Today on the emDOCs cast with Brit Long, MD (@long_brit), and Rachel Bridwell, MD (@rebridwell), we cover two more challenging cases.
Episode 86: Tricky Cases Part 2
Case 3:
- 56-year-old female with history of seizures, actively seizing, EMS called. Patient seized for approximately 20 minutes prior to EMS arrival. They administer two doses of 10 mg midazolam IM. After second dose the tonic clonic movement stop; GCS is 3, and she’s unresponsive.
- On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Concern for nonconvulsive status epilepticus (NCSE).
- Two forms of status epilepticus (SE): convulsive and nonconvulsive
- Nonconvulsive SE: Change in cognitive or mental processes with no cmajor/significant convulsive activity AND…
- Electrographic abnormalities on EEG for at least 10 continuous minutes, or there’s intermittent seizure activity for over 20% of an hour on EEG OR
- EEG abnormalities plus clinical manifestations
- NCSE is a difficult diagnosis:
- Usually presents with AMS and no readily apparent motor activity
- No complete agreement on diagnostic criteria
- Official diagnosis requires EEG, which most of us do not have in the ED, and EEG is not 100% specific.
- NCSE accounts for almost 47% of all cases of status epilepticus.
- Causes: Inadequately treated convulsive status, acute brain injury or structural lesion, infection, encephalopathy, medications/toxins
- Underlying cause is the most important factor in morbidity and mortality.
- NCSE presents with subtle signs/symptoms: ocular abnormalities (gaze deviation, nystagmus, eyelid twitching), change in speech, lip smacking, motor twitches of face or distal extremities.
- Negative findings: phasia, mutism, amnesia and catatonia
- Positive findings: rhythmic twitching of one or more muscle groups, tonic eye deviation, hippus, or nystagmoid eye jerking
- Ocular abnormalities have 85% specificity
- Think NCSE in patients with these signs/symptoms, those with a history of seizures/epilepsy, intracranial pathology and AMS, prolonged post ictal status, and AMS with no other explanation despite testing.
- Look for life threats, check a serum glucose, and obtain neuroimaging.
- Treatment includes benzodiazepines.
- If patient improves with benzo’s, that can be diagnostic.
- Have a low threshold to administer a second line ant-epileptic, and be ready for sedation with propofol/ketamine and intubation.
- Patient had received midazolam, but with concern for NCSE, decision made to administer ketamine and propofol. Levetiracetam also administered.
- Challenging airway: BMI > 40, kyphotic, short neck.
- Airway: Must have an approach, be prepared, and have backups.
- Our plan: 1) Video with hyperangulated blade, 2) direct standard geometry blade with bougie, 3) cricothyrotomy. Video with standard blade and flexible intubating endoscope unavailable at location.
- Airway plan discussed with resuscitation team. Cric is progression of the airway plan; it is not a failure.
- First attempt with hyperangulated blade. While second attempt ongoing, neck prepped and marked for cric.
- Second attempt with DL and bougie successful; ETT position confirmed with US. Propofol utilized for sedation; patient admitted to ICU for EEG monitoring. CT demonstrated no acute, actionable findings.
Learning points:
- Have an approach to seizures/status epilepticus: first dose benzo, but while asking for the second dose and other agent, prepare for intubation with ketamine and/or propofol.
- NCSE is likely more common than we think.
- Consider NCSE in patients with altered mental status and abnormal ocular movements, lip smacking or subtle twitches in the face or extremities, and those with a history of seizures/epilepsy or a medication history on an anti-epileptic. Also think about NCSE in patients with prior cerebral pathology (ie, ischemic stroke); a patient who was seizing, was treated, and is not coming out of their post ictal state; and in patients with unexplained altered mental status with no other cause.
- Official diagnosis requires EEG, which is not something we can typically obtain in the ED.
- Check glucose, obtain imaging, stop the seizure.
- Every airway requires a plan and backups. Cric is not a failure; it is an integral part of every airway plan.
Reference:
Case 4:
- 52-year-0ld male brought in by EMS with “code STEMI”. ECG demonstrates ST depressions with rocket like T waves in V2-V4.
- American College of Cardiology released a new consensus statement, “Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee“. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
- STEMI vs. NSTEMI dichotomy is not sensitive for true occlusion MI or acute coronary occlusion.
- “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant miry of patients who have acute coronary occlusion.”
