spread to the blood (thus, not contained).
- Two factors in cholangitis: Biliary obstruction and bacterial growth in the bile which can spread to the bloodstream. This is the cause of rapid progression to septic shock.
- Bile is typically sterile. In cholangitis, biliary obstruction creates a nidus for colonization and infection. Bacteria can ascend the biliary tree from the duodenum. Cholangiovenous reflux results in positive blood cultures in 70%.
History and Exam:
- History and exam are not always straightforward; patients may present with a variety of signs/symptoms, including altered mental status or sepsis with unknown source.
- Charcot’s triad of fever, right upper quadrant pain, and jaundice has a specificity of 85% and sensitivity of 25%.
- Reynold’s pentad is Charcot’s triad plus hypotension and altered mental status, which has a sensitivity of < 7%.
- Fever in 40-100%, abdominal pain in 60-100%, but these are not specific.
- Jaundice is present in 60-70%.
- May have other systemic symptoms like rigors, chills.
- May present with complications from bacteremia (shock, hepatic abscess).
Laboratory Evaluation:
- AST/ALT typically elevated, but degree of elevation varies.
- GGT and alkaline phosphatase elevated in close to 90%; bilirubin may be over 4 mg/dL.
- Elevated WBC in 80%. Neutrophil to lymphocyte ratio is often > 5.
- Blood cultures positive in 70%.
Imaging:
- Several options: US, CT, ERCP, MRCP.
- US can identify dilated intrahepatic ducts, as well as a dilated common bile duct to indicate common bile duct stone or other distal obstruction.
