Author: Angela Hua, MD (EM Resident Physician, Mount Sinai Hospital) // Edited by: Alex Koyfman, MD (EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital, @EMHighAK) and Brit Long, MD (EM Chief Resident at SAUSHEC, USAF, @long_brit)
A 41 yo M is brought in by EMS after an attempted hanging. He was found by his father-in-law, who cut him down with a neighbor’s assistance. Unwitnessed hanging, estimated 1-45min of hang time.
How should this case be managed? What are the issues to be immediately addressed, and of what complications should an emergency physician be aware?
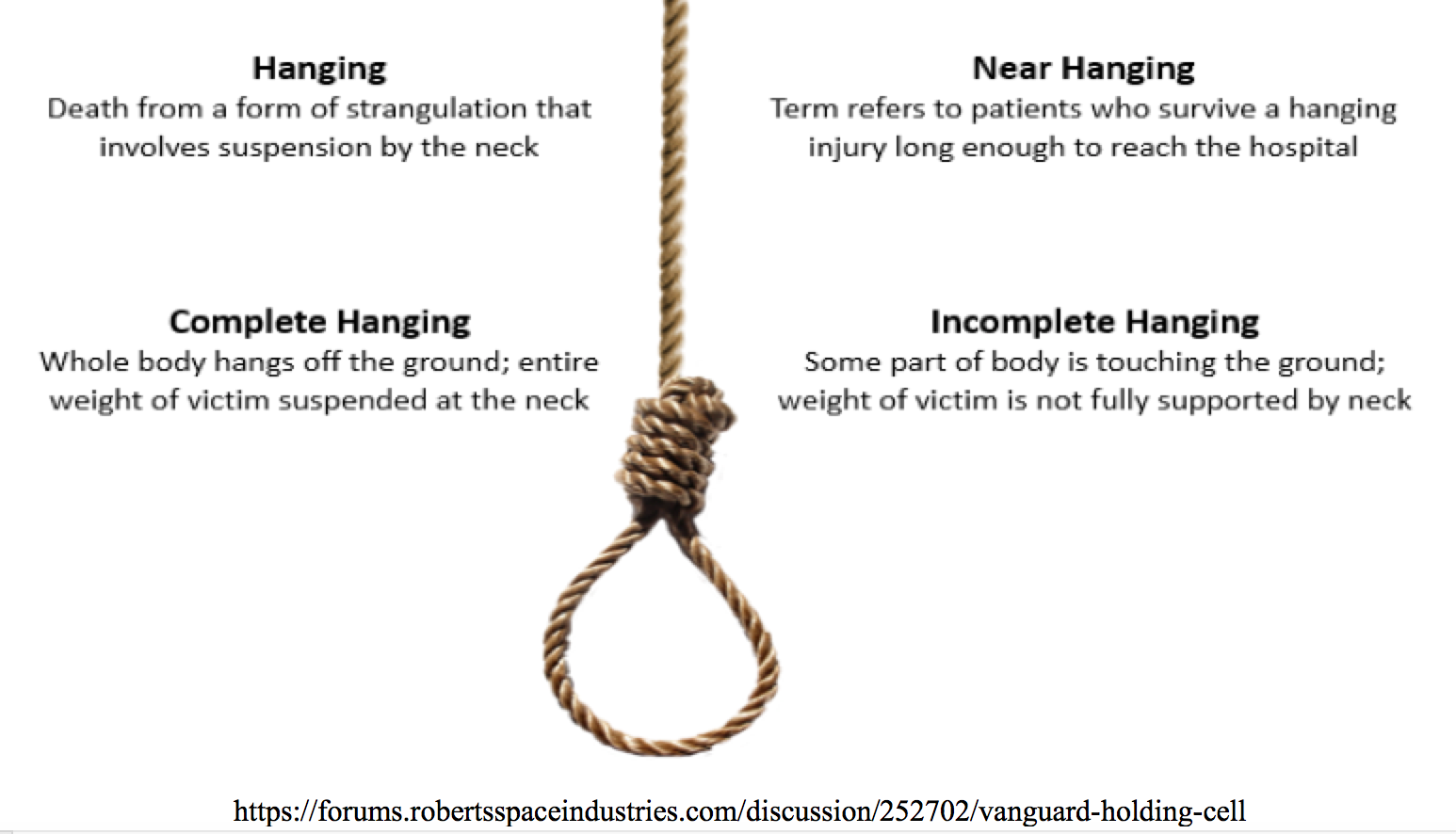
DEFINITION/CLASSIFICATION
WHY IS AWARENESS OF HANGING INJURIES IMPORTANT?
