Authors: Dennis Nmecha, MD and Jason Rotoli, MD (University of Rochester-Strong Memorial Hospital Department of Emergency Medicine) // Reviewed by: Michael J. Yoo, MD (EM Assistant Professor, San Antonio, TX); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
On a typical summer morning in the emergency department (ED), you evaluate a patient with a chief complaint of “headache.” The patient is a 33-year-old female who presents with multiple days of a positional headache. The headache started while she was outside golfing. She states that the current headache episode is different from her typical headaches. Her pain is worse while she sits or stands up and completely resolves when she is lying down. Review of systems is positive for nausea but negative for weakness, vision changes, numbness, tingling or other neurologic symptoms. The patient denies recent trauma. Her focused physical exam is noted below:
Initial vital signs: 36.7°C, HR 73, RR 16, BP 120/74, 100% on room air
General: lying comfortably in a dark room, denies active pain
Mental status: AAOx3
Neurologic: no focalizing deficits, equal strength/sensation throughout, self-ambulatory without ataxia
You consider a broad differential diagnosis for her headache, to include tension and migraine headache, space occupying mass, cavernous sinus thrombosis, carbon monoxide poisoning, infection, and post-procedural (lumbar puncture) headache. What else should we consider in a patient with an atypical headache, that is now positional in nature?
Background and Etiology
Spontaneous intracranial hypotension (SIH) is a clinical condition defined by postural headaches attributed to cerebrospinal fluid (CSF) leaks or low CSF volumes.(1) Historically, SIH has been attributed to a drop in CSF pressure which can occur as a result of trauma, surgery, CSF leak, and a CSF shunt with over drainage.(2-3) Headaches are a result of the low CSF volume. Classically described as a pressure like sensation, the pain is caused by sinking of the brain away from the meninges and its resultant traction on the pain sensitive fibers.(4) A CSF leak is a result of dural defects (in the form of fistulas or tears) and can be congenital or traumatic. There are various risk factors that can lead to leakage of CSF including the absence of dura around the nerve root sheaths, congenital connective tissue disorders causing structural abnormalities, osteophyte protrusions, and the herniation of the spinal disc.(5) Focal weakness in the dura occurs most commonly around the thoracic and lumbar spine.(5) Subsequently, spinal manifestations such as local back pain can occur at the site of the CSF leak.(6)
Epidemiology
SIH is often underdiagnosed and mistaken for other pathologies (see below for differential diagnoses). The incidence of SIH is around 5 in 100,000 and is more common in females, with a female to male ratio 2:1.(5) Both children and adults can be affected by SIH, though the peak incidence of SIH around 40 years old.(7)
Symptoms
Headaches can be bifrontal, occipital, or holocephalic (global) in location. The pain is typically acute, orthostatic, and can worsen with Valsalva maneuvers (which worsen CSF leakage).(4) In addition to postural headaches, other symptoms of SIH include nausea, vomiting, vertigo, tinnitus, blurred or double vision, unsteady gait, neck stiffness, anorexia, facial numbness, and paresthesia in the upper limbs.(7-9) Unfortunately, these symptoms are neither sensitive nor specific in the diagnosis of SIH, and the constellation of SIH symptoms may mimic typical migraine headaches, meningitis, and psychogenic or somatoform disorders.
Differential Diagnosis
The differential diagnosis of headaches is extensive, and the following is neither an exhaustive nor inclusive list. However, the following should be considered in any patient presenting with headaches:
– Headache disorder (new daily persistent headache)
– Subarachnoid hemorrhage
– Carotid or vertebral artery dissection
– Cerebral venous thrombosis
– Benign intracranial hypertension
– Posttraumatic headache
– Meningitis
For a more generalized discussion on the approach to headaches in the ED, you can visit here and here.
Evaluation
As with any patient in the ED, you should always address life threatening vital signs, assess the patient’s airway, breathing, and circulation, and perform a thorough exam. Once you know the patient is stable, your efforts should be focused on obtaining a detailed history and physical exam. A high index of suspicion is necessary, as SIH is often confused for other etiologies of headache. There are no specific labs necessary to diagnose SIH. However, you can and should obtain other relevant labs if you are trying to rule out other causes emergent causes headaches (i.e. CSF studies for meningitis). Advanced imaging that can assist the ED physician in the diagnosis of SIH is discussed below.