- Transabdominal US is approximately 38-91% sensitive for diagnosing common bile duct dilation and 25-60% sensitive for the detection of common bile duct stones. It is highly specific.
- CBD > 7 mm is dilated, but in those with prior cholecystectomy the dilation can be up to 10 mm. CBD may be normal early in the disease course.
- CT with IV contrast can identify dilated intrahepatic and common bile ducts and may also identify a nearby mass causing external compression on the biliary structures.
- Multidetector CT with IV contrast demonstrates a sensitivity of 85-97% and specificity of 88-96% in the identification of biliary duct dilation and strictures. CT can also evaluate for complications.
- MRCP is used if high diagnostic suspicion but inconclusive or negative CT/US.
Diagnosis:
- The Tokyo Guidelines have undergone several iterations. The most recent version was published in 2018. High density and specificity.
- Three diagnostic components for diagnosis (if two present, probable diagnosis; if three present; definitive diagnosis): systemic inflammation (fever/rigors or evidence of inflammatory response on laboratory evaluation), cholestasis (jaundice or abnormal liver function tests), and imaging (biliary dilatation or imaging evidence of etiology of obstruction) (Table 1).
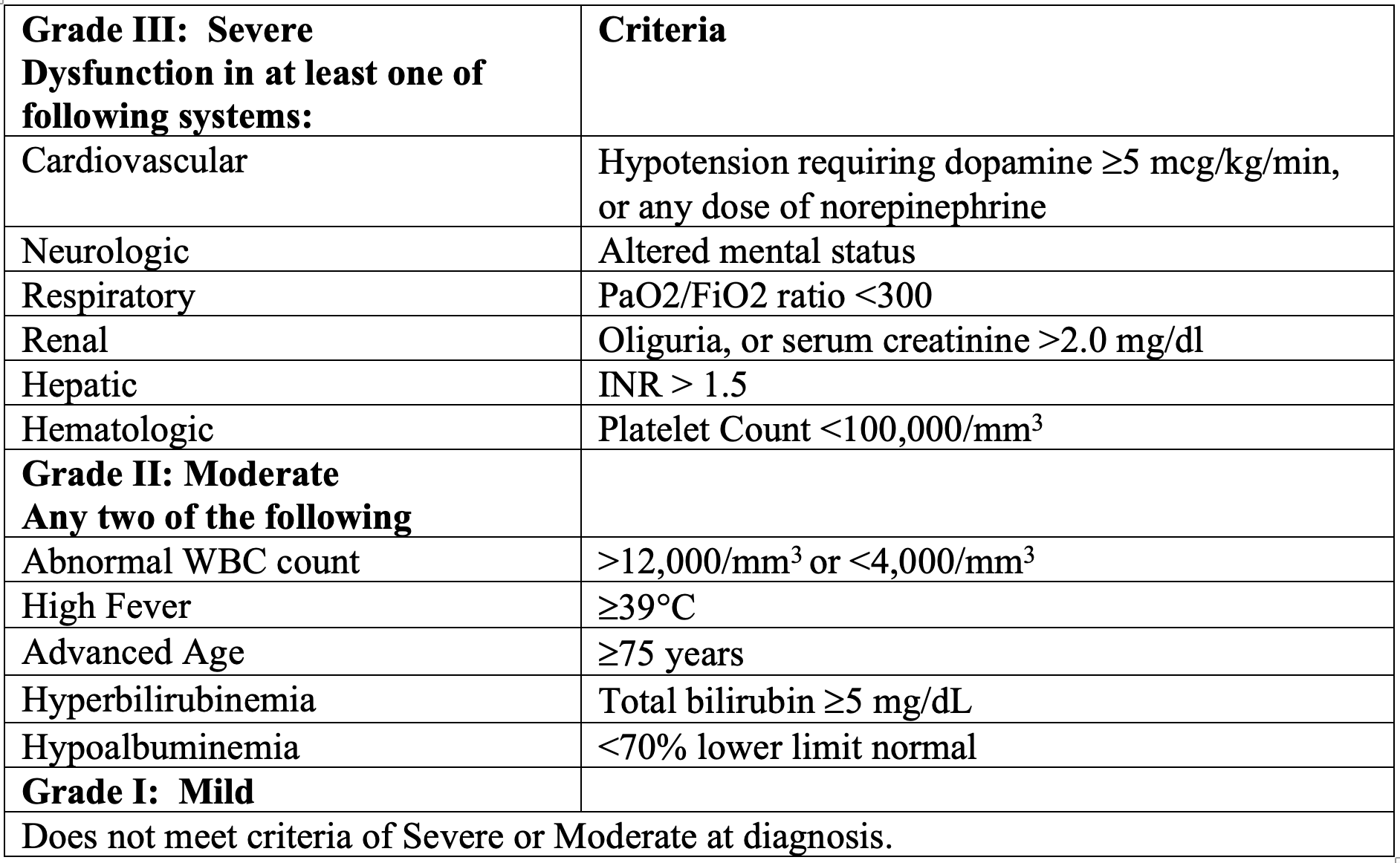
- Broken into grades based on severity (Table 2).
Table 1 – TG18 Diagnostic Criteria for Acute Cholangitis.
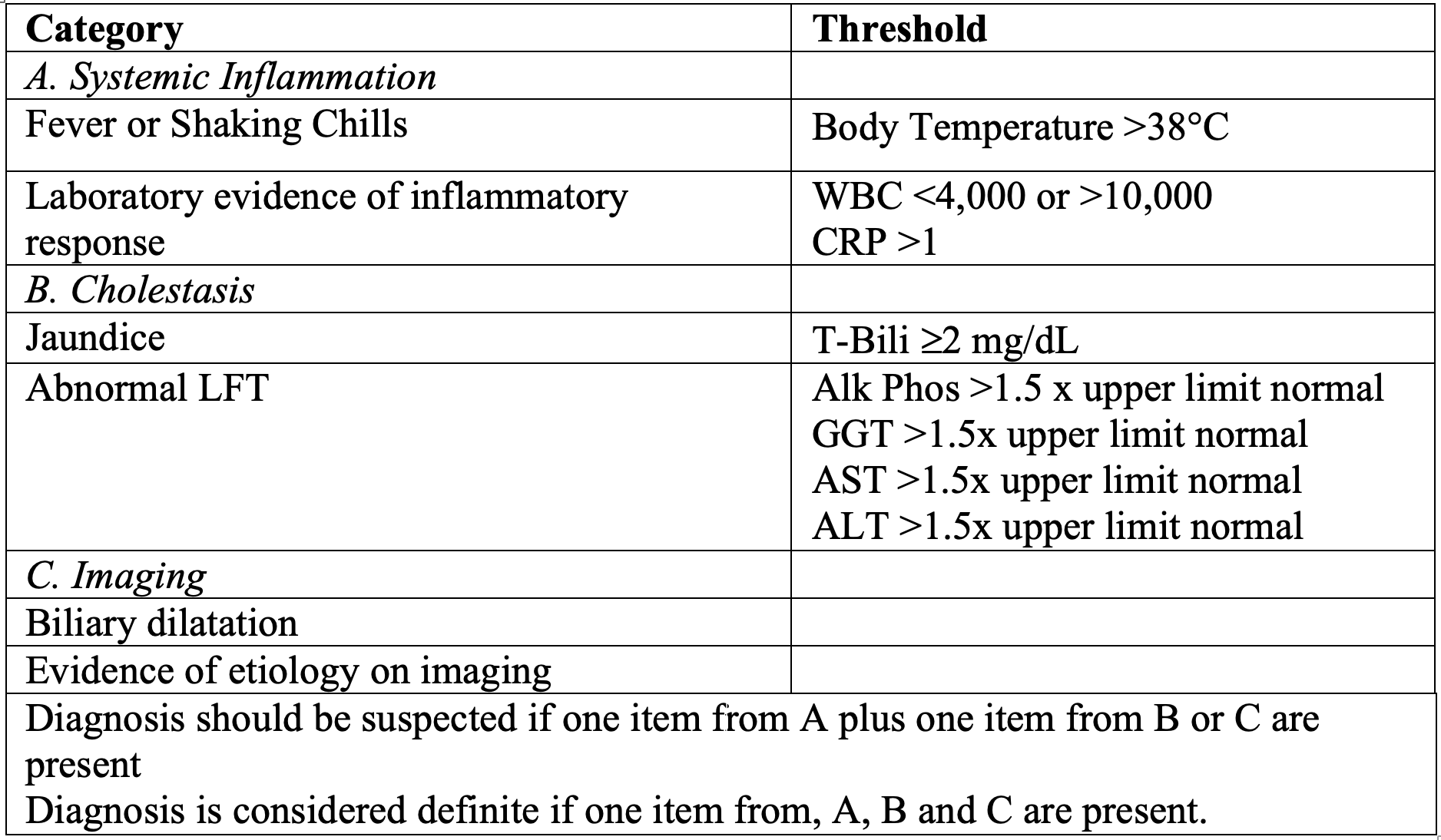
