Authors: Alessandra Della Porta MS3, EMT-B (@mededtweeter); Jean-Paul Bryant MS4, MSc (@paulyb126); Kasha Bornstein MS4, MSc, EMT-P (@bornstein-kasha); University of Miami School of Medicine; Tim Montrief MD, MPH (@EMinMiami, Critical Care Fellow University of Pittsburgh Medical Center) // Reviewed by: Manny Singh, MD (@MprizzleER); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)
Case
A 48-year-old woman presents to the ED with a ten-day history of low back pain that she notes began after lifting boxes in her garage. She has a past history of injection drug use and rheumatoid arthritis controlled with methotrexate. She sought care two days earlier at an urgent care and was prescribed cyclobenzaprine for a presumed lumbar sprain. She has had intermittent fevers that improve with acetaminophen, but her pain has grown worse in the past 72 hours, now occurring with shooting sensations down her legs bilaterally. On exam, her vitals are stable with a temperature of 99.4 ℉. She has mild weakness in her left lower extremity and full bilateral extremity pulses. What is the next step in evaluation?
Introduction
Spinal epidural abscess (SEA) is a rare, highly morbid, and often life-threatening, neurosurgical emergency characterized most often by a suppurative monomicrobial infection of the central nervous system, confined within the epidural space between the dura mater and the vertebral periosteum. Incidence has steadily increased in the past decade from 0.5 cases per 10,000 admissions to nearly 10 cases per 10,000 admissions.1 This is related to a combination of factors including population aging, increasing numbers of spinal surgeries, increasing population morbidity of diabetes and other immune compromising conditions, and increased case finding as access to highly sensitive diagnostic imaging studies such as magnetic resonance imaging (MRI) has become widespread.1 SEA can present as a constellation of symptoms including a classic triad of midline back pain, fever, and focal neurologic deficits such as lower extremity paresis, saddle anesthesia, and bladder and bowel dysfunction.1 However, SEA is an elusive and challenging diagnosis as symptomatology varies significantly. The classic triad is present in fewer than 15% of patients, while back pain, the only presenting symptom in nearly 75% of patients experiencing SEA, is also a common chief concern for adult emergency department visits with a wide differential including many benign etiologies.2
Mortality ranges between approximately 3-25%,3-6 and approximately 5% of patients die from associated sepsis or other related causes.7 Associated severe, disabling morbidity is common; between 4-22% of patients with SEA experience catastrophic neurologic sequelae including irreversible paraplegia and other deficits.4 Fewer than 50% of surviving patients have full return to baseline neurologic status.8 As many as 50-75% of patients with SEA may be initially misdiagnosed.9,10 Those most likely to receive operative management within 24 hours already have a high rate (~88%) of neurologic deficits.11 The development of focal neurological symptoms may be seen as a late sign: the presence and duration of neurologic deficits correlate significantly with adverse outcomes, and retrospective analysis has demonstrated poor reversal rates of neurological deficits in delayed surgeries.4 Patients treated with operative evacuation within 24 hours are noted to have significantly improved motor scores versus those who receive later surgical intervention.9
