ECG pointers: The Barcelona Criteria
- Oct 13th, 2021
- Brannon Inman
- categories:
Authors: Brannon Inman (EM Resident, San Antonio, TX) and Lloyd Tannenbaum (EM Attending Physician, San Antonio, TX) // Reviewed by: Jamie Santistevan, MD (@jamie_rae_EMdoc, EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD (@MPrizzleER); and Brit Long, MD (@long_brit)
The Case:
An 89-year-old man with a history of prior inferior myocardial infarction, chronic LAD occlusion and with Left Inferior Mammary Artery (LIMA) vessel bypass grafting, s/p ICD placement in 2005 presents complaining of chest pain “just like my last heart attack”.
As an astute clinician you obtain an ECG:

Figure 1: Adapted from: Making Sense of Sgarbossa’s Criteria – Chest Pain and Left Bundle Branch Block – Part 1: ECGMedicaltraining.com
Well that’s excellent, a left bundle. Luckily you recall Sgarbossa’s criteria like the back of your hand. *Quickly opens Google*
Ah yes… Sgarbossa’s criteria:
- Concordant ST elevation in any lead ≥ 1mm (5 points)
- Concordant ST depression in Leads V1-3 ≥ 1mm (3 points)
- Excessive discordance ≥ 5 mm (2 points)
≥ 3 points are need to diagnose an acute myocardial infarction.
These criteria were first described by Dr Elena Sgarbossa in 1996. Prior to these publications the common thought was that you could not diagnose electrocardiographic acute myocardial infarction (AMI) in those with a left bundle branch block. These criteria were a game changer and were determined to be highly specific for the diagnosis of AMI. During the initial derivation study the specificity was 90%, with a specificity of 96% during the validation study. Sensitivity was determined to be 78% during the derivation study. However, the validation trial showed the sensitivity to be closer to 36%. 1,2Essentially, this means that if the criteria are met the patient is very likely to have an occlusive myocardial infarction (high specificity). However, with the external validation criteria showing sensitivity in the mid-30’s, you simply can’t rule out an occlusive myocardial infarction if the criteria are absent.
So… lets apply these criteria to the patient above. Any concordant ST elevation? No. Any concordant ST Depression in the precordial leads (V1-3)? No. Excessive discordance alone doesn’t meet Sgarbossa’s criteria and we can’t diagnose acute myocardial infarction based off the third criteria alone. But this is a moot point since it’s not present on this EKG anyway.
The patient is still sitting there clutching his chest and diaphoretic. Your index of suspicion for a cardiac cause of his pain remains high, as your patient has an undeniable Levine’s sign.
You recall there’s a modified Sgarbossa’s criteria or “Smith Criteria”.
Smith Criteria
- Concordant ST elevation in any lead ≥ 1mm
- Concordant ST depression in Leads V1-3 ≥ 1mm
- Excessive discordance ST:S Ratio ≤ – 0.25
The Smith criteria was first derived in 2012 and later validated in 2015. In the validation and the scoring proposed was “unweighted”, meaning that only one of the 3 need to be positive to diagnose an AMI. During the derivation study Smith et. al.’s data suggested a sensitivity of 91%, and a specificity of 90%.3During the validation trial the sensitivity was 80%, with a specificity of 99%. 4Meaning these criteria, when positive, is very likely to correctly identify an occlusive AMI, but will still miss a few.
We established earlier that this patient’s ECG didn’t meet the first two criteria of Sgarbossa’s criteria. Since the first two criteria are the same in the original and modified criteria we can safely concentrate our attention to criteria 3. Are there any leads where excessive discordance is seen?
No… not really.
Still not buying the elderly man with a strong cardiac history in 33 clutching his chest with index chest pain is not having an AMI? You would likely be correct in your suspicion. As we have reviewed, the specificity of these criteria is quite high. Meaning if the ECG is positive the patient is likely to have an AMI. However the sensitivity is somewhere between ok and not-that-great. That’s fancy talk for: just because they don’t meet the criteria doesn’t mean they’re not infarcting their myocardium.
Well as of 2020 there’s a new kid on the block.
The New Kid on the Block
Barcelona Criteria:
- Concordant ST elevation in any lead ≥ 1mm
- Concordant ST depression in any lead
- Discordant ST deviation ≥ 1mm in any lead where the R or S is ≤ 6mm.
As with the prior 2 criteria, criteria 1 is the same. Criteria 2 is expanded to all leads (not just V1-3). Criteria 3 is a bit unique. For the BARCELONA criteria excessive discordance (criteria 3) is defined as a deviation of ≥ 1mm in any lead with a dominant R or S wave ≤ 6 mm. So, for criteria 3 you are primary looking at low voltage leads.For example, if there were a lead, any lead, with an R wave of 5mm, with discordant elevation of 1mm this would meet criteria. Like the Smith criteria, these criteria is unweighted meaning meeting 1 of the criteria is diagnostic of an AMI.