Table 2 – TG18 Severity Criteria for Acute Cholangitis
Treatment:
- Broad spectrum antibiotics, resuscitation (fluids, vasopressors), symptomatic therapy (analgesics, anti-emetics), and consultation.
- Consult GI in all patients for decompression with ERCP. Surgery should also be consulted if the patient is toxic with end organ injury.
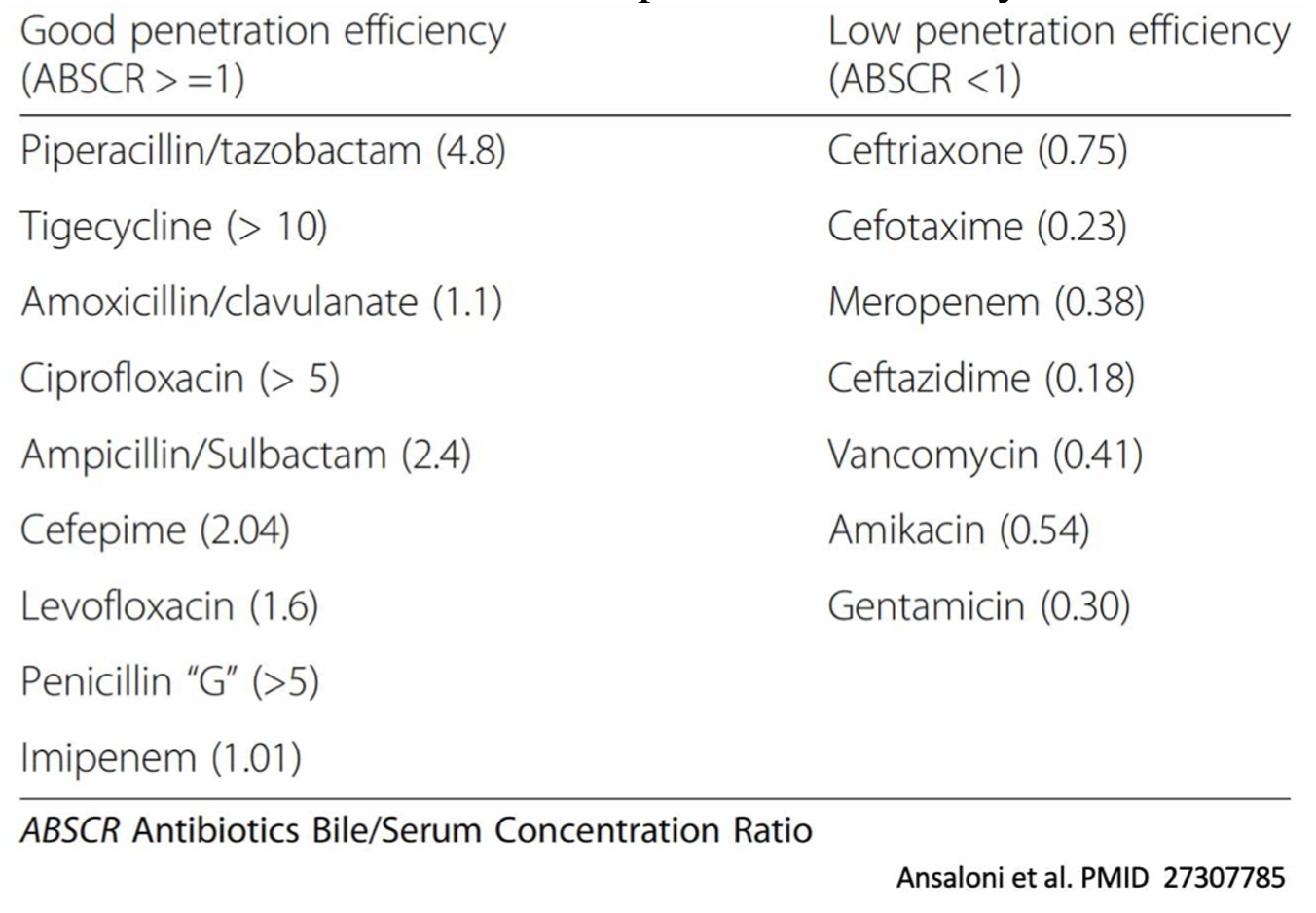
- Antibiotics should cover enteric streptococci, coliforms, and anaerobes. No solid evidence for using antibiotics with high biliary penetration, but still must be considered in cholangitis. Vancomycin is needed in very few patients with cholangitis.
- Not sick: Piperacillin/tazobactam or ertapenem OR metronidazole PLUS cefazolin or cefuroxime or ceftriaxone or cefotaxime or ciprofloxacin or levofloxacin.
- Sick: Piperacillin/tazobactam, meropenem, impenem-cilastatin OR metronidazole PLUS cefepime or ceftazidime.
- Healthcare associated: Add ampicillin or vancomycin.
- Disease grading can assist with treatment decisions and timing of treatment. Grade III patients benefit from near-immediate/emergent decompression, Grade II emergent/early decompression, Grade I may require only medical management or delayed surgical intervention to relieve obstruction.
- 70-80% of patients with mild cholangitis improve with antibiotics and can undergo drainage in 24-48 hours. If they don’t respond in first 24 hours, they should undergo decompression.