The most significant modifiable risk factor for morbidity and mortality is time to surgical decompression, as neurological symptoms are produced by local mass effect and abscess intrusion into spinal cord arterial blood supply, disc spaces, and spinal cord segments.4,8 Research into conservative management has demonstrated utility of antibiotic management +/- percutaneous drainage in select patient populations, including patients who are medically unstable for operative management and younger patients with no comorbidities and no neurologic symptoms.4-6,12 In the setting of conservative management, time to antibiotic management is cited as the most important factor attenuating morbidity and mortality.5 Nonetheless, review of patients treated conservatively revealed as many as 41% will require surgical intervention.9Patients with diabetes, C-reactive protein greater than 115 mg/L, white blood cell count (WBC) greater than 12.5/mL, ring enhancement on MRI, acute or progressive motor deficits, and positive blood cultures, particularly methicillin resistant Staphylococcus aureus, were more likely to fail antibiotic treatment alone.9,12 As such, correct management requires a low threshold for further evaluation with imaging studies and neurosurgical and/or interventional radiology consultation.12
Risk Factors
Index of suspicion for focused evaluation should be heightened in patient populations with significant demographic and etiologic risk factors, described in greater detail in table 1, including age >65, comorbid illness, injection drug use, diabetes, and recent surgical or procedural instrumentation of the spine.7,12 SEA most often occurs in the setting of compromised host immunity, with introduction or hematogenous seeding of flora from an initial infectious nidus into spinal epidural tissue.7
There are three main pathophysiologic mechanisms for development of SEA. Spontaneous SEA is most often regarded as a complication of a primary spinal infection like spondylodiscitis, with hematogenously spread via septic thrombosis of epidural veins.8 Infections of the epidural space may also propagate from hematogenous metastasis from distant foci such as urinary tract infections, pneumonia, retropharyngeal abscess, perirenal abscess and bacterial endocarditis.6 Infections may also result following iatrogenic introduction of bacteria into the spinal epidural space or local structures, most often in the setting of spinal surgery, epidural injection therapy, and spinal anesthesia, but also as adverse sequelae of dental procedures and upper endoscopy.13,14 Finally, smoldering infections in adjacent structures such as vertebral osteomyelitis, spondylodiscitis, and perispinal mass abscesses may translocate into the epidural space.15 In as many as one third of SEA cases, there is no identifiable primary infectious nidus.7
The mean age of patients presenting with SEA is 50 years, with a prevalence peak between 30-70 years of age.5,7Diabetes mellitus is the most significant risk factor for SEA, with at least a third of patients presenting with SEA bearing a prior history of diabetes.7 Intravenous drug use is a significant risk factor for development of SEA, particularly in the setting of the contemporary opioid epidemic.16 A 2000 to 2013 analysis of the Healthcare Cost and Utilization Project National Inpatient Sample found one in five SEA patients aged 15-64 had a history of injection drug use.17 Subacute or chronic bacterial infections (bacteremia, endocarditis, skin and soft tissue infections, osteomyelitis) can seed bacteria and/or septic emboli resulting in SEA, particularly in patients who use drugs with limited access or barriers to medical care.16 Other risk factors include chronic renal and liver failure, chronic alcohol use, HIV, recent local trauma, indwelling catheters, and acupuncture.18,19

Microbiology
