
Authors: Zachary Boivin, MD (@ZachBoivinMD, Ultrasound Fellow, Yale University); Jia Jian Li, MD (@JjMDUS, Ultrasound Fellow, Yale University) // Reviewed by: Stephen Alerhand, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Introduction
Anytime a patient presents to the ED with abdominal pain, biliary pathology should be considered in the diagnosis.1 A biliary point-of-care ultrasound (POCUS) is the fastest and most accurate way to assess for biliary pathology, but it can be difficult to locate the gallbladder, as it is not a fixed organ.2, 3 Biliary POCUS can help decrease patient length of stay in the Emergency Department.4
Benefits of Biliary POCUS?
o Immediate identification of pathology
o Decrease time to disposition
o Decrease time to surgical consultation
o Cognitive unloading
o No radiation risks
o Ultrasound tech availability may be limited
Downsides to Biliary POCUS?
o Difficulty obtaining biliary views due to patient body habitus or pain
o Operator dependent
o Consultants requesting radiology performed ultrasound
How to Perform a Biliary Ultrasound
The preferred ultrasound probe for biliary ultrasound is the curvilinear probe due to its wider field of view and lower frequency. Prior to evaluating with POCUS, ask about prior cholecystectomy, and look for surgical scars. The patient should be positioned supine, with the probe marker cranial (longitudinal or sagittal orientation) in the subxiphoid region, sweeping along the subcostal margin, while rocking the probe to aim superior. Often, you will see bowel gas, which is an indication you are too inferior.5
[videopress G0aojbLD]
Video 1: Subcostal Sweep
Improved imaging can be achieved by asking the patient to inhale deeply or by turning them onto a left lateral decubitus position, which brings the hepatobiliary structures closer to the abdominal wall for better visualization.6
For patients with larger body habitus, the “X minus 7” approach involves placing the probe on the xiphoid (X) process in a transverse view and moving 7 centimeters to the patient’s right.7
