
Author: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDocs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 29-year-old female presents with generalized weakness and vision problems. She says her weakness is worse at the end of the day or with prolonged activity, and she experiences double vision as well. The symptoms also worsen with heat. She denies fevers, pain, nausea/vomiting, recent illnesses, or any other neurologic deficits, including paresthesias. She has no past medical or surgical history.
You find fatiguable muscle weakness in proximal motor groups, but sensation, gait, reflexes, and mental status are normal. What is the likely diagnosis, and what is your next step in evaluation?
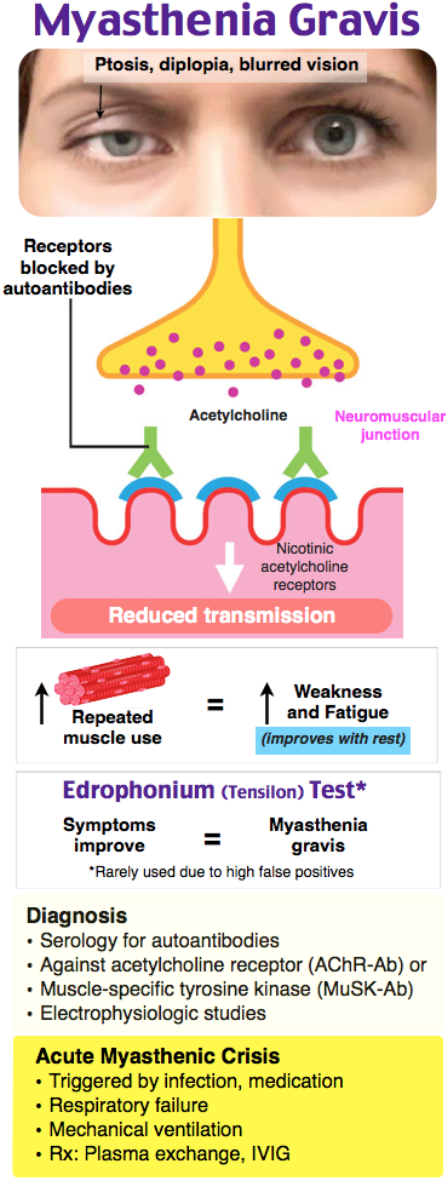
Answer: Myasthenia Gravis (MG)
Background: MG is the result of acetylcholine receptor blockade, degradation, and dysfunction by autoantibodies at the neuromuscular junction.
- Receptor dysfunction at the NMJ causes weakness.
- Up to 75% of patients have abnormal thymus, and a thymoma may be present.
- Affects < 0.7% of the population, most commonly in ages 20-40 and 50-70 years. Women are affected more commonly affected in the 20-40 year group, and men are more commonly affected in the older group.
- 5 classes of disease severity. Class 1 has ocular involvement only, with progressive weakness and dysfunction in higher classes.
Presentation:
- Generalized weakness is the most common symptom, typically of the proximal muscles, neck extensors, and facial/bulbar muscles (diplopia, ptosis, dysphagia, dysarthria).
- Ptosis is often the first symptom.
- Symptoms worsen with prolong muscle use, heat, stress, infection, and at the end of the day.
- There is usually no sensory, reflex, or cerebellar deficits. Patients should have normal gait, and they should also have normal mental status.
- Ask about recent illnesses, medication changes, toxin/drug exposure, trauma, new stressors.
- Myasthenic crisis (MC) is MG with respiratory failure.
- This is most commonly associated with infection, surgery, tapering of immunosuppressant medications, pain, pregnancy, medication changes, and poor sleep.
- MC is a clinical diagnosis.
- Evaluate respiratory status: look for weak cough, difficulty holding head up from bed, accessory muscle use, bulbar weakness, and single breath test (counting to 20 in a single breath). Patients should be able to count to 20 in a single breath. If they cannot, fear impending respiratory failure.
- Pulmonary functions tests such as forced vital capacity and negative inspiratory force can be used, but these require a good seal made by the patient, which can be difficult.
- Do not base need for intubation solely on assessment of pulmonary function tests. For more see the IBCC chapter.
- Stabilize with oxygen and noninvasive positive pressure ventilation.
- Autonomic dysfunction (irregular cardiac rhythms, tachycardia, bradycardia, hypotension, hypertension, urinary overflow or retention, diaphoresis, or anhidrosis)is unlikely in patients with MG and suggest another condition.
- In patients presenting with known MG, closely evaluate the medication list for any exacerbating agents (discussed below).
- Eculizimab (Soliris) is a medication used for control of MG. This medication reduces terminal complement production; however, it drastically increases risk of meningococcal infection, even after pre-therapy vaccination.