Pathogens isolated from blood cultures and wound cultures are typically concordant. Staphylococcus aureus accounts for the majority (65-70%) of SEA cases, with methicillin sensitive and methicillin resistant strains common depending on local antibiograms sampled.20 Gram-negative bacilli (most often Escherichia coli) account for approximately 15-20% of cases, streptococcal infections, Enterobacter, Klebsiella, and other bacteria/mycobacteria/fungi accounting for the remainder of infections. Pseudomonas has been noted in patients with a proximal history of injection drug use. Polymicrobial infections are rare and are described in the case report literature as sequelae of gastrointestinal and esophageal procedures.21 Given the wide differential of culprit pathogens, antibiotic regimens should be initiated early following collection of blood cultures. Appropriate empiric antibiotic regimens should be active against staphylococci (including MRSA), streptococci, and gram-negative bacilli, such as combination vancomycin plus ceftriaxone. For patients in whom Pseudomonas is suspected, such as those with recent or current admission to intensive care units, who have implanted hardware, recent use of antibiotics, or diabetes mellitus, an appropriate regimen should have antipseudomonal activity including cefepime, ceftazidime, or meropenem. Given the time sensitive nature of SEA, antibiotics should not be delayed to obtain a pretreatment aspirate of abscess fluid in patients in whom SEA is strongly suspected.8
Challenges to Diagnosis
SEA is a relatively rare condition and despite its increasing incidence may not be considered in the initial assessment of common chief complaints, such as low back pain. Given that low back pain is the fourth most common reason for adult emergency department visits, and fifth most common for general physician visits overall, patients presenting with symptoms consistent with SEA may first be diagnosed with more common musculoskeletal causes.22,23 Correct diagnosis is often made after multiple visits to the emergency department.24-26 Several studies have demonstrated that over fifty percent of patients have seen a healthcare provider greater than two times in the 30 days prior to their correct diagnosis.16,27 Delay to appropriate diagnosis in patients with SEA can be attributed to many factors, including nonspecific presentation, delay in ordering or receiving results from confirmatory studies, and interplay of various coexisting conditions.1
History and Physical Examination
In the majority of cases, signs and symptoms of SEA are subtle and diagnosis requires detailed history taking alongside low threshold to pursue further diagnostics in the most vulnerable patient populations. As mentioned, the “classic triad” of SEA; spinal pain, fever and neurologic deficits, has been documented as a specific but very insensitive indicator of SEA, as all three components are present in only 10-15% of cases.27 While back pain is the most common chief complaint and symptom in patients with SEA, it is nonspecific and has a vast differential diagnosis. Back pain may be indolent and non-focal for several weeks, and then advance to severe, localizable pain with radicular features prior to onset of cord compression and paralysis. Fever has been reported in up to 55% of patients with SEA but can vary in severity based on disease progression and time from onset of symptoms to presentation.28 As SEA can often arise from distant sites of infection, when present, fever may be initially attributed as part of the response to originating foci.29 In patients who present with neurologic findings, deficits may be either sensory, motor, or both. These findings may be present in up to 50% of patients and a large range of reported symptoms exists from loss of reflexes, motor weakness, radiculopathy, loss of anal sphincter tone, and paraplegia.22,27,28
The role of physical examination in the diagnosis of patients with SEA is controversial as sensitivity remains low. This may be due to the fact that observable neurologic symptoms develop late in the course of disease, difficulty in obtaining a full neurological exam in the ED, or failure to complete this portion of the exam altogether. Retrospective studies of patients diagnosed with SEA have demonstrated low documentation rates of the key components of the neurologic exam, especially rectal tone and sensation.27 Additionally, these findings may be particularly hard to ascertain in patients who are chronically ill, bedbound, live with chronic pain, are obtunded, or have neurologic deficits at baseline.22,23 Considering that neurologic findings are often present late in disease course, and consistent with other conditions that are more common causes of back pain, such as disc herniation, they are often not reliable enough to ensure early and correct diagnosis.16