[videopress 8AbDniFW]
Video 2: X minus 7 approach
If the gallbladder is still unable to be identified, attempting a coronal approach where Morison’s pouch and the right kidney is identified, with the probe marker facing cranial, and then moving anterior on the patient, approaching the anterior axillary line, until biliary anatomy comes into view.
[videopress vQHkaOra]
Video 3: Coronary approach to the gallbladder
POCUS Findings
Sonographically, the gallbladder is situated in the right upper quadrant as an elongated pear-shaped organ on the inferior surface of the liver. It consists of three main parts: the fundus, body, and neck. The fundus is the rounded distal portion, the body is the primary portion, and the neck is the narrow end connecting to the cystic duct.8
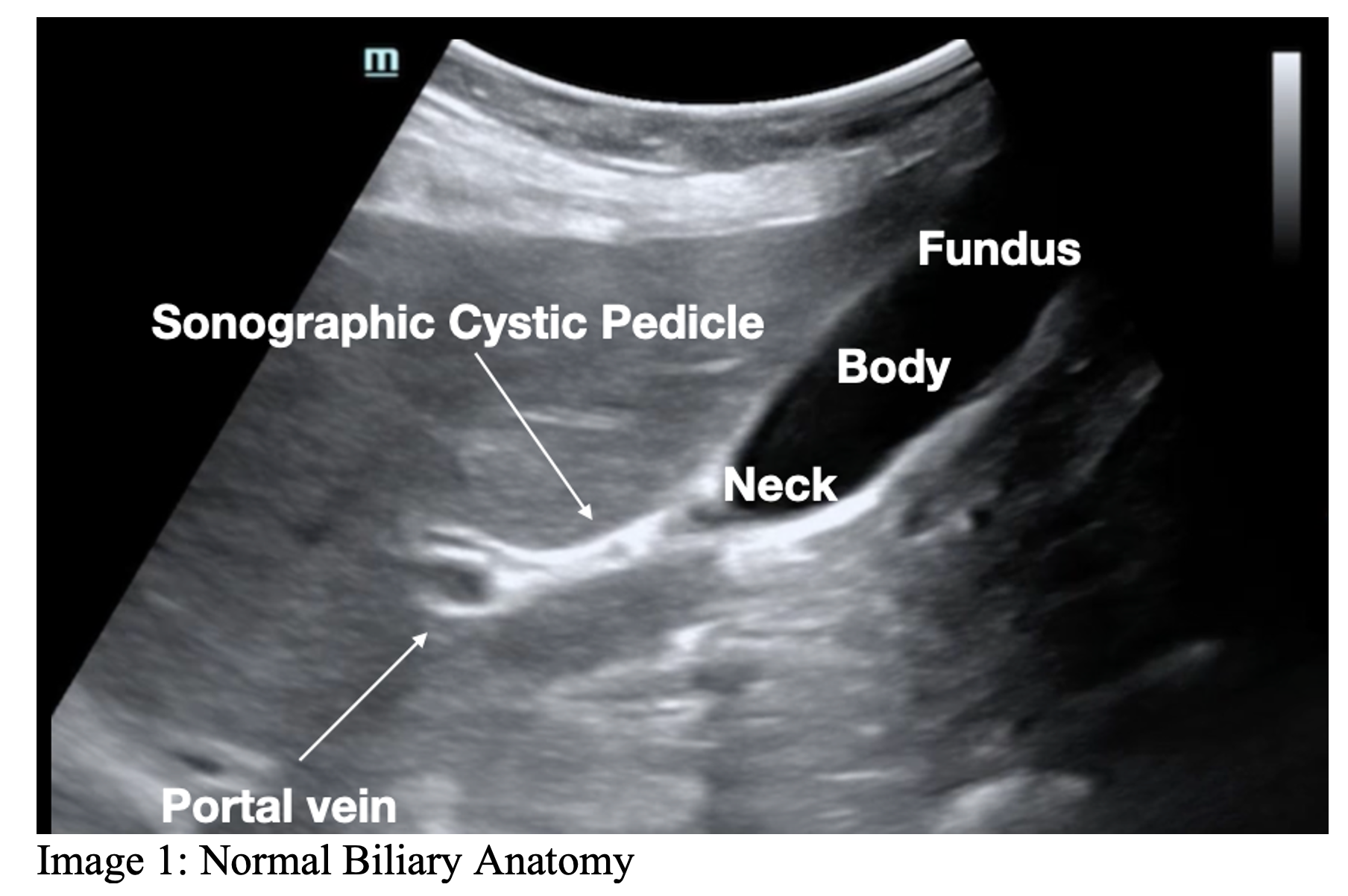
The sonographic cystic pedicle serves as a hyperechoic landmark in the right upper quadrant, present in approximately 70% of individuals. Recognizing these sonographic landmarks is crucial to avoid mistaking the duodenum for the gallbladder.9 Visual peristalsis, occurring only in the duodenum and not the gallbladder, can be an additional aid in differentiation.
[videopress i1ygLdNq]
Video 4: Duodenum and Gallbladder
After a short distance, the cystic duct joins the common hepatic duct to form the common bile duct (CBD), usually coursing with the hepatic artery and the portal vein, which serves as one of the primary landmarks for the gallbladder. The walls of the portal vein are hyperechoic, making it stand out compared to other hepatic vasculature. The portal triad containing the portal vein, hepatic artery, and CBD, is important to locate during a biliary POCUS. Another way to find the portal triad is to find the portal vessels within the hepatic vasculature (they have thicker hyperechoic walls in comparison to the thin-walled hepatic vessels that drain to the IVC), and track those portal vessels to the portal vein.

