
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University in St. Louis); Jessica Pelletier, DO (EM Attending Physician, Washington University in St. Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
You are working in the trauma/critical care pod of your emergency department (ED). You receive a page for a cardiac arrest and take report from emergency medical services (EMS). A bystander called EMS after they saw a man unresponsive on a sidewalk near a parked car. It is unclear how long he was down. Per EMS he was very cold to touch. His blood sugar was normal en route to the ED, and his initial rhythm on the cardiac monitor was asystole. The patient received 1 mg of epinephrine IV x2 with conversion of his rhythm to ventricular fibrillation (VF) for which he was defibrillated twice in the field. He arrives at the ED with a laryngeal mask airway (LMA) in place with waveform end tidal CO2 of approximately 20 mmHg. The patient is actively receiving chest compressions with a LUCAS automated compression device.
What would your next steps be?
The patient is moved over to the stretcher and connected to the monitors and defibrillator. He is unresponsive and continues to be in VF, for which he receives a dose of amiodarone and is defibrillated twice more. However, the VF is refractory and does not convert to sinus rhythm. A temperature sensing Foley catheter is placed which reveals a temperature of 25℃.
What would you do next?
The patient is covered with warm blankets and warmed intravenous (IV) fluids are administered at 39℃ at a gentle bolus rate via a Belmont transfuser. Cardiac surgery is immediately paged for consideration of veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) for active rewarming. His LMA is exchanged for an endotracheal tube without induction or paralytic agents. A right femoral arterial line and triple lumen catheter are placed. His point-of-care labs return with a potassium of 3.4 mEq/L. Cardiac surgery cannulates him onto VA ECMO for active rewarming. The patient is rewarmed to 30℃ on the ECMO circuit and at this point is successfully defibrillated out of VF into what appears to be a wide-complex bradycardia. The patient begins to blink and make purposeful movements, at which point he is started on sedation for comfort and safety. He requires low-dose epinephrine to maintain his mean arterial pressure (MAP) in the 60s mmHg and is transported to the cardiothoracic (CT) ICU. The patient is extubated and decannulated four days later. He subsequently walks out of the hospital with a normal neurologic exam two weeks after admission.
Hypothermic Arrest
In general, hypothermic patients in cardiac arrest should be aggressively resuscitated. Patients can have excellent outcomes despite prolonged resuscitation.1,2 Some exceptions are patients with unsurvivable traumatic injuries, frozen chest wall to the point where compressions cannot be performed, or if there is snow or ice occluding the airway and suffocation is the suspected primary cause of cardiac arrest.2,3 If the patient meets criteria for resuscitation, they generally are not declared dead until their core temperature is above 32℃ (“warm and dead”).3,4 As always, the decision to end the resuscitation should be based on several other factors, but 32℃ would be the minimum temperature achieved before the decision is made to end the resuscitation.
Some authors recommend not starting chest compressions in hypothermia unless there is no organized cardiac activity (e.g., VF/asystole), a pulse cannot be identified via Doppler ultrasound for a full minute, or if lack of organized cardiac activity is confirmed on bedside echocardiogram.2 In reality you may start compressions before you confirm that hypothermia was the primary cause of cardiac arrest. It can be very challenging to palpate pulses in hypothermic arrests (even more so than other arrests) due to vasoconstriction. This is a good time to utilize an arterial line or use the ultrasound to find a central pulse.
Obtaining a core temperature early in any arrest suspected to be from hypothermia is key. This should be accomplished via a rectal, esophageal, or Foley temperature probe. Rectal temperature is challenging to obtain in patients who are receiving chest compressions, and bladder temperatures can be unreliable; thus, esophageal temperature is preferred.2Esophageal and bladder temperatures can also be continuously monitored which is essential in hypothermic cardiac arrest.