Laboratory Testing
Beyond blood and abscess culture, there are no specific laboratory tests or biomarkers for SEA. No single laboratory test has adequate sensitivity and specificity to discern SEA from other infections.30 Laboratory data may be used in aggregate to prognosticate illness and predict mortality. Blood cultures yield an organism in roughly half of patients with SEA.10 Several aspects of the work up for low back pain have high sensitivity but low specificity in SEA. Leukocytosis is present in 38-70% of cases, but only moderate elevations in WBC are usually noted and degree of elevation does not correlate to prognosis.30 C-reactive protein (CRP) is highly sensitive (68-100%), as is erythrocyte sedimentation rate (ESR) at 84%.30 However, these acute phase reactants are elevated in a wide spectrum of diseases. CRP concentration declines quickly in disease resolution and may be used to guide time to treatment completion.30 Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio are clinical scoring tools with wide use for predicting disease severity in many inflammatory and infectious conditions. NLR and PLR been previously identified as useful markers for risk stratification and efficient surgical disposition in necrotizing soft tissue infections.31 Higher neutrophil-lymphocyte and platelet-lymphocyte ratios are indicative of worse prognosis.31 Recent evidence suggests utility of NLR as an independent risk predictor for 90-day mortality in SEA.31,32
Imaging Studies
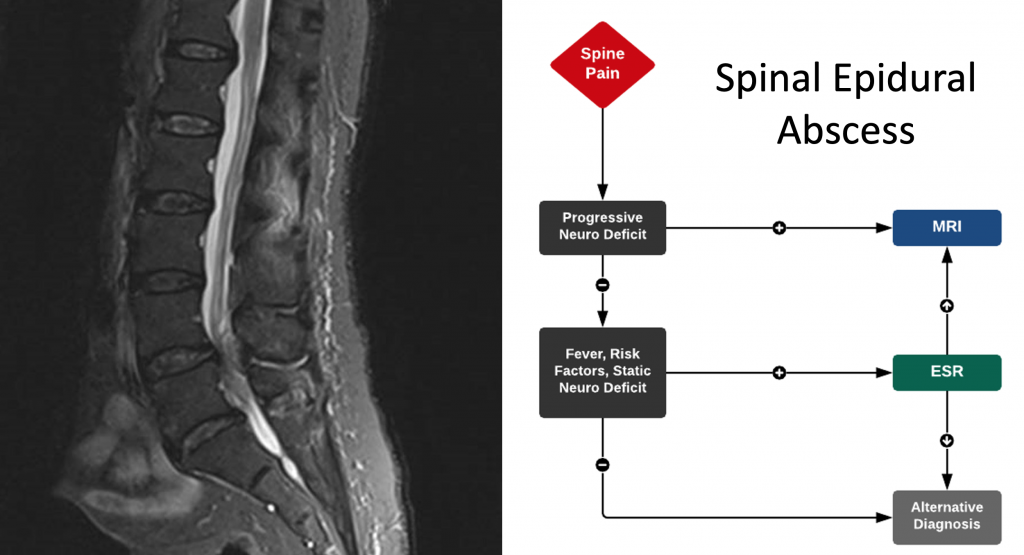
The confirmatory diagnostic study for the vast majority of patients is MRI with a sensitivity of 95% and specificity above 90% (Image 1). In the absence of MRI access, CT scanning with intravenous contrast may demonstrate fluid collections in the epidural space.27 Plain radiographs of the spine may demonstrate associated osteomyelitis, spondylodiscitis, and/or vertebral collapse if infection extends into or translocated from local structures. While these should be performed, they are not enough to establish the diagnosis. As osteomyelitic changes may not be present within the first three weeks of symptoms, reliance on plain radiography may produce falsely negative findings. Plain radiography indicating findings suggestive acute infection are present in fewer than one-third of patients.33

One final challenge to the diagnosis of spinal epidural abscess is the interplay of various coexisting conditions and risk factors. First, up to 50% of patients have a coexisting or contiguous infection that predisposed the patient to developing SEA.16,34 Common infections include pneumonia, osteomyelitis, endocarditis and superficial skin infections. As these may be the primary presenting complaints on arrival to the emergency department or the reason why the patient is hospitalized, they may outcompete signs of SEA for the clinicians’ attention. Furthermore, as fever, leukocytosis, and ESR and CRP may be elevated in various infectious states, in cases of coexisting infection, diagnosis of SEA may be complicated even more. Second, known risk factors for the development of SEA, many of which do so by increasing likelihood of bacteremia, are very common in ED patients.23,35 Risk factors such as intravenous (IV) drug usage increase risk in multiple ways, via direct inoculation, spread from skin abscess and any concomitant immunosuppressive states that may be present.36 As these patients may present to the emergency department with multiple concerns, and later in disease course due to inability to easily access care, special attention should be paid to patients at increased risk. One study of patients with SEA found that patients with concomitant IV drug usage were more likely than other cases to experience diagnostic and admission delays.27
