Author: Derek Marcantel, MD (EM Resident Physician, LSUHSC-Shreveport), Ashley Arnold, MD (OB/GYN Resident Physician, LSUHSC-Shreveport), and Avery Callahan, DO (EM Attending Physician, LSUHSC-Shreveport) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM physician at SAUSHEC, USAF)
A 27-year-old gravida 1, para 1 female presents to the ED via EMS for shortness of breath, swelling of the lower extremities, and severe headache. The patient states that these symptoms began 2 days ago when she got home from the hospital after an uneventful stay on the obstetrics unit, where she completed an otherwise healthy pregnancy by delivering a healthy newborn male. She states that her head is pounding, her vision is swimming, and she is having trouble catching her breath. Examination reveals an ill-appearing woman with a blood pressure of 188/115, HR 110, RR 30, O2 saturation of 94% on 2L NC placed by EMS. Auscultation reveals bilateral crackles and 2+ pitting edema in the lower extremities bilaterally.
As you begin to question the patient further, she becomes unresponsive and begins to suffer from a generalized tonic-clonic seizure.
Your team then looks to you for instructions on how to proceed.
Hypertensive disorders in pregnancy affect about 5% to 10% of all pregnancies in the USA.1 The American College of Obstetrics and Gynecology (ACOG) differentiates these into2:
- Chronic hypertension
- Chronic hypertension with Superimposed Preeclampsia
- Preeclampsia-Eclampsia
- Gestational hypertension
In this article, we will focus our attention on two of the hypertensive disorders that emergency physicians must be able to identify, treat, and provide an appropriate disposition for: preeclampsia and eclampsia.
Preeclampsia
This is classically defined as the new onset of hypertension and either proteinuria or end-organ dysfunction after 20 weeks of gestation in a previously normotensive woman.3 This is the most common form of hypertension that complicates pregnancy. The criteria for diagnosis of severe preeclampsia are below.2