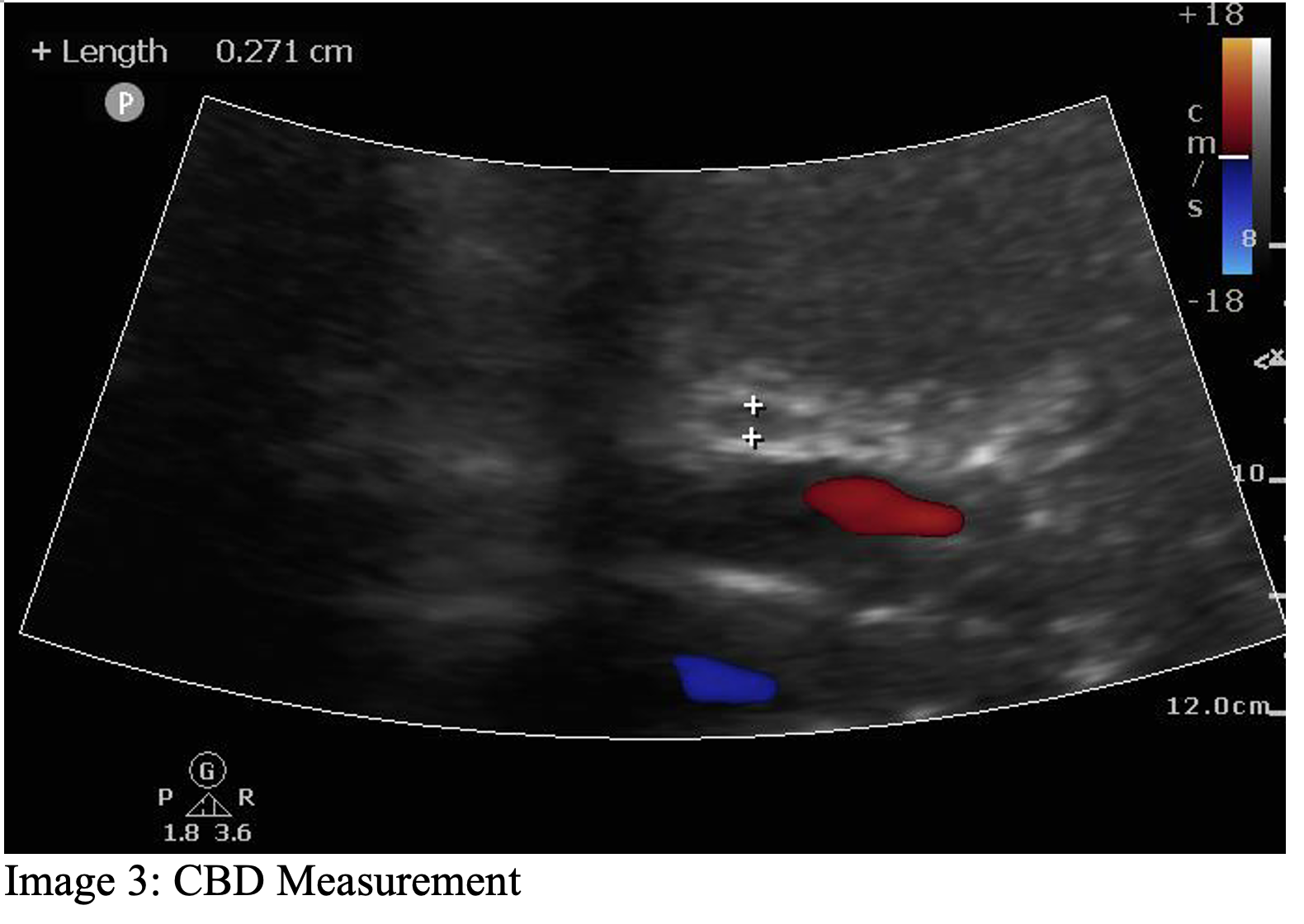
The CBD can be difficult to visualize at times. It sits anterior to the portal vein, and can be further identified through color Doppler, which will not have a Doppler signal over the CBD. The CBD should be measured as part of biliary POCUS if identified, and it is measured from inside to inside. The normal size of the CBD varies with age, with normal being up to 6 mm in patients below the age of 70. Once patients reach 70 years old, the normal CBD increases at a rate of 1 mm per year, meaning that a normal 70-year-old patient has up to a 7 mm CBD, an 80-year-old has up to an 8 mm CBD, etc.5, 10, 11 The CBD can also be dilated up to 1 cm after a cholecystectomy.
