
Anand Swaminathan, MD, MPH (@EMSwami) is an assistant professor and assistant program director at the NYU/Bellevue Department of Emergency Medicine in New York City.
Background
There are a number of myths that have been purported over time in regards to intravenous contrast for CT scans. These myths have passed from unfounded statements to well-accepted dogma. Here, we attempt to look at the evidence behind two of these myths, where evidence exists, in order to change clinical practice to benefit patients.
Myth #1 – Patients with shellfish allergies cannot safely receive intravenous contrast because they are allergic to the iodine in both of these substances.
We frequently see patients who report a shellfish allergy and/or iodine allergy in triage. In the cases where these patients need CT scans with contrast performed, we are often told by radiology (or by the patient) that they cannot get contrast because of their allergy. But is there actually any truth to this?
The short answer is no. There is no such thing as an iodine allergy. Iodine is found throughout our bodies in thyroid hormones. In addition, almost all salt in the United States has iodine added to it in order to avoid iodine deficiency.
What about the second part of the myth? Can patients with shellfish allergy get IV contrast? The answer here is clearly yes. While it’s true that patients can have allergies to shellfish and shellfish contain iodine, the actual allergens are two proteins: tropomyosins and parvalbumin. So there’s no direct relationship between shellfish and contrast allergies. In fact, the American College of Radiology (ACR) Manual on Contrast Media1 clearly states:
“A significant number of healthcare providers continue to inquire specifically into a patient’s history of “allergy” to seafood, especially shellfish. There is no evidence to support the continuation of this practice.” 2-3
Bottom Line: Based on the literature that’s available, as well as the professional recommendations from the ACR, medical personnel should stop asking patients about shellfish allergies. Even if the question is asked, we should all be clear that there’s no relationship between a shellfish allergy and an IV contrast allergy.
One caveat to this is that patients who have a history of a severe allergic reaction to any medication have an increased risk of having a severe allergic reaction to any other medication you give them.4
Myth #2: Pretreatment is necessary prior to IV contrast in all patients with history of allergic reactions to medications and reduces the risk of anaphylactoid reaction to contrast.
The first point that needs clarification is that the reaction to contrast is an anaphylactoid reaction, not an anaphylactic one. This is important because while these two reactions manifest with similar symptoms and signs, the pathophysiology is very different. In an anaphylactic reaction, a patient is exposed to an allergen and the body’s immune system creates antibodies to this allergen. Upon repeat exposure, the antibodies and antigens form complexes leading to degranulation of mast cells and histamine release. In anaphylactoid reactions, primary exposure to a substance causes histamine release without the involvement of antibodies.
So, now that the definitions are clear, let’s delve into the literature on pretreatment with corticosteroids to prevent IV contrast reactions.
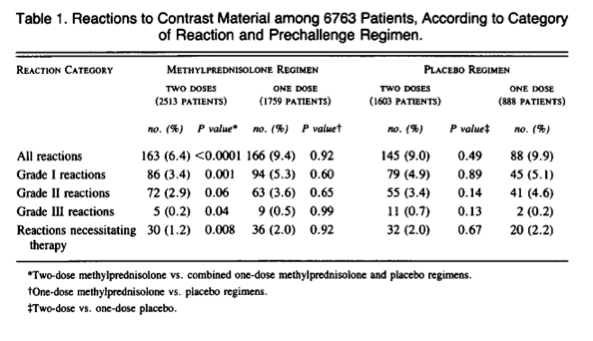
The first relevant article comes from the NEJM in 1987. Lasser and colleagues took 6,800 patients who were scheduled to receive ionic contrast (high osmolality) and divided them into 3 groups.5 They found a statistically significant reduction in all reactions in the group that received 2 doses of steroid in comparison to 1 dose regimen and placebo. However, the reduction was only in grade I or mild reactions. They found no difference in moderate or severe reactions and no difference in the number of reactions that required any kind of treatment. In essence, pretreatment was able to reduce the number of patients who developed hives but had no benefit beyond this.
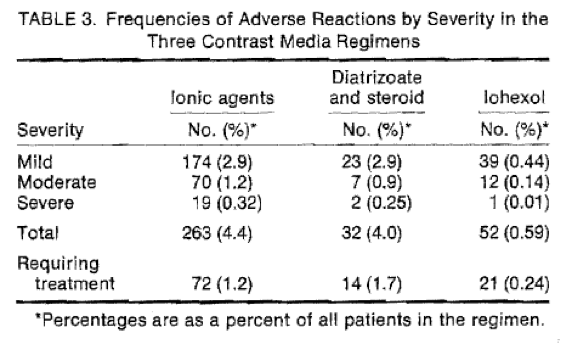
Around this time, non-ionic contrast agents began being used. These agents have lower osmolality and potentially, a lower risk for adverse reactions. Wolf and colleagues compared ionic contrast versus ionic contrast with steroid pretreatment to non-ionic contrast alone.6 They found no significant difference when comparing ionic contrast versus ionic contrast with pretreatment. However, there was a significant difference in all types of reactions between ionic contrast (with or without pretreatment) and non-ionic contrast.