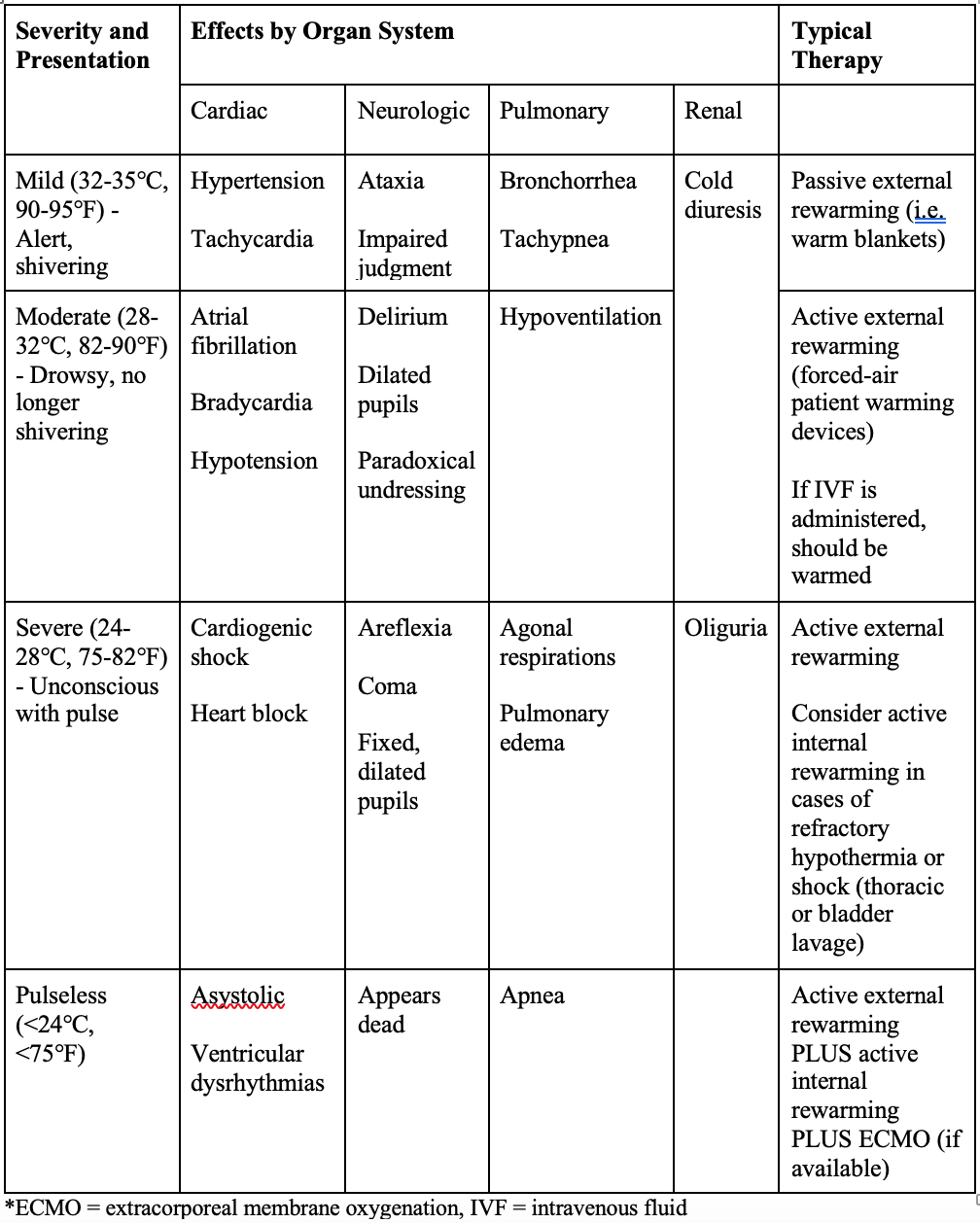
Be careful with excessive medication administration. This is a bit controversial, but it is prudent to avoid excessive doses of ACLS drugs until the patient is rewarmed. This is because medications will accumulate and may only fully metabolize once the patient is normothermic. It is worth attempting defibrillation at any temperature, though success is unlikely until the patient’s core temperature is > 30℃.2 After rewarming to approximately 30℃ you can generally proceed with standard ACLS techniques including medications. Obtaining a core temperature and evaluating for clinical effects of hypothermia by organ system is essential when managing hypothermic patients (Table 1).