- “In the absence of ischemic ST-segment elevation, the ECG should be examined for other changes that have been associated with coronary artery occlusion; when present, these should prompt evaluation for emergent coronary angiography.”
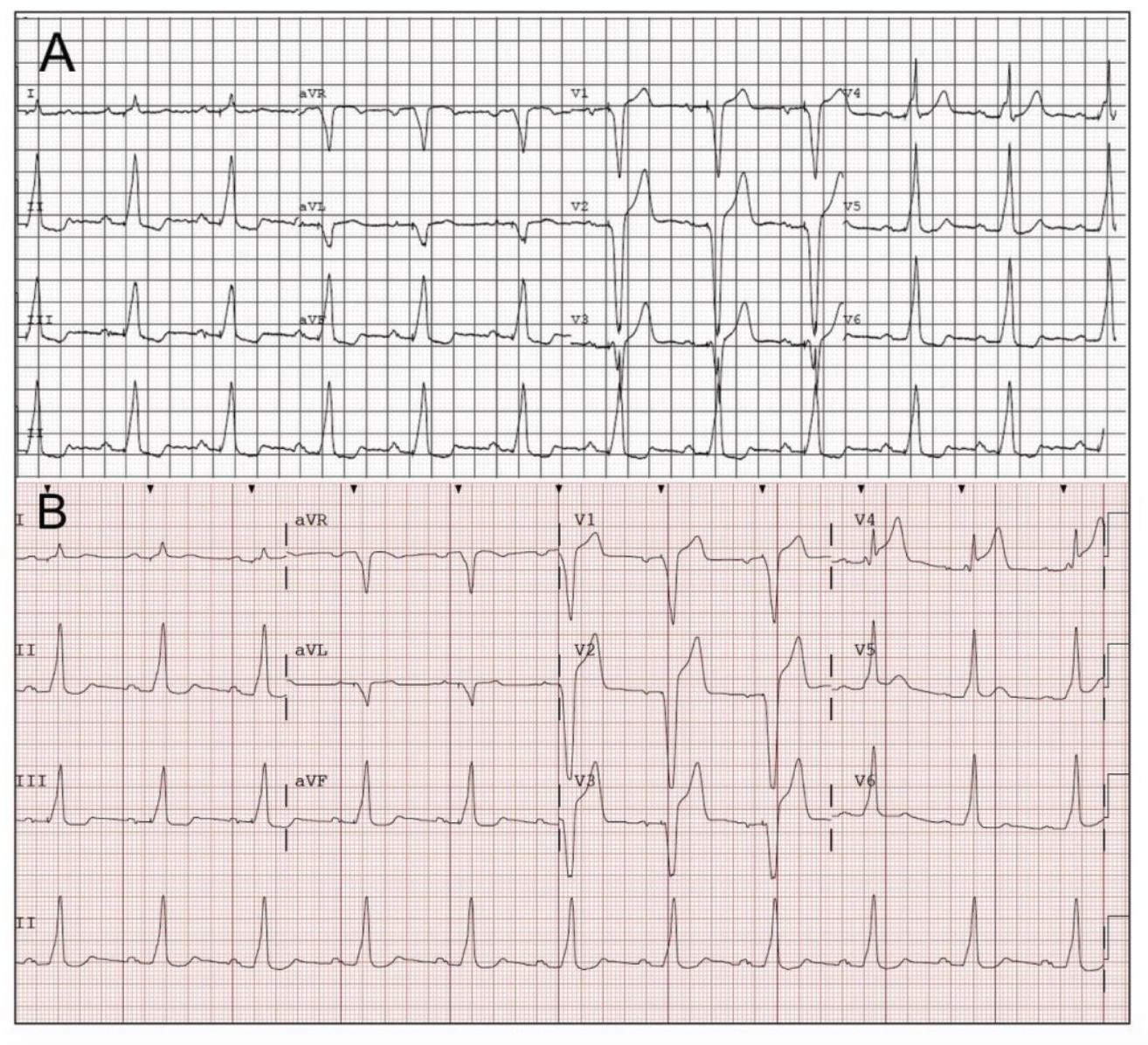
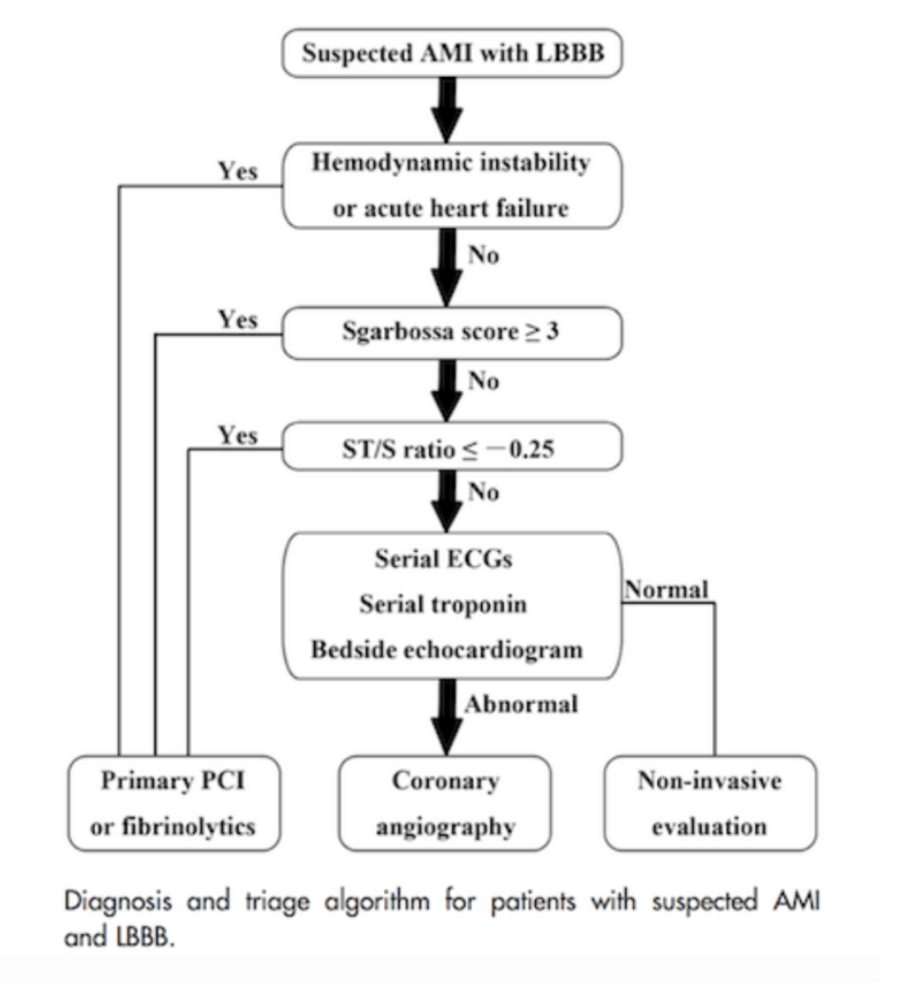
- LBBB or ventricular paced rhythm with Sgarbossa or Smith-modified Sgarbossa criteria