The next logical step, then, would be to see if pretreatment with corticosteroids reduces adverse reactions in patients getting non-ionic contrast. Lasser and colleagues investigated this in 1994 and found a statistically significant reduction in all adverse reactions with pretreatment (1.7% vs 4.9% p = 0.005).7 Once again, however, there was no reduction in moderate or severe reactions.
Finally, the BMJ published a systematic review in 2006 where they found a small reduction in respiratory symptoms and hemodynamic compromise with pretreatment in patients getting non-ionic contrast (0.2% vs 0.9%) and estimated a NNT of 100-150.8 Additionally, they were unable to find a single case of death, CPR, irreversible neurological deficit, or prolonged hospitalization resulting from an adverse reaction to IV contrast.
What does the ACR Manual on Contrast Media recommend? The ACR states that whenever possible, nonionic contrast is preferred over ionic contrast because of the lower risk of adverse drug reactions. Despite the evidence detailed above, the ACR recommends that corticosteroids be given to reduce the likelihood of an adverse drug reaction 4-6 hours prior to administration of the IV contrast. However, they also state that premedication should not delay the CT scan in emergent situations. Finally, the ACR states, “contrast reactions occur despite premedication prophylaxis.”
Bottom Line: Premedication with corticosteroids has never been shown to reduce the risk of moderate or severe adverse drug reactions. Premedication should not delay the CT scan when the clinical information that a CT scan will give is critical to the management of the patient.
Knowing all of this, what should we do for a patient with a history of severe anaphylactoid reaction to intravenous contrast? It is critical to recognize that we don’t have any therapy to reduce the risk of a recurrent reaction. Whenever possible, we should elect for an alternate study (i.e. ultrasound, MRI etc) to avoid administration of contrast to these patients. If there is no other option, medications for treatment of the adverse reaction should be close at hand (i.e. epinephrine).
Special thanks to Salim Rezaie (@srrezaie) for editing this post.
References
- American College of Radiology Manual on Contrast Media 2012 – Version 8.
- Beaty AD et al. Seafood allergy and radiocontrast media: are physicians propagating a myth? Am J Med 2008; 121(2): 158.
- Boehm I. Seafood allergy and radiocontrast media: are physicians propagating a myth? Am J Med 2008; 121(2): 158.
- Apter AJ et al. Is there cross-reactivity between penicillins and cephalosporins? Am J Med 2006; 119: 354e11-20.
- Lasser EC et al. Pretreatment with corticosteroids to alleviate reactions to IV contrast. NEJM 1987; 317(14): 845-9.
- Wolf GL et al. Comparison of the rates of adverse drug reactions – ionic contrast agents, ionic agents combined with steroids and non-ionic agents. Investigative radiology 1991; 26(5): 404-10
- Lasser EC et al. Pretreatment with corticosteroids to prevent adverse reactions to non-ionic contrast media. AJR 1994; 162: 523-26.
- Tramer MR et al. Pharmacological prevention of serious anaphylactic reactions due to iodinated contrast media: systematic review. BMJ 2006; 33: 675.
- http://www.ncbi.nlm.nih.gov/pubmed/21854485





7 thoughts on “IV Contrast Myths”
Great overview. Here’s my question: We know that repeat exposure does NOT increase risk of rxn w/ contrast. What is the likelihood that NO reaction will happen w/ repeat exposure? We don’t want practitioners to forego dye in, say, an urgent dissection study. So what’s the actual risk of rxn in a pt. w/ known hx of anaphylactoid rxn to IV dye?
This is rare and I couldn’t find any real data on it. When I can, I try to avoid giving contrast to patients with a history of prior anaphylactoid reaction to contrast and try to find an alternate imaging modality. I agree with you, though, that it’s all a matter of how critical the imaging is.
Pingback: Profilassi antiallergica al mezzo di contrasto: serve? - EM Pills
Here’s a Q from a non radiology person. In anesthesia, we tend to give pretreatment of H1 & H2 blockers + steroid within minutes to an hour before exposure to contrast. Radiology seems to skip the H1 blocker and my local hospitals administer the pretreatment 24 hours prior to exposure. What do you do at your facilities?
Here’s a Q from a non radiology person. In anesthesia, we tend to give pretreatment of H1 & H2 blockers steroid within minutes to an hour before exposure to contrast. Radiology seems to skip the H1 blocker and my local hospitals administer the pretreatment 24 hours prior to exposure. What do you do at your facilities?
Pingback: Episode 82 – Emergency Radiology Controversies – Emergency Medicine Cases
Pingback: emDOCs.net – Emergency Medicine EducationEM Cases: Emergency Radiology Controversies - emDOCs.net - Emergency Medicine Education