Improving Emergency Department Diagnosis of SEA
An important factor in the prognosis of patients with SEA is time-to-diagnosis, as diagnostic delays can have potentially devastating consequences. Due to the uncommon nature and diagnostic challenges mention previously, emergency departments have reported diagnostic delays, defined as multiple ED visits prior to diagnosis or an admission to a nonsurgical service without initially diagnosing SEA but subsequently diagnosing SEA during that admission, in up to 84% of individuals.37 Although this principle area of reducing delays has been identified, the question of how best to intervene and produce better outcomes remains more equivocal. Due to the cost and length of time required to obtain MRI images and interpretation, it is not the first imaging considered in many patients presenting to the ED with back pain. As it is a necessary study to diagnose or rule out SEA, several algorithms have been created to parse out which patients may benefit from MRI and if the study is needed on an emergent basis.26 Algorithms may decrease the diagnostic delay, and take into account patient presentation, laboratory values and known risk factors for the development of SEA. The impact of these algorithms on diagnosis of SEA must be balanced by the feasibility of the increase in MRI utilization and the desire to minimize unnecessary imaging.22,23,27
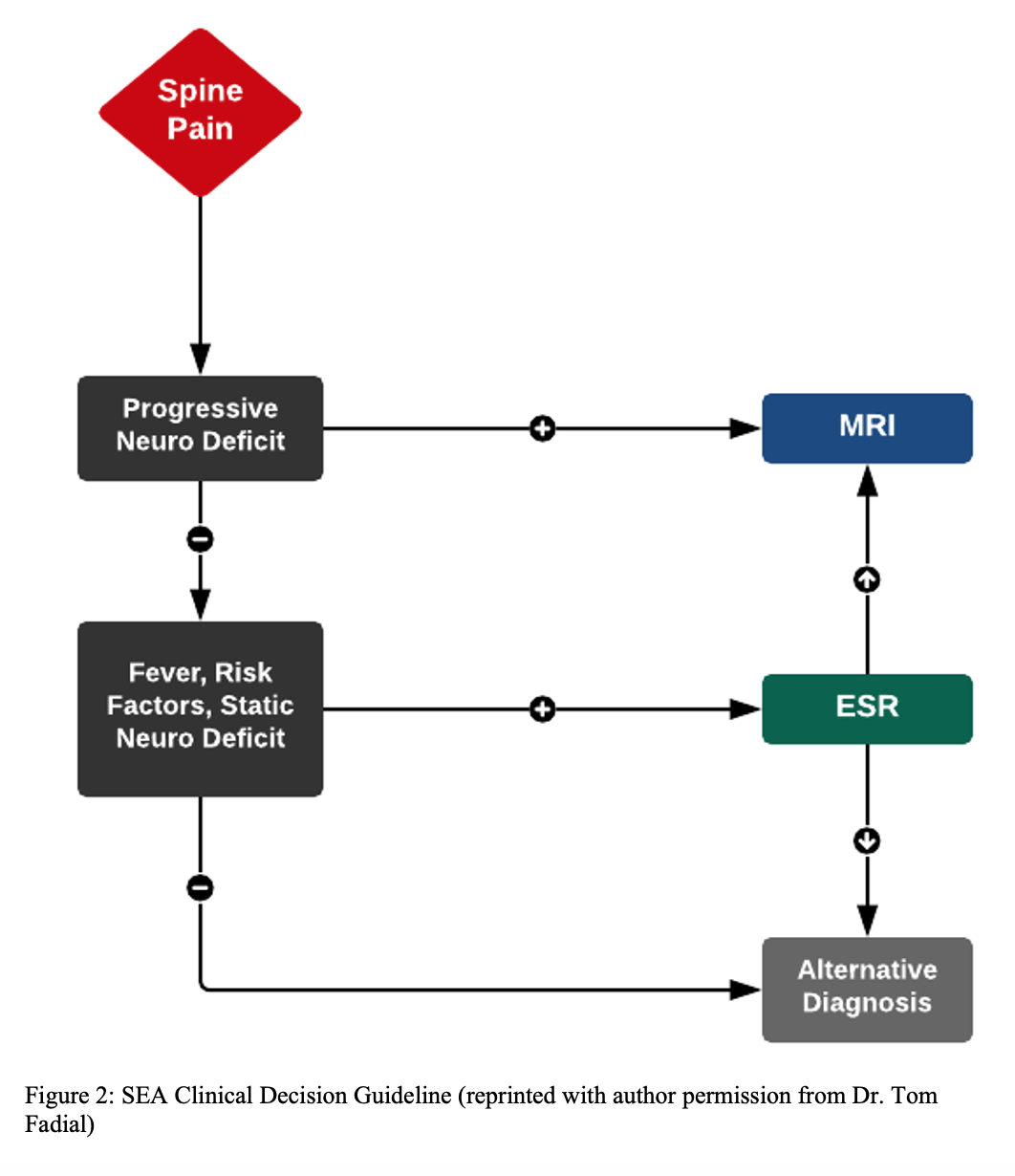
Initially, it is imperative to screen patients presenting to the ED with midline and/or radicular pain with any SEA risk factors including: diabetes, history of intravenous drug use, chronic liver or kidney disease, recent spinal fracture or surgery, indwelling vascular catheter, other sites of infection, and/or an immunocompromised state. If the patient has one or more risk factors in conjunction with spine pain, emergent MR is recommended for those with progressive neurological deficits or elevated inflammatory markers (ESR or CRP).1 Davis et al. evaluated this clinical decision guideline in an ED-based study, finding diagnostic delays, as defined as multiple ED visits prior to diagnosis or admission to nonsurgical service without diagnosis, were reduced by 73.9% in a cohort of 86 patients.26 Furthermore, implementation of this approach reduced the rate of neurological complications (i.e. motor deficits) present at time of diagnosis by 62.4%.26
Since the findings by Davis et al., similar algorithms have been presented that diverge slightly, some suggesting that patients without back pain but at high risk for SEA due to recent bacteremia should be considered for routine MRI examination. This strategy is comparable to that of screening for signs of endocarditis in patients presenting with bacteremia due to S. aureus infection. This concept is supported by a study that identified an identical rate of endocarditis and SEA in patients presenting with MRSA bacteremia.38 Madhuripan et al. (2017) devised an algorithm (Figure 1) for a streamlined screening suspected SEA cases prompting STAT MRI orders, which resulted in an immediate and sustained decrease in order-to-read, and scan completion–to–read time periods for imaging patients with suspected SEA. That protocol yielded nearly three times more studies compared with baseline, without changing the frequency of significant positive studies.1 Madhuripan et al. (2017) recommend neurology as the primary admission team; however, this is dependent on the institution. Most centers will not use neurology as the primary team, but rather, the most important factor is involving the spinal surgeon/neurosurgeon and infectious disease specialist. Resources vary by hospital facility; the key takeaway is that as a time-sensitive neurologic emergency, management of patients with SEA should be centralized and efficient. An even more streamlined clinical decision guideline was developed by Dr. Tom Fadial with recommendation of MRI in all patients with spine pain and progressive neurologic deficits (Figure 2).