- Delayed biliary decompression after failure of medical therapy carries a mortality rate up to 80%. Delayed ERCP beyond 24-48 hours has been associated with prolonged hospital stay, increased risk of death, increased need for vasopressor support, persistent organ failure, and increased ICU length of stay.
- ERCP is successful in > 90%.
- ERCP has lower morbidity and mortality compared to open surgical biliary decompression in those patients with severe cholangitis, but this benefit is blunted in the elderly population.
- Percutaneous drainage of the gallbladder or biliary tree remains an option when ERCP is unsuccessful or if not feasible (Roux-en-Y anastomosis or Whipple resection or duodenal narrowing).
- Surgical drainage is the final option when other treatments have failed.
- Admit patients with confirmed/suspected cholangitis.
Summary:
- Cholangitis is due to CBD obstruction and bacterial infection. It can be associated with high mortality.
- Don’t rely on Charcot’s triad or Reynold’s pentad. Think about cholangitis in patients with rigors, abdominal pain, jaundice, and/or toxic appearance. Also think about the disease in the older patient with sepsis without a source who’s toxic/altered.
- Labs may reveal elevated WBC, LFTs. Blood cultures positive in 70%.
- Imaging includes US and CT with IV contrast (higher sensitivity).
- Tokyo guidelines can assist in diagnosis and management.
- For the emergency physician, the most important factors are suspecting the disease, resuscitating, providing antibiotics, and recognizing those patients who require emergent surgical or GI evaluation in order to improve outcome in moderate or severe disease.