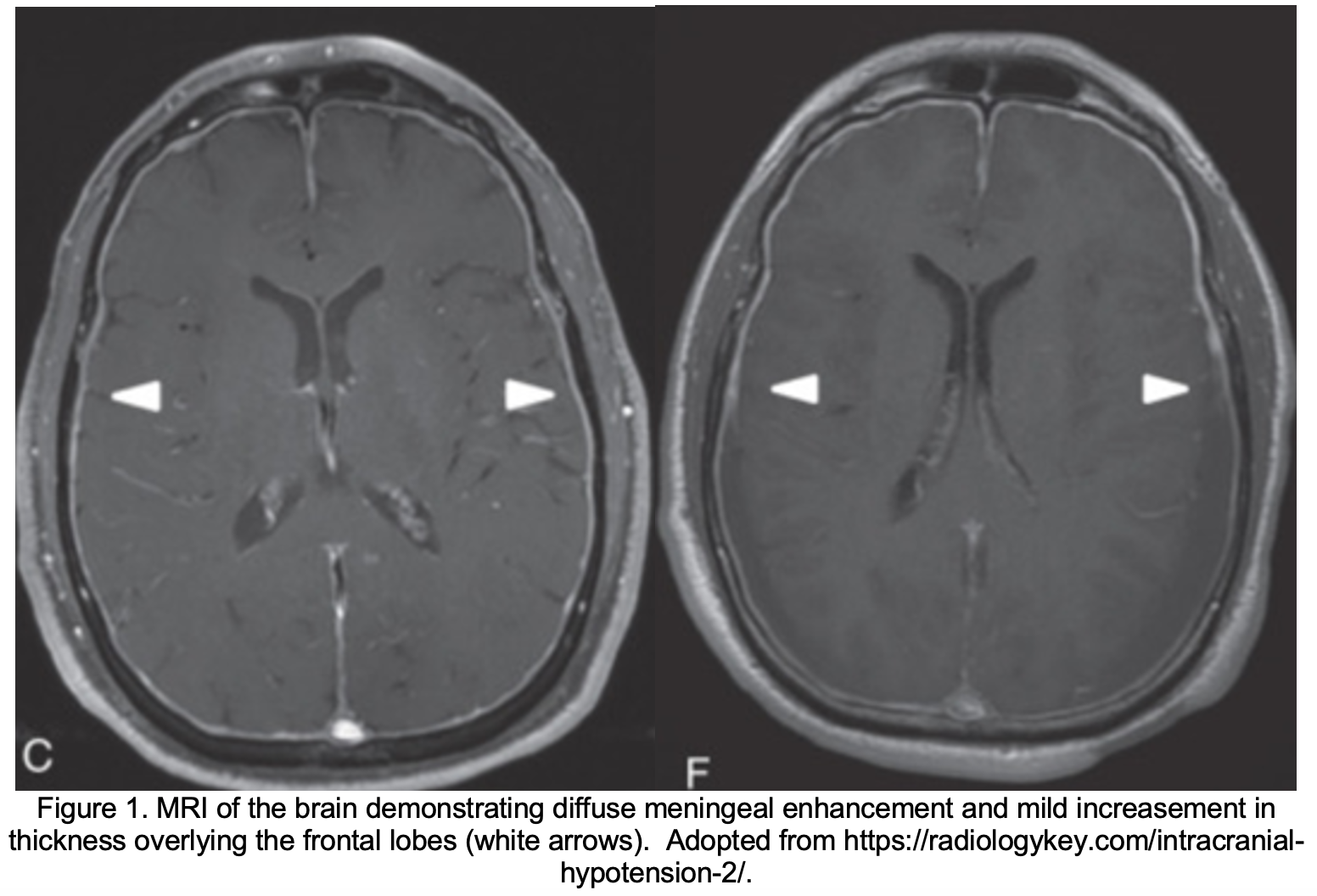
Magnetic resonance imaging (MRI) of the brain. The main imaging modality that would be helpful in obtaining the diagnosis of SIH is an MRI of the brain with and without contrast. The acronym SEEPS, which stands for Subdural fluid collections, pachymeningeal Enhancement, venous Engorgement, Pituitary hyperemia, and brain Sagging are the main features of SIH seen on MRI.(6) Of these findings, the most common and pathognomonic finding is diffuse uniform pachymeningeal enhancement.(10) In layman terms, this means enhancement of the dura and outer layer of the arachnoid following contrast administration for a brain MRI.
MRI of the spine. Obtaining an MRI of the spine may be helpful in identifying the source of CSF leak. The findings on a MRI of the spine include the epidural leakage of the fluid, presence of meningeal diverticula, fluid collection in the extra-meningeal cavity, and the shrinking of the dural sac with concomitant epidural venous plexus distension.(11)

Myelography. Myelography with iodinated contrast of the entire spine (or with gadolinium followed by MRI) has been shown to be the study of choice to accurately define the location and extent of a CSF leak.(6) Although multiple leaks are frequently found along the spine, the majority of CSF leaks are found at the cervicothoracic junction or along the thoracic spine.(7)
Non-contrasted computed tomography (CT) of the head. Although not as definitive as MRI, CT may suggest the diagnosis by showing subdural fluid collections or obliteration of subarachnoid cisterns and ventricular collapse.(12-14) If unable to coordinate obtaining a MRI in the ED setting, CT imaging is a reasonable first line of imaging despite the lower sensitivity and specificity to rule out malignant and emergent etiologies of headache and identify secondary findings associated with SIH.