While MRI remains the diagnostic study of choice, other imaging modalities with possible benefit in identifying patients with SEA are being explored. One such modality is point-of-care ultrasound for measuring post void residual volume (PVR) in patients with progressive neurological dysfunction due to a suspected SEA.39 Healthy adults typically have the urge to void at a bladder volume of 300 mL. A PVR of over 200 mL indicates inadequate emptying which can be quickly measured by ultrasound in cases where catheterization is contraindicated.40 Of note, many use over 100 mL as the threshold concerning for spinal compression. PVR values do not directly correlate to SEA, but early recognition of subtle neurologic deficits can aid in early detection and intervention.
In addition to the implementation of clinically based diagnostic algorithms to diagnose SEA, EDs have employed statistical models to aid in early recognition. One department retrospectively applied an Integrated Discrimination Improvement Index (IDI) which represents the degree to which patient variables can increase the probability of an event in cases, while simultaneously decreasing the probability of an event in controls.41 Studied variables included age, fever and/or rigors, recent antimicrobial use, back or neck pain and intravenous drug use. Using data from a 10-year period, this predictive model determined a sensitivity of 89% for patients with a cut-point of six points for cases that subsequently required emergent spinal imaging. Given the importance of expeditious diagnosis for favorable prognosis, an accurate scoring model could provide an additional data point to aid in clinical decision-making.
Additional challenges to diagnosis and management of SEA are the detection of noncontiguous SEAs or skip lesions. Skip lesions present a significant diagnostic challenge as providers may not reflexively order imaging of additional spinal segments when the patient presents with symptoms that are consistent with a single lesion (i.e. lower back pain or lower extremity radiculopathy).42 The consequences of failing to diagnose a skip lesion can be grave, with isolated infection progressing to sepsis or continued neurological decline. As concurrent and noncontiguous SEA may be present in up to 9% of patients diagnosed with a SEA, whole spine imaging may represent an additional area for improvement.43 Furthermore, this study demonstrated that patients with skip lesions may differ significantly from patients with single lesions in three variables: ESR, delay of symptom onset to ED presentation (≥7 days), and other sites of infection outside of the spinal or paraspinal region. Eighty-three percent of patients with skip lesions had an ESR ≥ 95 mm/h as compared to 30% in those with a single lesion.10 Given that measuring ESR is often suggested in diagnostic algorithms this value combined with clinical judgement could be used as a screening tool for the detection of noncontiguous lesions.
Conclusion
Diagnosing patients with SEA can be challenging due to nonspecific symptoms and presentation that overlaps with a myriad of pathological processes. Given its potential for causing rapid clinical deterioration, time from symptom onset to diagnosis is critical in managing this disease process. Areas that could benefit from continued research include reducing this diagnostic time interval and implementation of whole spine imaging when indicated to detect the presence of noncontiguous lesions.
Take home points
Why is spinal epidural abscess a challenging diagnosis?
- Back pain is a common chief complaint, while SEA is a rare condition.