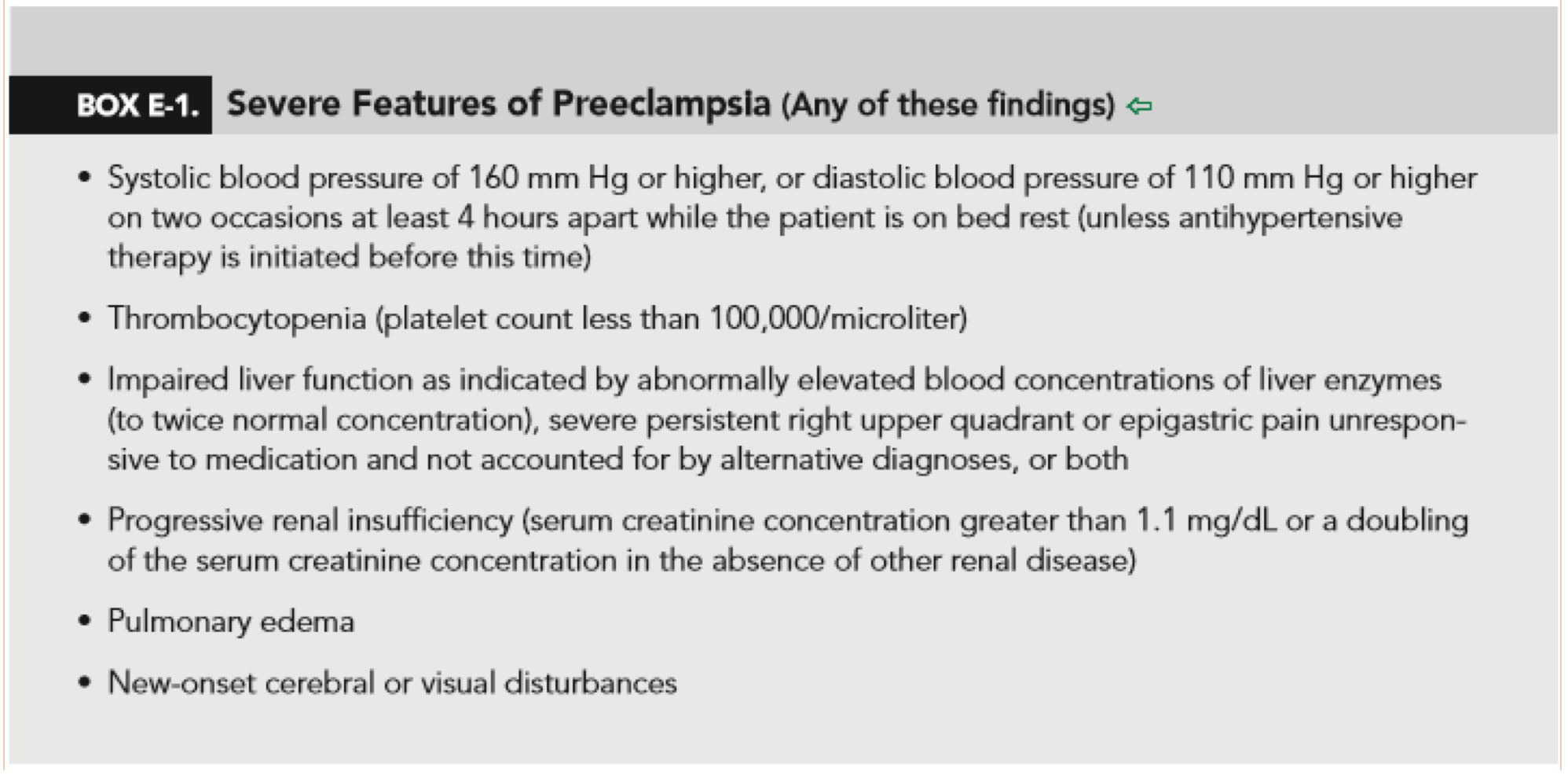
From http://www.acog.org/Resources-And-Publications/Task-Force-and-Work-Group-Reports/Hypertension-in-Pregnancy
The pathogenesis is unclear, but it is thought to be related to an abnormal placenta; more specifically, placental hypoperfusion. The signs and symptoms of preeclampsia all relate to endothelial dysfunction and increased vascular permeability. Research as to why this occurs is still ongoing, but it remains poorly understood at this time.
It is important for the emergency provider to be aware of the significant morbidity and mortality associated with this disease process. This includes, but is not limited to3,4:
- Placental abruption
- AKI
- Cerebral hemorrhage
- Hepatic failure
- Pulmonary edema
- DIC
It is also essential for the emergency physician to realize that this process can occur in the postpartum period, as late as 4 weeks after delivery.3,5
The typical history of preeclampsia is vague. Patients are typically diagnosed on routine prenatal visits. However, as emergency physicians are aware, severe hypertension can cause blurry vision, headaches, and other symptoms that would drive patients to seek acute care in the emergency department.
A proper diagnostic workup would be similar to the workup performed in hypertensive emergency, which includes evaluation for end organ damage, a check for proteinuria, and control of BP with anti-hypertensive medication. Typical medications used in the acute phase include nifedipine, labetalol, and hydralazine, with ACOG suggesting that labetalol be first line unless a contraindication is present. Doses suggested by ACOG are in the table below. Maximize one agent before moving on to the next agent. Continue with aggressive therapy with frequent BP checks (every 10-15 minutes) until the blood pressure is below 160/110 mmHg.1,2 Some authors suggest the use of nicardipine in refractory cases, but there have been no large RCTs showing the safety and efficacy of this drug in the pregnant patient.6