Differential:
- Consider other causes of general weakness and respiratory disease such as electrolyte imbalance, sepsis, stroke, thyroid disease, intracranial mass, botulism, Lambert-Eaton syndrome, intoxication, envenomation, Guillain–Barre syndrome (GBS), ALS, MS, hypoglycemia, ACS, syncope, arrhythmia, anemia.
- Drug induced MG: antibiotics (fluoroquinolones, aminoglycosides, clindamycin, macrolides, metronidazole), steroids, antiseizure, beta blockers, calcium channel blockers, opioids, haloperidol.
- To differentiate MG from other conditions, the 30-second neurologic exam can assist:
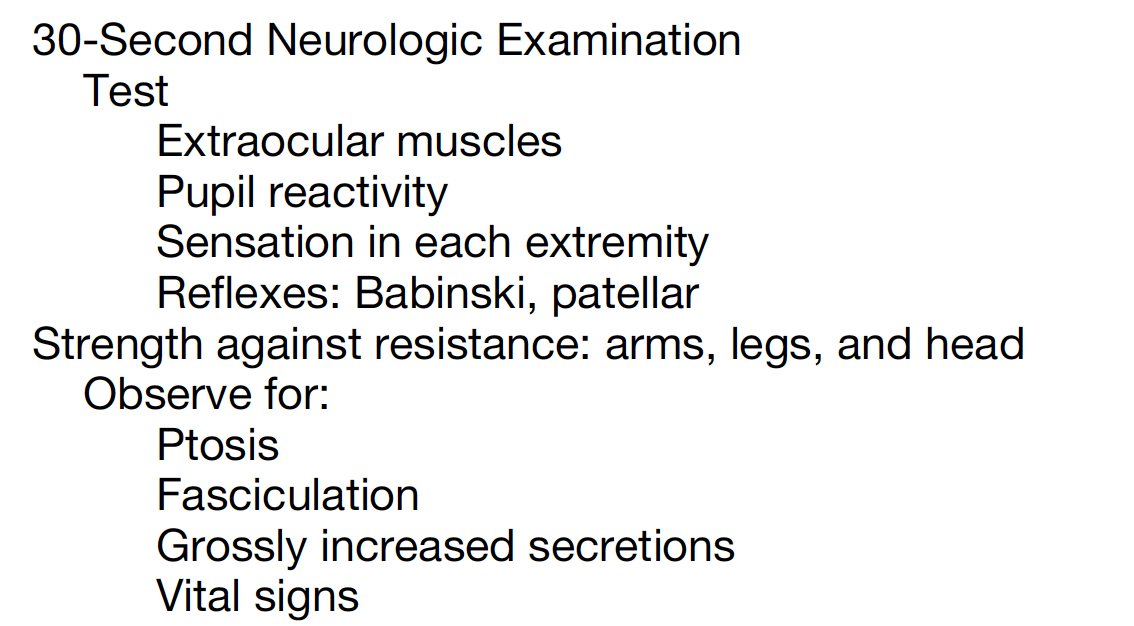
- Cholinergic crisis, due to excess anticholinesterase medication, is rare but presents with fasciculations, bradycardia, miosis, diarrhea, vomiting, and tearing.
ED Studies and Assessment:
- Base on differential and patient hemodynamic/respiratory status: CBC, TSH, renal and liver function, troponin, VBG, extended electrolytes, CK, urinalysis, hCG in females, ECG.
- Chest x-ray if respiratory symptoms are present.
- LP should be considered if spinal cord disease (GBS) is suspected.
- Edrophonium or neostigmine testing can improve muscle strength, but this is currently limited in the U.S. It may lead to respiratory failure, bradycardia, and cardiac arrest. There are also numerous false positives and false negatives.
- Electromyographic testing evaluates postsynaptic NMJ dysfunction.
Diagnosis:
- Serologic testing can assist, as 85% of cases are due to acquired antibodies, but there are a large number of receptor antibodies that can cause MG. Up to 55% of patients with ocular MG will have positive antibodies.
- Ice pack test can be used in patients with ptosis or ophthalmoparesis and MG, with sensitivity over 90%. Place an ice pack over the affected eye for 2 minutes and reassess. If there is a 2-mm improvement, the test is positive. However, over 20% of patients with MG do not have ocular symptoms.
Treatment: Goals include stabilize life-threatening condition, treat any underlying etiology of MC, and discuss with neurology.
- Consult neurology during initial stabilization.
- Treat any underlying condition and any associated infection and fever.