- SEA presents with non-specific symptoms and infrequently with the classic triad.
- Diagnosis requires expensive and time-consuming imaging (MRI).
- Coexisting infections or risk factors are common in the ED setting.
How can we improve diagnostic delay of SEA?
- Implementation of decision-making algorithms can reduce time intervals of ED presentation to diagnosis.
- Statistical models have accurately discriminated cases from non-cases of SEA.
- Focused exam, such as the PVR, can detect subtle neurologic deficits and increase our assessment sensitivity.
- When indicated, early whole spine imaging can detect skip lesions and prevent delays in diagnosing multiple abscess locations.
References/Further Reading
- Madhuripan N, Hicks RJ, Feldmann E, Rathlev NK, Salvador D, Artenstein AW. A Protocol-Based Approach to Spinal Epidural Abscess Imaging Improves Performance and Facilitates Early Diagnosis. J Am Coll Radiol. 2018;15(4):648-651.
- Muck AE, Balhara K, Olson AS. Finding the needle in the haystack. Internal and Emergency Medicine. 2018;13(2):219-221.
- Du JY, Schell AJ, Kim CY, Trivedi NN, Ahn UM, Ahn NU. 30-day Mortality Following Surgery for Spinal Epidural Abscess: Incidence, Risk Factors, Predictive Algorithm, and Associated Complications. Spine (Phila Pa 1976). 2019;44(8):E500-E509.
- Epstein NE. Timing and prognosis of surgery for spinal epidural abscess: A review. Surg Neurol Int. 2015;6(Suppl 19):S475-486.
- Adogwa O, Karikari IO, Carr KR, et al. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014;20(3):344-349.
- Eltorai AEM, Naqvi SS, Seetharam A, Brea BA, Simon C. Recent Developments in the Treatment of Spinal Epidural Abscesses. Orthop Rev (Pavia). 2017;9(2):7010.
- Ameer MA, Knorr TL, Mesfin FB. Spinal Epidural Abscess. In: StatPearls. Treasure Island (FL)2020.
- Lener S, Hartmann S, Barbagallo GMV, Certo F, Thomé C, Tschugg A. Management of spinal infection: a review of the literature. Acta Neurochir (Wien). 2018;160(3):487-496.
- Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. The Spine Journal. 2014;14(2):326-330.
- Bond A, Manian FA. Spinal Epidural Abscess: A Review with Special Emphasis on Earlier Diagnosis. BioMed research international. 2016;2016:1614328-1614328.
- Ghobrial GM, Beygi S, Viereck MJ, et al. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014;37(2):E1.
- Tuchman A, Pham M, Hsieh PC. The indications and timing for operative management of spinal epidural abscess: literature review and treatment algorithm. Neurosurg Focus. 2014;37(2):E8.
- Radulovic D, Vujotic L. Cervical spinal epidural abscess after oesophagoscopy. Eur Spine J. 2013;22 Suppl 3(Suppl 3):S369-S372.
- Rainsford KD, Parke AL, Clifford-Rashotte M, Kean WF. Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases. Inflammopharmacology. 2015;23(5):231-269.
- Ying J, Pei S, Su L, Wen T, Lv Y, Ruan D. Successful Conservative Management of Delayed Cervical Spondylodiscitis with Epidural Abscess Caused by Esophageal Diverticulitis: A Case Report and Review of Literature. World Neurosurg. 2018;118:250-260.
- Artenstein AW, Friderici J, Holers A, Lewis D, Fitzgerald J, Visintainer P. Spinal Epidural Abscess in Adults: A 10-Year Clinical Experience at a Tertiary Care Academic Medical Center. Open Forum Infectious Diseases. 2016;3(4).
- Toppo AJ, Rogerson A, Oh DHW, Tybor DJ, Wurcel AG, Salzler MJ. Injection Drug Use in Patients With Spinal Epidural Abscess: Nationwide Data, 2000 to 2013. Spine. 2020;45(12).
- Godhania V. Lumbar spine osteomyelitis and epidural abscess formation secondary to acupuncture. Journal of Surgical Case Reports. 2016;2016(3).
- Chan JJ, Oh JJ. A rare case of multiple spinal epidural abscesses and cauda equina syndrome presenting to the emergency department following acupuncture. International Journal of Emergency Medicine. 2016;9(1):22.
