Authors: Jenna Pallansch, MD, Emergency Medicine Resident, Carolinas Medical Center, Charlotte, NC; Kathryn T. Kopec, DO, Emergency Medicine Attending, Medical Toxicologist, Carolinas Medical Center, Charlotte, NC; Cynthia Santos, MD (@CynthiaSantosMD), Assistant Professor, Emergency Medicine, Medical Toxicology, Addiction Medicine, Rutgers NJMS // Editors: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)

Case:
A 6-year-old female presents to the Emergency Department (ED) for weakness and difficulty walking. Vitals on arrival: HR 105 bpm, RR 20 breaths/min, BP 114/72 mmHg, 95% SpO2 on room air, T 99.7F.
On exam, she has 3/5 strength in bilateral lower extremities and subjective paresthesias in her bilateral lower extremities and hands. She appears to have trouble swallowing with intermittent coughing but has a normal voice. She is unable to walk on her own without falling.
Questions:
- What is the toxicologic differential for acute onset paralysis?
- What features are most important in your history and exam?
- Which toxins have specific antidotes?
Background:
- Weakness is commonly reported in patients presenting to the ED and among the top ten chief complaints in patients greater than 65 years old.1
- Guillain-Barré Syndrome (GBS), while rare, is the most common cause of acute onset symmetric paralysis with an incidence of approximately 0.4 – 4 persons per 100,000 annually.2
- GBS is an acquired peripheral nerve disease that can cause ascending symmetric paralysis, areflexia, decreased sensation, and respiratory compromise.2,3
- Miller Fisher Syndrome, a variant of GBS, presents with ophthalmiplegia often followed by ataxia and areflexia.2,3
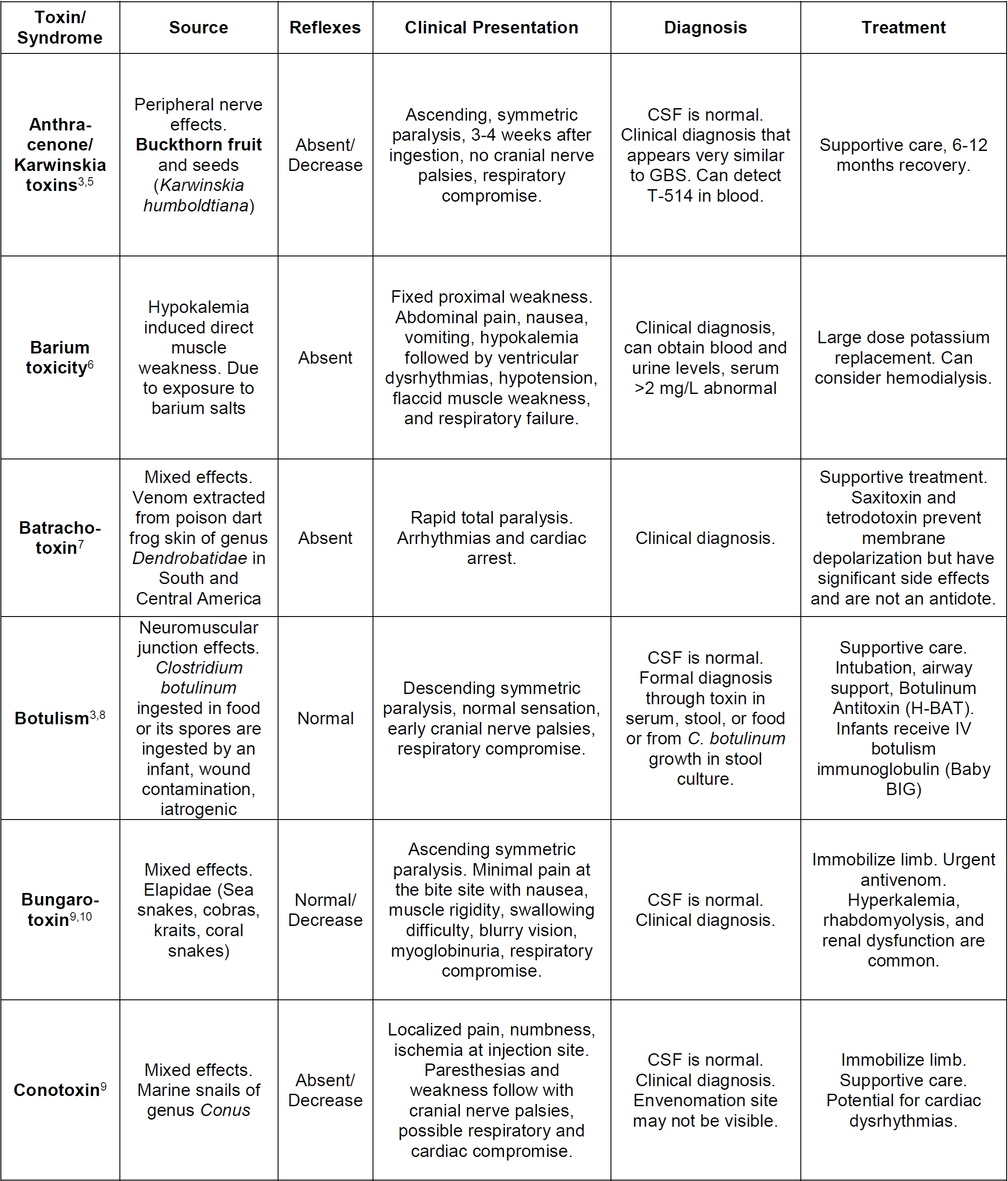
- The differential for causes of acute, symmetric paralysis include multiple toxicologic causes (See Table 1 below) and non-toxicologic causes (See List 1 below).