[videopress 8AbDniFW]
Video 5: CBD with Doppler flow applied
Another measurement needed for a complete biliary POCUS is a measurement of the gallbladder wall. The normal gallbladder wall appears as a pencil-thin line, with 3 to 4 mm being the upper limit of normal thickness for the anterior gallbladder wall. The anterior wall, closest to the transducer footprint, is measured due to an artifact called posterior acoustic enhancement leading to an artificially thick appearance of the posterior gallbladder wall.5

Pearls:
- Use the portal vein and sonographic cystic pedicle to help identify the gallbladder
- Beware the duodenum, look for visible peristalsis and landmarks to ensure the gallbladder is being visualized
- Use patient positioning to improve your image, asking the patient to move into the left lateral decubitus, or asking them to take a deep breath and hold
- Always use the same three-step process to find the gallbladder
Summary:
A three-step process to help identify the gallbladder:
- Start in the sagittal plane (indicator facing the head) with the probe under the subxiphoid, go down the costal margin
- Then go back to the starting position and go straight across the ribs, often traveling 7cm or more laterally towards the patient’s right
- Obtain the coronal view of the kidney (as you would for a FAST exam) and then move the probe anteriorly, going at least to the anterior axillary line if not even more anterior
- Identify the portal vein and the sonographic cystic pedicle
Help improve your image:
- Left lateral decubitus position
- Deep breath and hold
Video Resources:
- ACEP Sonoguide: https://www.acep.org/sonoguide/basic/gallbladder
- POCUS Atlas: https://www.thepocusatlas.com/hepatobiliary
- 5 minute sono – https://coreultrasound.com/gallbladder/
References:
- Woo MY, Taylor M, Loubani O, Bowra J, Atkinson P. My patient has got abdominal pain: identifying biliary problems. Ultrasound. 2014;22:223-228.
- Ross M, Brown M, McLaughlin K, et al. Emergency physician-performed ultrasound to diagnose cholelithiasis: a systematic review. Acad Emerg Med. 2011;18:227-235.
- Dumbrava BD, Bass GA, Jumean A, et al. The Accuracy of Point-of-Care Ultrasound (POCUS) in Acute Gallbladder Disease. Diagnostics (Basel). 2023;13.
- Blaivas M, Harwood RA, Lambert MJ. Decreasing length of stay with emergency ultrasound examination of the gallbladder. Acad Emerg Med. 1999;6:1020-1023.
- Ma OJ, Mateer JR, Reardon RF, Joing SA. Ma and Mateer’s Emergency Ultrasound, 3e. New York, NY: The McGraw-Hill Companies; 2014.
- Conrad MR, Leonard J, Landay MJ. Left lateral decubitus sonography of gallstones in the contracted gallbladder. AJR. American journal of roentgenology. 1980;134:141-144.
- Al-Khouja F, Mazumder P, Moeller J, Lahham S. A Case Report on Detecting Porcelain Gallbladder form Wall-Echo-Shadow Sign on Point-of-Care Ultrasound. J Educ Teach Emerg Med. 2021;6:V25-v29.
- Jones MW, Small K, Kashyap S, Deppen JG. Physiology, Gallbladder. StatPearls. Treasure Island (FL): StatPearls PublishingCopyright © 2024, StatPearls Publishing LLC.; 2024.
- Yang FJ, Kohen B, Sanapala S, Halperin M. A Potential Pitfall in POCUS of the Gallbladder: Beware of the Duodenum. Pocus j. 2022;7:188-189.
- Lahham S, Becker BA, Gari A, et al. Utility of common bile duct measurement in ED point of care ultrasound: A prospective study. Am J Emerg Med. 2018;36:962-966.
- Bowie JD. What is the upper limit of normal for the common bile duct on ultrasound: how much do you want it to be? Am J Gastroenterol. 2000;95:897-900.





1 thought on “Using Point-of-Care Ultrasound to Identify the Gallbladder”
Pingback: Zedu Weekly Wrap - 29 March 2024