Table 1. Classification of hypothermia. Modified from: https://emcrit.org/ibcc/hypothermia/
Some institutions have ECMO (relatively) readily available. This is an optimal means of management for patients who are pulseless from suspected hypothermic arrest.5,6,7 This can allow warming at up to 10℃ an hour and improves organ perfusion. Generally, VA-ECMO is considered for patients without major traumatic injuries with a core temperature <30℃, without severe comorbidities that would make the resuscitation futile, and who have a favorable HOPE score (https://www.hypothermiascore.org/).10,11 The HOPE score was developed as part of an international collaboration led by a Swiss Emergency Medicine group.10 The score predicts the probability of survival to hospital discharge using a number of factors including CPR duration, serum potassium, core temperature, age, and suspected mechanism of hypothermia. Our patient’s HOPE Score estimated he had a 78% chance of survival to hospital discharge.
Hypothermic arrest differs from cardiac arrest from other causes. Down time and time doing CPR is not nearly as important, and even patients with low end tidal, fixed, dilated pupils, asystole rhythm, and extended low-flow times can have favorable neurologic outcomes.2,11 There are cases of patients recovering after hours of time without a pulse with good CPR.12 Classically, serum potassium has been used as a prognostic marker. However, hemolysis can cause falsely elevated levels and there are reports of patients surviving with significant hyperkalemia on initial labs.13,14 It is recommended that potassium be used as part of the HOPE score rather than in isolation.10 However, a potassium >12 mEq/L carries a poor prognosis as there do not appear to be any known case reports of patients in hypothermic arrest surviving with a potassium this high.
Other options if ECMO is not available include thoracic lavage and bladder lavage. Thoracic lavage is traditionally performed with two chest tubes on each side of the chest, though one can be used. An anterior chest tube, which is an uncommon procedure in the ED, is usually used in addition to the standard lateral chest tube, but two lateral chest tubes may be used. The more anterior chest tube can be connected to the Belmont in order to infuse warm fluids into the chest and then drained from the more lateral tube.5,15,16 Theoretically this can warm at approximately 4-5℃/hour. Similarly, the peritoneum can be warmed using warmed saline. If the patient already has a peritoneal dialysis catheter, this can be used, otherwise a technique similar to a diagnostic peritoneal lavage is utilized to access the peritoneum.15,16 If available, general surgery can be consulted for assistance with this technique. For bladder lavage the Belmont can be used to place approximately 300 mL into the bladder, allow this to percolate for 15 minutes, drain it, and repeat as needed. It is best to use a three-way irrigation Foley if possible. For warmed IV fluids, the Belmont can be used but generally the fluid administration rates will be much lower than for sick trauma patients. For intubated patients, the ventilator can be set to deliver humidified air and assist in rewarming.14
These patients will often have a significant amount of “cold diuresis” leading to intravascular hypovolemia; thus, infusion of warm IV fluids is essential with the rate dependent on the patient’s volume status and cardiac/renal function. Avoid supradiaphragmatic central lines in these patients as any guidewire contact with the sensitive hypothermic myocardium can cause them to go back into VF.17
It is crucial to figure out why the patient is hypothermic and reverse the underlying cause if possible. In our case, the patient had accidentally overdosed on drugs prior to being found. However, consideration of infection, endocrine shock (adrenal, thyroid disease), electrolyte abnormalities, hypoglycemia or central nervous system (CNS) disasters is important. If your altered patient is mildly hypothermic and their mental status is not improving, consider other conditions.
Pearls and Pitfalls:
- Check a core temperature early in any cardiac arrest (esophageal is preferred).
- Rule out reversible causes of hypothermia (such as hypoglycemia) early in the resuscitation.
- Avoid excessive utilization of ACLS medications until the patient has been warmed to >30℃ due to the risk of drug accumulation.
- Patients with a hypothermic arrest require aggressive rewarming and generally are not declared dead until warmed above 32℃.
- Consider ECMO early on in the resuscitation for active rewarming; otherwise, use non-invasive and invasive rewarming strategies.
- If your patient is warming up but still unstable or altered, consider infectious or endocrine causes for their presentation.
For more information, please check out this excellent prior post on Hypothermia and Drowning Pearls: https://www.emdocs.net/hypothermia-and-drowning-pearls/
For more hypothermia cases, please visit the following EM@3AM links:
References:
- Headdon WG, Wilson PM, Dalton HR. The management of accidental hypothermia. BMJ. 2009;338:b2085. Published 2009 Jun 10. doi:10.1136/bmj.b2085.