- Most heavy metal toxicities present with peripheral neuropathies as opposed to true paralysis. These metals include lead, arsenic, thallium, and mercury.4
Key Questions for Acute Paralysis:
- Has the patient had any recent illnesses, bites or stings, new foods, travel, or exposures?
- When was the onset of their symptoms?
- Does the patient have difficulty breathing, speaking, swallowing, double or blurry vision?
- What is the pattern of weakness? If it’s progressive, is it ascending or descending? Proximal or distal?

Non-toxicologic causes of symmetric paralysis3
-GBS, including Miller Fisher variant
-Myasthenia gravis
-Hypokalemia
-Hyperkalemia
-Hypermagnesemia
-Encephalitis
-Hypokalemic periodic paralysis
-Lambert Eaton myasthenic syndrome
-Spinal cord compression or injury
-Transverse myelitis
-Poliomyelitis
-Polymyositis
Main Points:
- Patients with acute symmetric paralysis should undergo a detailed history and physical addressing exposures, travels, time of onset, patterns of weakness, presence of bulbar palsies, and reflexes.
- Peripheral nerve involvement often presents with decreased reflexes and abnormal sensory exams.
- Neuromuscular junction involvement often present with intact reflexes and sensation.
- Botulism is frequently misdiagnosed and early recognition is critical as patients often progress to respiratory failure that may be prevented with the early administration of botulinum antitoxin.4
- Tick paralysis is a very rare condition but similarly can progress rapidly to respiratory failure until the tick is identified and removed.3
- Other toxicologic sources of paralysis encompass a broad array of foodborne toxins, envenomations, and chemical exposures.5
References:
- Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. 2016.
- McGillicuddy DC, Walker O, Shapiro NI, Edlow JA. Guillain-Barré syndrome in the emergency department. Ann Emerg Med 2006; 47:390.
- Geyer HL. Botulism. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds.Goldfrank’s Toxicologic Emergencies, 11e New York, NY: McGraw Hill.
- Staff NP, Windebank AJ. Peripheral neuropathy due to vitamin deficiency, toxins, and medications. Continuum (Minneap Minn). 2014;20(5 Peripheral Nervous System Disorders):1293–1306.
- Salazar-Leal ME, Flores MS, Sepulveda-Saavedra J, Romero-Diaz VJ, Becerra-Verdin EM, Tamez-Rodriguez VA, et al. An experimental model of peripheral neuropathy induced in rats by Karwinskia humboldtiana (buckthorn) fruit. Peripheral Nerv Syst. 2006;11:253–61
- Dawson, AH. Barium. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds.Goldfrank’s Toxicologic Emergencies, 11e New York, NY: McGraw-Hill.
- Albuquerque EX, Daly JW, and Witkop B. 1971. Batrachotoxin: chemistry and pharmacology. Science. 172:995–1002.
- Chatham-Stephens K, Fleck-Derderian S, Johnson SD, et al. Clinical features of foodborne and wound botulism: a systematic review of the literature, 1932–2015. Clin Infect Dis 2018; 66:S11–6.
- Ganti L, Rastogi V. Acute generalized weakness. Emerg Med Clin North Am. 2016;34(4):795–809.
- Ranawaka U.K., Lalloo D.G., Silva H.J. De Neurotoxicity in Snakebite—The Limits of Our Knowledge. PLoS Negl. Trop. Dis. 2013;7:e2302.
- Bowman WC. Neuromuscular block. Br J Pharmacol. 2006;147 Suppl 1(Suppl 1):S277–S286.
- Nelson LS, Goldfrank LR. Plants. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds. Goldfrank’s Toxicologic Emergencies, 11e New York, NY: McGraw-Hill; . http://accesspharmacy.mhmedical.com/content.aspx?bookid=2569§ionid=210276997. Accessed August 13, 2019.
- Blohm E, Brush E. Marine Envenomations. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds.Goldfrank’s Toxicologic Emergencies, 11e New York, NY: McGraw-Hill.
- Yen LM, Thwaites CL. Tetanus. Lancet. 2019 Apr 20;393(10181):1657-1668.
- Fil LJ, Tunik MG. Food Poisoning. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS. eds.Goldfrank’s Toxicologic Emergencies, 11e New York, NY: McGraw-Hill.