Figure 2: Excerpt from New Electrocardiographic Algorithm for the Diagnosis of Acute Myocardial Infarction in Patients With Left Bundle Branch Block displaying criteria 3
In the study of the BARCELONA criteria the sensitivity and specificity were 93% and 94%, respectively. 5The BARCELONA criteria has been derived and internally validated (i.e. validated at the institution it was derived), but has not been externally validated.
Now, let’s apply this to our patient:
- Concordant ST elevation in any lead ≥ 1mm
This is the same for the Sgarbossa, Smith and BARCELONA criteria. We already established our patient does not meet this one.
- Concordant ST depression in anylead
Unique to the BARCELONA criteria concordant depression now applies to ALL LEADS. If you look at lead V6 on our patients ECG you can see concordant depression of the ST segments.
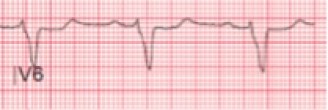
Figure 3: V6 showing concordant depression
Using the BARCELONA criteria, this patient would be captured, and diagnosed with AMI.
- Discordant ST deviation ≥ 1mm in any lead where the R or S is ≤ 6mm.
This patient does not have any low voltage leads ≤ 6mm, therefore this #3 cannot be applied. However, see figure 4 below, which shows an example ECG meeting this criterion:

Figure 4: Excerpt from New Electrocardiographic Algorithm for the Diagnosis of Acute Myocardial Infarction in Patients with Left Bundle Branch Block displaying criteria 3
This image displays 3 examples of leads meeting criterion #3 on the BARCELONA criteria.
Case wrap up:
You activate the Cath lab. While the cardiologist is apprehensive of the application of a new scoring system that has yet to be externally validated, they agree that your patient’s pre-test probability is very high. He is taken to the Cath Lab where he is determined to have an occluded segment of his left circumflex.
Main ECG Pointers:
- Both the Sgarbossa and Smith criteria are approved for use to diagnose AMI in LBBB
- The Barcelona criteria are new (published in 2020)
- Unique parts of the Barcelona criteria include applying concordant depression to all leads, and the application of excessive discordance to low voltage leads ≤ 6mm.
- The Barcelona criteria have been derived and internally validated with promising results. However, it awaits external validation.
- As always, when applying any clinical rules, always consider the patient’s pretest probability.
Resources:
- Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic Diagnosis of Evolving Acute Myocardial Infarction in the Presence of Left Bundle-Branch Block. http://dx.doi.org/101056/NEJM199602223340801. 2009;334(8):481-487. doi:10.1056/NEJM199602223340801
- Sgarbossa EB, Pinski SL, Gates KB, Wagner GS, Investigators TG-1. Early electrocardiographic diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm. American Journal of Cardiology. 1996;77(5):423-424. doi:10.1016/S0002-9149(97)89377-0
- SW S, KW D, TD H, DM D, LA P. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Annals of emergency medicine. 2012;60(6):766-776. doi:10.1016/J.ANNEMERGMED.2012.07.119
- HP M, AT L, EJ J, et al. Validation of the modified Sgarbossa criteria for acute coronary occlusion in the setting of left bundle branch block: A retrospective case-control study. American heart journal. 2015;170(6):1255-1264. doi:10.1016/J.AHJ.2015.09.005
- A DM, M R, J C, et al. New Electrocardiographic Algorithm for the Diagnosis of Acute Myocardial Infarction in Patients With Left Bundle Branch Block. Journal of the American Heart Association. 2020;9(14). doi:10.1161/JAHA.119.015573