- Hanging has become the 2nd most common form of successful suicide in the US, and is one of the more common forms in the UK and Canada
- In the jail system, hanging is the most common form of successful suicide
PATHOPHYSIOLOGY
Judicial Hanging
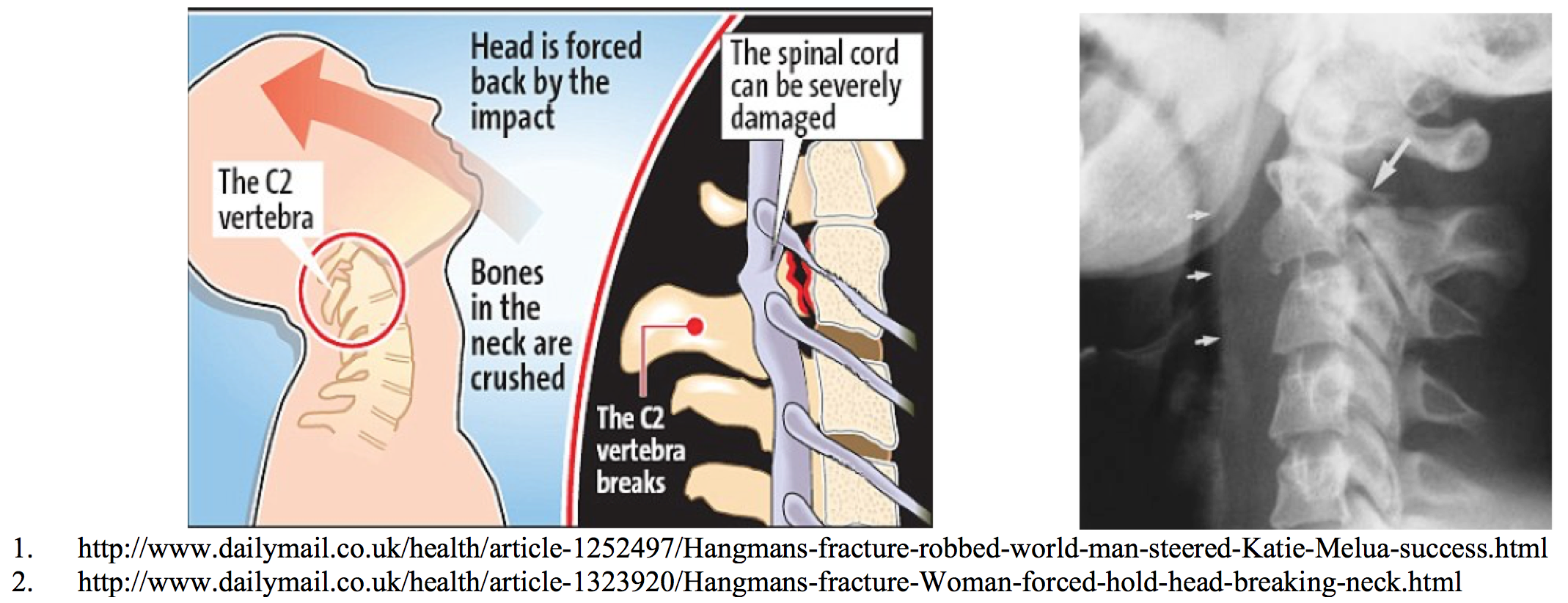
- Drop is at least as long as the height of the victim, hanging is complete
- Head hyperextends =>
- Fracture of upper cervical spine, most commonly traumatic spondylolisthesis of C2, “hangman’s fracture”
- Transection of the spinal cord
Other Strangulation Injuries
- Death ultimately results from cerebral hypoxia and ischemic neuronal death
- Airway compromise plays minimal role in the immediate death of successful strangulation victims, but initial survivors may suffer significant pulmonary complications (see below)
PHYSICAL EXAM
 Abrasions, lacerations, contusions, edema to neck
Abrasions, lacerations, contusions, edema to neck
- Tardieu spots
- Severe pain on gentle palpation of the larynx (laryngeal fracture)
- Mild cough
- Stridor
- Muffled voice