- Carsten L, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation. 2021.
- Brown DJ, Brugger H, Boyd J, Paal P. Accidental hypothermia [published correction appears in N Engl J Med. 2013 Jan 24;368(4):394]. N Engl J Med. 2012;367(20):1930-1938. doi:10.1056/NEJMra1114208
- Weinberg AD. Hypothermia. Ann Emerg Med. 1993;22(2 Pt 2):370-377. doi:10.1016/s0196-0644(05)80467-6
- Farkas J. Hypothermia – EMCRIT Project. EMCrit Project. https://emcrit.org/ibcc/hypothermia/. Published February 12, 2023. Accessed September 30, 2023.
- Mathieu Pasquier, Peter Paal, Marc Blancher, Tomasz Darocha. Higher Survival Chances of Hypothermic vs. Normothermic cardiac arrest patients with ECLS re-warming, Resuscitation, Volume 134, 2019, Pages 161-162, ISSN 0300-9572. doi.org/10.1016/j.resuscitation.2018.11.004
- ELSO: Ultrasound Guidance for Extracorporeal Membrane Oxygenation Veno-Arterial ECMO Specific Guidelines. Available from: elso_ultrasoundguidance_vaecmo_guidelines_may2015.pdf. Accessed December 4, 2022
- Swol, Justyna; Darocha, Tomasz; Paal, Peter; Brugger, Hermann; Podsiadło, Paweł; Kosiński, Sylweriusz; Puślecki, Mateusz; Ligowski, Marcin; Pasquier, Mathieu. Extracorporeal Life Support in Accidental Hypothermia with Cardiac Arrest—A Narrative Review. ASAIO Journal: February 2022 – Volume 68 – Issue 2 – p 153-162. doi: 10.1097/MAT.0000000000001518
- Zafren K, Mechem C. UpToDate. UpToDate. https://www.uptodate.com/contents/accidental-hypothermia-in-adults?search=hypothermia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Published April 13, 2023. Accessed September 30, 2023.
- Pasquier M, Hugli O, Paal P, Darocha T, Blancher M, Husby P, Silfvast T, Carron PN, Rousson V. Hypothermia outcome prediction after extracorporeal life support for hypothermic cardiac arrest patients: The HOPE score. Resuscitation 2018.
- Monika BM, Martin D, Balthasar E, et al. The Bernese Hypothermia Algorithm: a consensus paper on in-hospital decision-making and treatment of patients in hypothermic cardiac arrest at an alpine level 1 trauma centre. Injury. 2011;42(5):539-543. Doi:10.1016/j.injury.2010.11.037.
- Forti A, Brugnaro P, Rauch S, et al. Hypothermic Cardiac Arrest With Full Neurologic Recovery After Approximately Nine Hours of Cardiopulmonary Resuscitation: Management and Possible Complications. Ann Emerg Med. 2019;73(1):52-57. doi:10.1016/j.annemergmed.2018.09.018
- Romlin BS, Winberg H, Janson M, et al. Excellent Outcome With Extracorporeal Membrane Oxygenation After Accidental Profound Hypothermia (13.8°C) and Drowning. Crit Care Med. 2015;43(11):e521-e525. doi:10.1097/CCM.0000000000001283
- Dobson JA, Burgess JJ. Resuscitation of severe hypothermia by extracorporeal rewarming in a child. J Trauma. 1996;40(3):483-485. doi:10.1097/00005373-199603000-00032
- Danzl DF, Pozos RS. Accidental hypothermia. N Engl J Med. 1994;331(26):1756-1760. doi:10.1056/NEJM199412293312607.
- Klein LR, Huelster J, Adil U, et al. Endovascular rewarming in the emergency department for moderate to severe accidental hypothermia. Am J Emerg Med. 2017;35(11):1624-1629. doi:10.1016/j.ajem.2017.05.001
- Paal P, Pasquier M, Darocha T, et al. Accidental Hypothermia: 2021 Update. Int J Environ Res Public Health. 2022;19(1):501. Published 2022 Jan 3. doi:10.3390/ijerph19010501





1 thought on “Hypothermic Cardiac Arrest: Pearls and Pitfalls”
Pingback: LITFL Update 022 • LITFL • Newsletter