- Posterior STEMI
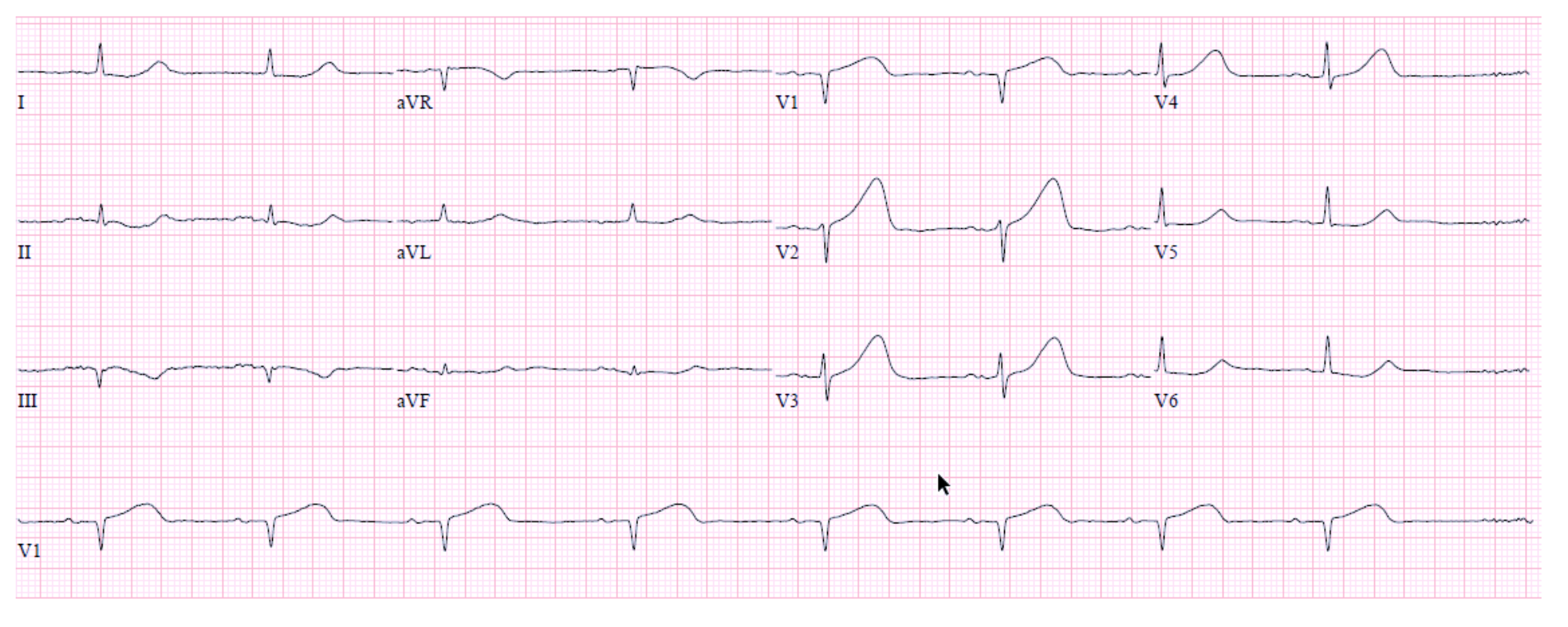
- Hyperacute T waves
- DeWinter T waves
- LBBB/ventricular paced rhythm with Sgarbossa or Smith-modified Sgarbossa criteria