- Respiratory distress
- Hypoxia (usually late finding)
- Mental status changes
INITIAL EMERGENCY DEPARTMENT CARE – ABCs
- Endotracheal intubation (ETI) may become necessary with little warning
- If ETI unsuccessful, consider cricothyroidotomy; if unsuccessful, percutaneous trans-laryngeal ventilation may be used temporarily

- Fluid resuscitation must be performed judiciously – risk of ARDS and cerebral edema
- Monitor for cardiac arrhythmias
- Altered / comatose patient => treat as cerebral edema with elevated ICP
IMAGING STUDIES
- Soft-tissue neck x-ray

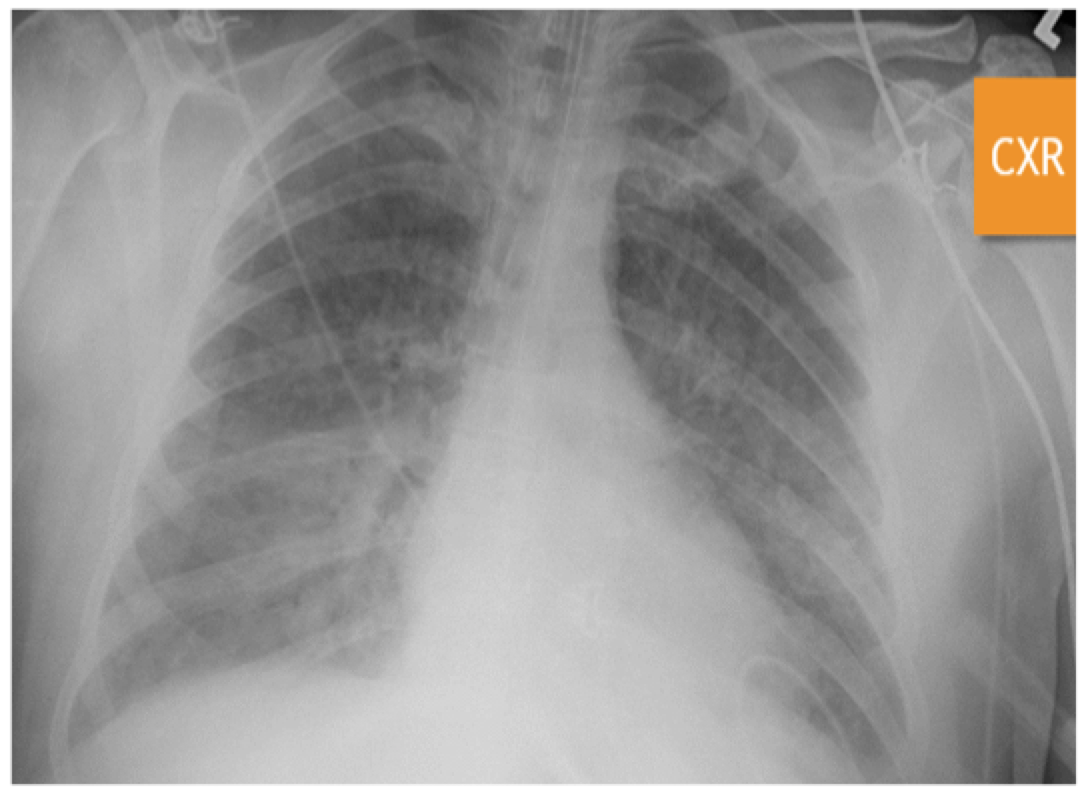
- Chest radiograph
- CT brain
- CT C-spine
- Consider CTA head/neck or MRA head/neck http://www.virtualmedstudent.com/links/musculoskeletal/hangmans_fracture.html
FURTHER CARE AND POTENTIAL COMPLICATIONS
Even if the initial presentation is clinically benign, all near-hanging victims and those with vascular compromise should be admitted for 24 hours observation => risk of delayed airway and pulmonary complications
BEWARE COMPLICATIONS!