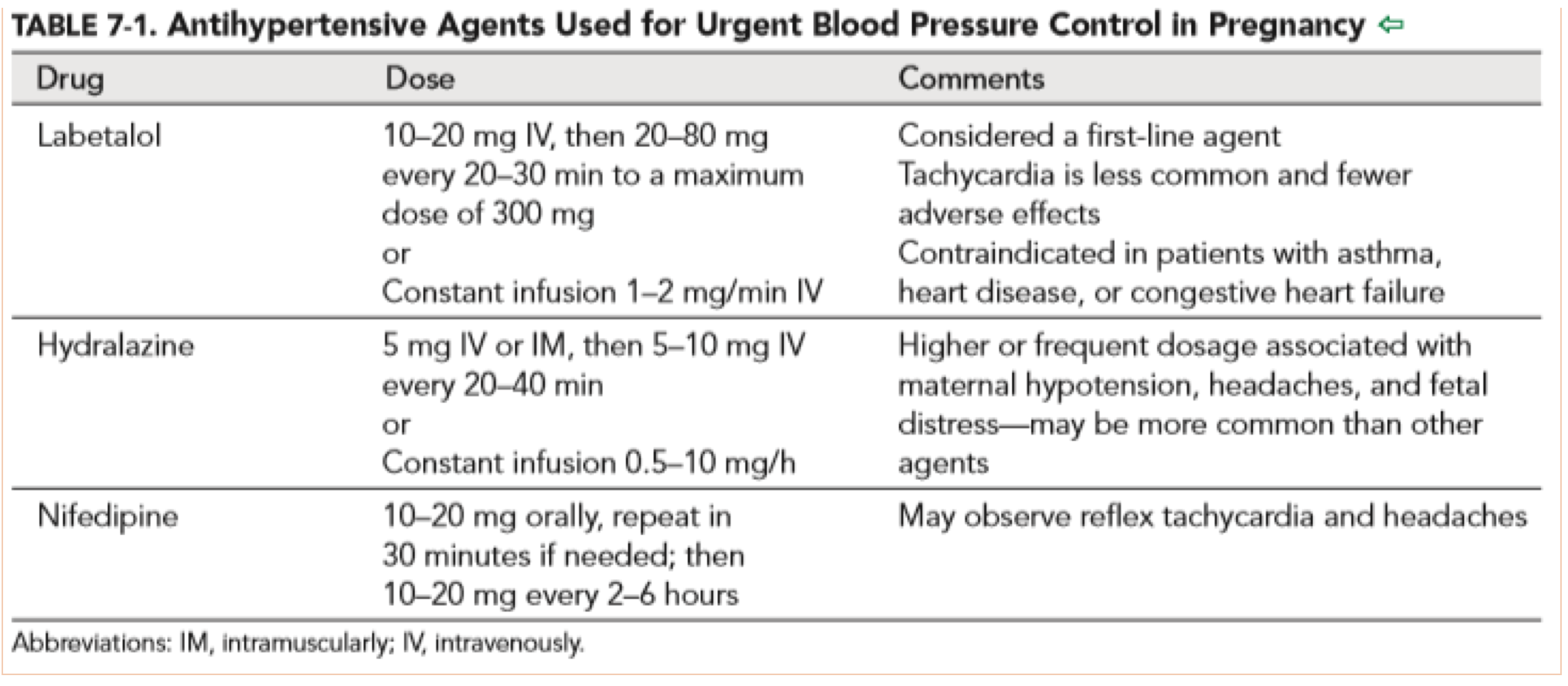
From http://www.acog.org/Resources-And-Publications/Task-Force-and-Work-Group-Reports/Hypertension-in-Pregnancy
Preeclampsia without severe features (previously called mild preeclampsia) has the potential to be managed in the outpatient setting in close collaboration with the patient’s obstetrician. However, an emergency physician should not make the call to discharge a patient with preeclampsia without talking to an OB/GYN.2
Preeclampsia with severe features is never discharged home. The definitive treatment for preeclampsia is delivery. These patients are admitted to the perinatal floor and every attempt is made to keep the patient pregnant until 34 weeks. However, if the patient deteriorates sooner, the patient is delivered anyway.2
Antepartum preeclampsia is unlikely to be diagnosed in the ED. As mentioned earlier, these patients are typically picked up on routine OB visits and are managed by their obstetricians. A more likely pitfall for the emergency physician comes in the form of postpartum preeclampsia.
Postpartum onset of preeclampsia can quickly progress to eclampsia. The most dangerous time period for late onset is 24-48 hours after delivery, but this can occur as far as 4 weeks out from delivery.3,4 Because of this, the emergency physician must keep this in the differential for any postpartum patient (i.e. home delivery, little to no prenatal care) presenting with elevated BP and signs of end organ damage. In addition to anti-hypertensives, magnesium should be given to these patients in short order to avoid progression to eclampsia and consultation with the patient’s obstetrician is advised.2,3,4
Also, remember that since the patient has delivered, the full armamentarium of anti-hypertensives is at your disposal, so do not necessarily limit the choices to nifedipine, hydralazine, and labetalol.