- Be wary of administering corticosteroid and magnesium infusions, which can worsen MC.
- Corticosteroids may be needed in treatment refractory cases with neurology consultation.
- Use NIPPV early for MC. If the patient fails NIPPV, is in respiratory failure, or is significantly altered, intubate with a non-depolarizing agent at smaller doses.
- Plasmapheresis and IVIG are cornerstones of therapy.
- For those with thymoma, thymectomy may be needed.
- Patients may require chronic immunosuppressive medications such as azathioprine, mycophenolate, cyclosporine, methotrexate, rituximab, or tacrolimus.
Disposition:
- Hospitalize patients with patients experiencing exacerbation with severe symptoms.
- ICU admission is recommended for patients with severe respiratory disease or severe bulbar weakness.
- Ventilatory support may be required for at least a week.
- Patients require close neurology follow-up.

A 35-year-old woman presents to the emergency department with complaints of fatigue, weakness, and shortness of breath. Symptoms started about a month ago when she began to have trouble keeping her eyes open towards the end of the day. Over the last few days she has noted overall weakness and shortness of breath. Vital signs including a respiratory rate of 16 breaths/minute and 96% SpO2. You note bilateral ptosis and clear lung sounds. Ice bags were applied to the eyes for two minutes. After the ice bags were removed, the distance between her upper and lower eyelids had improved by greater than 2 mm. Which of the following describes the pathophysiology of the most likely underlying diagnosis?
A) Autoimmune destruction of acetylcholine receptors on the postsynaptic membrane
B) Neurodegenerative lesion formation in the anterior horn cells
C) Toxin irreversibly bound to presynaptic membrane preventing acetylcholine release
D) Toxin reversibly bound at the presynaptic membrane preventing acetylcholine release
Answer: A
Myasthenia gravis is a rare disorder known for a bimodal onset, with the first peak among women 20 to 40 years of age and a second peak among men 50 to 70 years old. It involves autoimmune destruction of acetylcholine receptors on the postsynaptic membrane at the neuromuscular junction. This results in complement-mediated destruction of the total number of receptors along with autoantibodies competing with acetylcholine to bind to the remaining receptors. Therefore, with repeated stimulation and fewer sites available, fatigue develops. Fatigue and muscular weakness are the hallmarks of myasthenia gravis. Ocular symptoms are often the first manifestation, with ptosis worsening by the end of the day. Muscular weakness can also affect respiration along with the bulbar muscles causing dysarthria or dysphagia. The diagnosis is based on clinical findings and a combination of serologic testing, electromyographic testing, and the bedside edrophonium (tensilon) or ice bag tests. Myasthenic crisis is defined as respiratory failure leading to mechanical ventilation. Overall mortality has declined dramatically due to treatments with plasmapheresis, intravenous immunoglobulin, and corticosteroids.
Neurodegenerative lesion formation in the anterior horn cells (B) describes the pathophysiology of amyotrophic lateral sclerosis or Lou Gehrig disease. This degeneration produces purely motor symptoms early on, such as spasticity, hyperreflexia, weakness, and dysphagia, followed by later onset of intercostal muscle weakness and decreased forced vital capacity. Toxin irreversibly bound to presynaptic membrane preventing acetylcholine release (C) describes the pathophysiology of botulism. This, like myasthenia gravis, occurs at the neuromuscular junction. Symptoms include abdominal pain, nausea, vomiting, descending flaccid paralysis, diplopia, ptosis, dysphagia, and dysarthria and may lead to respiratory failure. Toxin reversibly bound at the presynaptic membrane preventing acetylcholine release (D) describes the pathophysiology of tick paralysis. This, like myasthenia gravis and botulism, occurs at the neuromuscular junction. There are 40 known tick species capable of producing ixovotoxin, which results in tick paralysis. Symptoms include ascending flaccid and symmetric paralysis. Symptoms resolve one to 24 hours following tick removal.
Further Reading:
emDocs – Elemental EM: MG
emDocs – Weakness
References:






3 thoughts on “EM@3AM: Myasthenia Gravis and Crisis”
Thanks to Dr. Dave Talan for pointing out an important consideration regarding MG medications:
Note that MG is now treated with a mab, eculizimab (Soliris) which reduces terminal complement production, and puts patients at crazy increased risk of meningococcal infection, even after pre-therapy vaccination. ED docs should be super careful in patients on this drug who present with infection symptoms.
Great point; thanks Dr. Talan!
Pingback: Weekly Update – 29 March 2021 – NewYork-Presbyterian Emergency Medicine
Pingback: Neuromuscular Disease in Emergency Medicine | EM Cases