- Ma H, Kim I. Clinical outcomes of spinal epidural abscess. Korean J Spine. 2012;9(1):6-11.
- Akhondi H, Baker MB. Epidural Abscess. In: StatPearls. Treasure Island (FL)2020.
- Alerhand S, Wood S, Long B, Koyfman A. The time-sensitive challenge of diagnosing spinal epidural abscess in the emergency department. Intern Emerg Med. 2017;12(8):1179-1183.
- Muck AE, Balhara K, Olson AS. Finding the needle in the haystack. Intern Emerg Med. 2018;13(2):219-221.
- Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL. Spinal epidural abscess: a report of 40 cases and review. Surg Neurol. 1992;38(3):225-231.
- Yang X, Guo R, Lv X, et al. Challenges in diagnosis of spinal epidural abscess: A case report. Medicine (Baltimore). 2019;98(5):e14196.
- Davis DP, Salazar A, Chan TC, Vilke GM. Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain. 2011;14(6):765.
- Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med. 2004;26(3):285-291.
- Bond A, Manian FA. Spinal Epidural Abscess: A Review with Special Emphasis on Earlier Diagnosis. Biomed Res Int. 2016;2016:1614328.
- Mackenzie AR, Laing RB, Smith CC, Kaar GF, Smith FW. Spinal epidural abscess: the importance of early diagnosis and treatment. J Neurol Neurosurg Psychiatry. 1998;65(2):209-212.
- Chenoweth CE, Bassin BS, Mack MR, et al. In: Vertebral Osteomyelitis, Discitis, and Spinal Epidural Abscess in Adults. Ann Arbor (MI)2018.
- Karhade AV, Shah KC, Shah AA, Ogink PT, Nelson SB, Schwab JH. Neutrophil to lymphocyte ratio and mortality in spinal epidural abscess. Spine J. 2019;19(7):1180-1185.
- Karhade AV, Shah AA, Bono CM, et al. Development of machine learning algorithms for prediction of mortality in spinal epidural abscess. Spine J. 2019;19(12):1950-1959.
- Amini MH, Salzman GA. Infectious spondylodiscitis: diagnosis and treatment. Mo Med. 2013;110(1):80-84.
- Chima-Melton C, Pearl M, Scheiner M. Diagnosis of spinal epidural abscess: a case report and literature review. Spinal Cord Ser Cases. 2017;3:17013.
- Tijunelis MA, Fitzsullivan E, Henderson SO. Noise in the ED. Am J Emerg Med. 2005;23(3):332-335.
- Shweikeh F, Saeed K, Bukavina L, Zyck S, Drazin D, Steinmetz MP. An institutional series and contemporary review of bacterial spinal epidural abscess: current status and future directions. Neurosurg Focus. 2014;37(2):E9.
- Davis DP, Salazar A, Chan TC, Vilke GM. Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain. J Neurosurg Spine. 2011;14(6):765-770.
- Horino T, Sato F, Hosaka Y, et al. Predictive factors for metastatic infection in patients with bacteremia caused by methicillin-sensitive Staphylococcus aureus. The American journal of the medical sciences. 2015;349(1):24-28.
- Alerhand S, Wood S, Long B, Koyfman A. The time-sensitive challenge of diagnosing spinal epidural abscess in the emergency department. Internal and Emergency Medicine. 2017;12(8):1179-1183.
- Sakakibara R, Yamamoto T, Uchiyama T, et al. Is lumbar spondylosis a cause of urinary retention in elderly women? Journal of neurology. 2005;252(8):953-957.
- Artenstein AW, Friderici J, Visintainer P. A Predictive Model Facilitates Early Recognition of Spinal Epidural Abscess in Adults. The western journal of emergency medicine. 2018;19(2):276-281.
- Mellado JM, Pérez del Palomar L, Camins A, Salvadó E, Ramos A, Saurí A. MR imaging of spinal infection: atypical features, interpretive pitfalls and potential mimickers. European radiology. 2004;14(11):1980-1989.
- Ju KL, Kim SD, Melikian R, Bono CM, Harris MB. Predicting patients with concurrent noncontiguous spinal epidural abscess lesions. Spine J. 2015;15(1):95-101.