Eclampsia
Eclampsia is the development of generalized tonic-clonic seizure in a patient who has preeclampsia. This is essentially a form of hypertensive encephalopathy due to the aforementioned increase in vascular permeability. Only 38% of eclamptic seizures occur antepartum; a further 18% occur in labor and 44% occur postpartum. Outcomes are poor: 1 in 50 women will die from eclampsia, 23% will require mechanical ventilation, and 35% will have major organ system dysfunction associated with eclampsia. One third of eclamptic seizures occur outside of the emergency department. These patients will present to the emergency department, and the emergency physician needs to be prepared to care for these critically ill patients.7,8
The first line medication for this is magnesium sulfate. 1,2,3,9 Magnesium is given IM if necessary while IV access is being obtained. Magnesium is provided at 4-6 g IV load over 15 minutes, followed by 2-3 g/hr. The IM route includes up to 10 g. Benzodiazepines can be given in refractory situations, or if magnesium is not readily available. A gravid-appearing woman having seizures should be presumed to have eclampsia until proven otherwise.
Remember, this can present to the ED postpartum. In an undifferentiated, unresponsive patient, making this diagnosis in the ED can be challenging. It must be in the differential for the female patient that is seizing without an obvious cause and no history of seizures.3,4,8
The administration of magnesium is only a temporizing measure. Emergent delivery, usually by caesarean, is required by an obstetrician. Get them involved as soon as an eclamptic patient arrives. These patients require centers that are capable of caring for high-risk obstetrics and premature infants, so stabilization and transfer may be required.1,2,7,9
Take Home Points
- Preeclampsia is a common hypertensive disorder in pregnancy
- Preeclampsia is responsible for a significant amount of both maternal and fetal morbidity and mortality
- Severe preeclampsia requires aggressive blood pressure control with hydralazine, nifedipine, and labetalol; it may also require prophylactic magnesium sulfate, discuss with OB
- It is considered poor form to discharge preeclampsia patients without an OB/GYN on board
- Preeclampsia/Eclampsia can manifest postpartum
- Eclampsia requires emergent delivery (if antepartum) and magnesium sulfate
References / Further reading
- Alexander JM, Wilson KL. Hypertensive Emergencies of Pregnancy. Obstetrics and Gynecology Clinics of North America. 2013;40(1):89-101. doi:10.1016/j.ogc.2012.11.008.
- American College of Obstetrics and Gynecology Task Force on Hypertension in Pregnancy. Hypertension in Pregnancy. ACOG Practice Guideline. 2013:1-79.
- Graeber B, Vanderwal T, Stiller RJ, Werdmann MJ. Late postpartum eclampsia as an obstetric complication seen in the ED. The American Journal of Emergency Medicine. 2005;23(2):168-170. doi:10.1016/j.ajem.2004.04.035.
- Yancey LM, Withers E, Bakes K, Abbott J. Postpartum Preeclampsia: Emergency Department Presentation and Management. The Journal of Emergency Medicine. 2011;40(4):380-384. doi:10.1016/j.jemermed.2008.02.056.
- Kuklina EV, Ayala C, Callaghan WM. Hypertensive Disorders and Severe Obstetric Morbidity in the United States. Obstetrics & Gynecology. 2009;113(6):1299-1306. doi:10.1097/aog.0b013e3181a45b25.
- Nooij L, Visser S, Meuleman T, Vos P, Roelofs R, Groot CD. The Optimal Treatment of Severe Hypertension in Pregnancy: Update of the Role of Nicardipine. Current Pharmaceutical Biotechnology CPB. 2014;15(1):64-69. doi:10.2174/1389201015666140330194722.
- Munro PT. Management of eclampsia in the accident and emergency department. Emergency Medicine Journal. 2000;17(1):7-11. doi:10.1136/emj.17.1.7.
- Small KR, Cannava M, Casey S, Jacques J. Tonic-Clonic Seizures in a Postpartum Patient: Case Report. American Journal of Critical Care. 2010;19(3):307-305. doi:10.4037/ajcc2010668.
- Olson-Chen C, Seligman NS. Hypertensive Emergencies in Pregnancy. Critical Care Clinics. 2016;32(1):29-41. doi:10.1016/j.ccc.2015.08.006.





3 thoughts on “Preeclampsia and Eclampsia: Common Pitfalls in Diagnosis and Management”
Pingback: Preeclampsia and Eclampsia: Common Pitfalls in Diagnosis and Management – emdocs – EM & CC
Pingback: emDOCs.net – Emergency Medicine EducationElemental EM: Preeclampsia - emDOCs.net - Emergency Medicine Education
Pingback: Sh!t I Learned This Week 2019.03.30 – Future Flight Medic