Imaging considerations. While MRI of the brain and spine are diagnostic for SIH, they are often difficult to obtain in the ED setting due to resource allocation and timing. Alternative solutions for diagnosis include admission to an observation unit (if available) or the hospital for an urgent MRI if clinical suspicion is high, and the patient is unable to tolerate conservative treatment (discussed below). If the patient can tolerate conservative treatment and deemed safe for discharge, outpatient follow up with neurology and an outpatient MRI may also be a viable option.
Treatment
The treatment of SIH usually depends on the severity of the disease. For mild cases, conservative therapy is often trialed first. This includes bed rest, avoiding sitting upright, oral hydration, and analgesics, such as acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs).(15) Response to oral caffeine has shown to be largely unpredictable but, if attempted, a dose of 200mg TID or 300mg QID would be reasonable.(16,17) Regarding steroids, their use in SIH remains a controversial topic.(18) However, there are cases in which oral steroids have been successful in treating SIH. In particular, one small study demonstrated that a 2-4 week course of oral prednisone at 50mg/day was successful in treating SIH in 3 patients.(19) Subsequently, steroid therapy should be tailored patient by patient, with consideration for its side-effects on other comorbid conditions.
If the symptoms persist after 1 to 2 weeks of conservative management (or if the headache is associated with debilitating features), the next therapy that is considered is an epidural blood patch (EBP). EBPs are theorized to work by producing a tamponade effect around the site of CSF leak, leading to short term resolutions of symptoms. Outside of the immediate post-procedural period, EBPs promote the deposition of fibrin and formation of scar tissue around the leak sites. This procedure can be repeated, if necessary.(20) If EBPs do not lead to symptom improvement, epidural fibrin glue and surgical correction of the leaks are the next treatment options.(5) However, both epidural fibrin glue seal and surgical correction of the CSF leaks require the identification of the points where the CSF leak is occurring.(7,21) Finally, patients who fail adequate treatment with EBP and do not have a confirmed location of CSF leaks are treated with continuous epidural infusion of dextran or saline.(22) This should be done by anesthesiology or neurosurgery and can help in replenishing the CSF volume, which can, in turn, alleviate the symptoms.
Disposition
If the patient’s symptoms are well controlled with analgesics, antiemetics, and hydration, the patient can go home with strict return precautions with outpatient neurology follow-up. If patient has an intractable headache or are unable to tolerate oral fluids or medications due to their symptoms, an admission is warranted for consideration of an EBP and other advanced treatment as discussed above. This should be done in conjunction with your neurology colleagues.
Case Conclusion
The patient underwent a CT and CTA of the brain showing no acute intracranial abnormalities. An MRI of the brain was subsequently obtained, which revealed diffuse pachymeningeal enhancement and thickening and engorgement of the dural venous sinus. The patient was admitted to the observation unit for further workup, including an MRI T/L spine, which showed a large epidural fluid collection likely from injury to T5-T6 nerve root sheath. Anesthesiology was consulted, and she received an epidural blood patch and discharged home with resolution of her symptoms.
Take Away Points
– Consider spontaneous intracranial hypotension in a patient who presents with a postural headache.
– SIH is underdiagnosed and often mistaken for other etiologies of headache as many symptoms of this condition are non-specific. It predominantly affects females. Children can also have SIH.
– MRI of the brain with and without contrast is the main imaging modality for the diagnosis of SIH and will show pachymeningeal enhancement.
– If unable to coordinate an MRI from the ED, a head CT is a reasonable first line of imaging despite the lower sensitivity and specificity to rule out emergent etiologies of headache and identify secondary findings associated with SIH.
-Treatment depends on the severity of the presentation. Conservative therapy is trialed first. If that is not effective, other treatment options include steroids, epidural blood patch, fibrin glue, surgical correction of leaks, or epidural infusion of dextran and saline.
References and Further Reading
1D’Antona L, Jaime Merchan MA, Vassiliou A, et al. Clinical Presentation, Investigation Findings, and Treatment Outcomes of Spontaneous Intracranial Hypotension Syndrome. JAMA Neurology. 2021;78(3):329. doi:10.1001/jamaneurol.2020.4799
2Mokri B, Hunter SF, Atkinson JL, Piepgras DG. Orthostatic headaches caused by CSF leak but with normal CSF pressures. Neurology. 1998;51(3):786-790. doi:10.1212/wnl.51.3.786
3Schievink WI, Reimer R, Folger WN. Surgical treatment of spontaneous intracranial hypotension associated with a spinal arachnoid diverticulum. Journal of Neurosurgery. 1994;80(4):736-739. doi:10.3171/jns.1994.80.4.0736
4Mokri B. Spontaneous Low Pressure, Low CSF Volume Headaches: Spontaneous CSF Leaks. Headache: The Journal of Head and Face Pain. 2013;53(7):1034-1053. doi:10.1111/head.12149
5Liaquat MT, Jain S. Spontaneous Intracranial Hypotension. 2021 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32644492.