- Respiratory complications = major cause of delayed mortality in near-hanging victims
- Pulmonary edema
- Neurogenic: centrally mediated, massive sympathetic discharge; often in association with serious brain injury, poor prognostic implication
- Post-obstructive: due to marked negative intrapleural pressure, generated by forceful inspiratory effort against extrathoracic obstruction; when obstruction removed, may have rapid onset pulmonary edema leading to ARDS
- Aspiration pneumonia
- Carotid intimal dissection or thrombus formation
- Tracheal stenosis
- Neurologic sequelae
- Transient hemiplegia
- Central cord syndrome
- Seizures
- Spinal cord injury
- Long-term paraplegia/quadriplegia
- Short-term autonomic dysfunction

PROGNOSIS
- GCS on presentation is NOT predictor of outcome
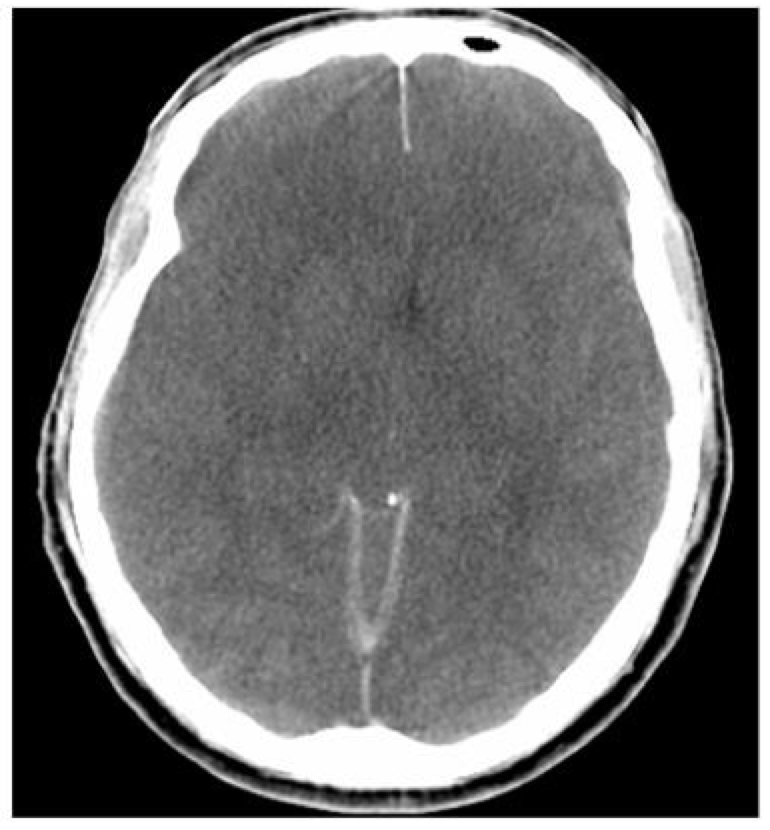
- Predictors of poor clinical outcome:

-Anoxic brain injury on head CT
-Long hanging time
-Cardiopulmonary arrest
-Cervical spine injury
-Hypotension on arrival
-PaO2/FiO2 < 100 at admission
References / Further Reading
- Berdai AM, Labib S, Harandou M. Postobstructive pulmonary edema following accidental near-hanging. American Journal of Case Reports 2014; 14: 350-353
- Borgquist O, Friberg H. Therapeutic hypothermia for comatose survivors after near-hanging—a retrospective analysis. Resuscitation 80(2009): 210-212.
- Casha S, Christie S. A systematic review of intensive cardiopulmonary management after spinal cord injury. Journal of Neurotrauma 28: 1479-1495.
- Furlan JC, Fehlings MG. Cardiovascular complications after acute spinal cord injury: pathophysiology, diagnosis, and management. Neurosurgery Focus 2008; 25(5): E13
- Gandhi R, Taneja N, Mazumder P. Near hanging: early intervention can save lives. Indian Journal of Anaestehsia 2011, 55(4): 388-391
- Kaki A, Crosby ET, Lui ACP. Airway and respiratory management following non-lethal hanging. Can J Anaesth 1997 44(4): 445-450
- Irvin CB, Szpunar S, Cindrich LA, et al. Should trauma patients with a Glasgow Coma Scale score of 3 be intubated prior to hospital arrival? Prehospital Disaster Medicine 2010 25(6) 541-6.
- Mack EH. Neurogenic shock. The Open Pediatric Medicine Journal 2013, 7 (suppl 1: M4) 16-18
- Mansoor S, Afshar M, Barett M, et al. Acute respiratory distress syndrome and outcomes after near hanging. American Journal of Emergency Medicine 2015, 33: 359-362.
- Newton K, Claudius I. Rosen’s Emergency Medicine – Concepts and Clinical Practice. 8th Edition (2014). Volume 1, Part II, Chapter 44 pp 421-431.
- Nickson C. Trauma! Spinal injury. Life in the Fast Lane. http://lifeinthefastlane.com/trauma-tribulation-016/
- Salim A, Martin M, Sangthong B. Near-hanging injuries: a 10-year experience. Injury, Int J Care Injured 2006, 37: 435-439.
- Trujillo MH, Fragachan CF, Tortoledo F. Noncardiogenic pulmonary edema following accidental near-hanging. Heart & Lung. 2007 36(5) 363-366.