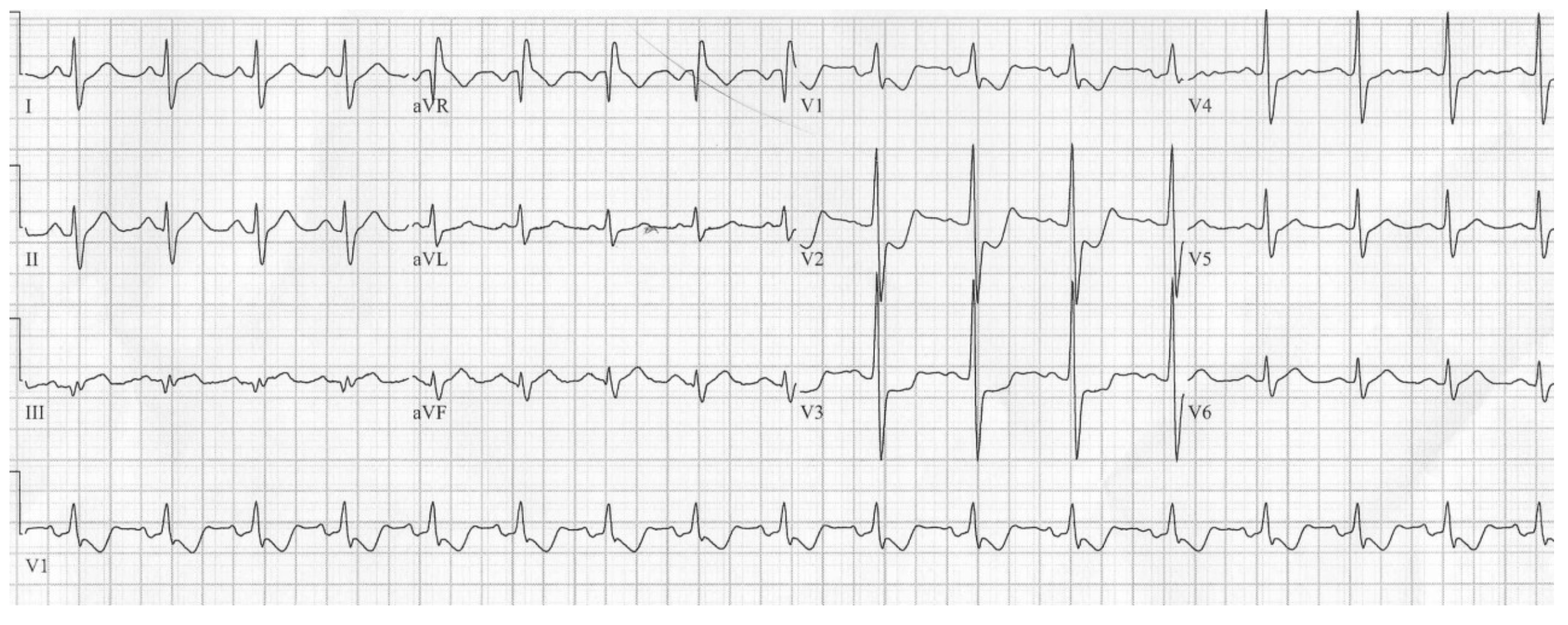
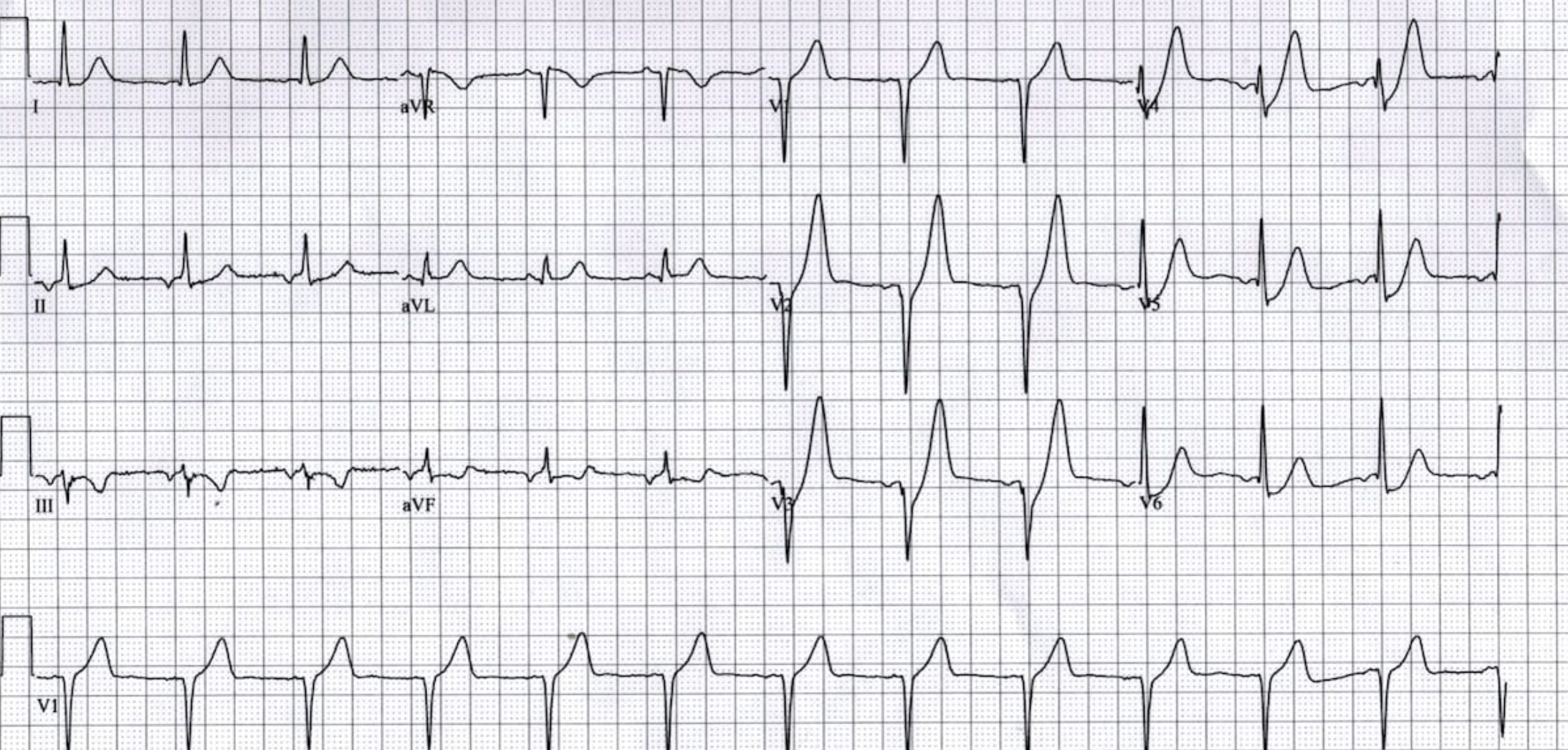
- Cardiology consulted; patient taken to cath lab, 100% proximal LAD occlusion.