6Schievink WI, Meyer FB, Atkinson JLD, Mokri B. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. Journal of Neurosurgery. 1996;84(4):598-605. doi:10.3171/jns.1996.84.4.0598
7Schievink WI. Spontaneous Spinal Cerebrospinal Fluid Leaks and Intracranial Hypotension. JAMA. 2006;295(19):2286. doi:10.1001/jama.295.19.2286
8Silberstein SD, Marcelis J. Review Article: Headache Associated With Changes in Intracranial Pressure. Headache: The Journal of Head and Face Pain. 1992;32(2):84-94. doi:10.1111/j.1526-4610.1992.hed3202084.x
9Fernandez E. Headaches Associated with Low Spinal Fluid Pressure. Headache: The Journal of Head and Face Pain. 1990;30(3):122-128. doi:10.1111/j.1526-4610.1990.hed3003122.x
10Mokri B, Piepgras DG, Miller GM. Syndrome of Orthostatic Headaches and Diffuse Pachymeningeal Gadolinium Enhancement. Mayo Clinic Proceedings. 1997;72(5):400-413. doi:10.4065/72.5.400
11Starling A, Hernandez F, Hoxworth JM, Trentman T, Halker R, Vargas BB, Hastriter E, Dodick D. Sensitivity of MRI of the spine compared with CT myelography in orthostatic headache with CSF leak. Neurology. 2013 Nov 12;81(20):1789-92.
12Sipe JC, Zyroff J, Waltz TA. Primary intracranial hypotension and bilateral isodense subdural hematomas. Neurology. 1981;31(3):334-334. doi:10.1212/wnl.31.3.334
13Murros K, Fogelholm R. Spontaneous intracranial hypotension with slit ventricles. Journal of Neurology, Neurosurgery & Psychiatry. 1983;46(12):1149-1151. doi:10.1136/jnnp.46.12.1149
14Schievink WI, Maya MM, Tourje J, Moser FG. Pseudo-subarachnoid hemorrhage: A CT-finding in spontaneous intracranial hypotension. Neurology. 2005;65(1):135-137. doi:10.1212/01.wnl.0000167192.86419.15
15Upadhyaya P, Ailani J. A Review of Spontaneous Intracranial Hypotension. Current Neurology and Neuroscience Reports. 2019;19(5). doi:10.1007/s11910-019-0938-7
16Kong D-S, Park K, Nam DH, et al. Clinical Features and Long-term Results of Spontaneous Intracranial Hypotension. Neurosurgery. 2005;57(1):91-96. doi:10.1227/01.neu.0000163093.38616.35
17Urbach H, Fung C, Dovi-Akue P, Lützen N, Beck J. Spontaneous Intracranial Hypotension. Dtsch Arztebl Int. 2020;117(27-28):480-487. doi:10.3238/arztebl.2020.0480
18Lin J, Zhang S, He F, Liu M, Ma X. The status of diagnosis and treatment to intracranial hypotension, including SIH. The Journal of Headache and Pain. 2017;18(1). doi:10.1186/s10194-016-0708-8
19Gentile S, Giudice RL, Martino PD, Rainero I, Pinessi L. Headache attributed to spontaneous low CSF pressure: report of three cases responsive to corticosteroids. European Journal of Neurology. 2004;11(12):849-851. doi:10.1111/j.1468-1331.2004.00898.x
20Marcelis J, Silberstein SD. Spontaneous Low Cerebrospinal Fluid Pressure Headache. Headache: The Journal of Head and Face Pain. 1990;30(4):192-196. doi:10.1111/j.1526-4610.1990.hed3004192.x
21Crul Ben JP, Gerritse Bastiaan M, van Dongen Robert TM, Schoonderwaldt Hennie C. Epidural Fibrin Glue Injection Stops Persistent Postdural Puncture Headache. Anesthesiology. 1999;91(2):576-577. doi:10.1097/00000542-199908000-00039
22Binder DK, Dillon WP, Fishman RA, Schmidt MH. Intrathecal Saline Infusion in the Treatment of Obtundation Associated with Spontaneous Intracranial Hypotension: Technical Case Report. Neurosurgery. 2002;51(3):830-837. doi:10.1097/00006123-200209000-00045




