EM@3AM: Thoracic and Lumbar Spine Trauma
- Mar 30th, 2024
- Luke Bailey
- categories:
Authors: Luke Bailey (Medical Student, Texas A&M SOM, Bryan, TX) and Scott Wieters, MD (Associate Dean Temple Campus, Texas A&M SOM, Temple, TX) // Reviewed by: Sophia Görgens, MD (EM Physician, Northwell, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 70-year-old female with a past medical history of osteoporosis, atrial fibrillation, and hypertension presents with acute thoraco-lumbar back pain after a ground-level fall. She was walking her dog who pulled her backwards, landing on her buttocks on the pavement. She denies any loss of consciousness, shortness of breath, chest pain, abdominal pain and denies any motor or sensory weakness.
Her vital signs are blood pressure 144/86, heart rate 88, SPO2 99%, temperature 36.8C, and a glucose of 138. Comprehensive physical exam is unremarkable, but she does have pain at the T-12/L-1 region of her back. She has full motor strength and sensory function in the lower extremities. Her patellar reflexes are 1+ bilaterally, no ankle clonus is noted, and she denies any saddle anesthesia or bowel/bladder incontinence.
CT of lower spine is ordered and shows the following:1

What is the diagnosis?
Answer: Thoracic and Lumbar Spine Trauma
Epidemiology:
- Approximately half of the vertebral injuries that are seen in the emergency department are thoracic and lumbar injuries.2-4
- Around 7% of all blunt trauma injuries include the thoracic and lumbar regions.2
- Males experience injuries to this region at an incidence of 3:1.3
- Males aged 16-30 experience the greatest number, with men older than 50 being the second highest risk group.3
- 40-45% occur due to motor vehicle accidents, 15-30% from falls, and 10-20% are from sports or leisure activities.3,4
- Risk factors include engaging in high energy activities, consumption of large amounts of alcohol, osteoporosis, and previous thoracic or lumbar fractures.5-7
Anatomy:
- The thoracic spine has 12 vertebrae (T1-T12), lumbar has five (L1-L5).
- Intervertebral disks lie between vertebrae and act as shock absorbers.
- The spinal canal houses the spinal cord.
- The spinal cord typically ends at the L2 level.8,9
- The spinal cord then continues as the cauda equina.
- Spinal roots exit the spinal cord bilaterally through intervertebral foramen and provide motor and sensory innervation to the abdomen/thorax (thoracic) or the lower limbs/pelvis (lumbar).8,9
- Two ligaments, the anterior and posterior longitudinal ligaments, run the length of the spine and allow for flexion and extension while providing overall stability.
- The ligamentum flavum attaches the vertebrae together.
- A multitude of muscles attach to the thoracic or lumbar spine, most of which aid in either movement or maintaining posture.
- Thoracic examples include erector spinae, latissimus dorsi, trapezius.8
- Lumbar examples include erector spinae, interspinales, psoas major.9


Clinical Presentation:
- Mechanism of injury is typically a trauma event including a hard impact.
- Most commonly motor vehicle accidents for younger patients, falls for older patients.
- Symptoms vary depending on severity of injury
- Common symptoms include diffuse back pain, tenderness to palpation, pain with movement.
- Severe injuries may present with ambulatory difficulties or motor/sensory deficits if the spinal cord is affected.
Evaluation:
- History is necessary to determine the mechanism of injury.
- Comprehensive Physical Exam
- Primary and secondary trauma survey should be performed.
- Evaluate for spinal trauma with tenderness, deformities.
- Assess for any motor or sensory deficits indicating spinal cord impairment.
- Rectal/vaginal assessment to check for hemorrhaging, spinal cord injury, or any underlying injuries not noticed superficially.10
- Spinal Fracture Classification11
- There are multiple different classification systems available.
- For emergent scenarios the patient can be classified as stable, potentially unstable, and unstable.
- Stability is determined by radiographs, CT scan, neurological status, and clinical status.
- Stable: mild pain, able to ambulate, no neurological deficits
- Potentially Unstable: mild to moderate pain, minor radicular symptoms, none to mild neurological deficits
- Unstable: severe pain, little to no ambulation, significant neurological deficits. Easily visible on imaging with severe defects.
- Imaging
- AP and lateral radiographs of thoracic and lumbar regions may be used to evaluate the integrity of vertebrae.12
- The sensitivity and specificity of thoracic radiographs are 55% and 94%, respectively.13
- The sensitivity and specificity of lumbar radiographs are 84.8% and 100%, respectively.14
- CT is the imaging modality of choice and indicated for definitive clarification of injury; it can specify the type of injury and assist with definitive management.
- Consider CT scan in potentially unstable or unstable patients as defined above.
- MRI is recommended if there are any neurologic deficits on examination.
- AP and lateral radiographs of thoracic and lumbar regions may be used to evaluate the integrity of vertebrae.12
Treatment:
- Stable Injuries
- No surgery needed.
- Manage pain and stabilize the affected area with a brace for patient’s comfort and also to prevent further damage.
- Potentially Unstable Injuries
- Surgery needed if there are deformities, inability to walk, or spinal cord involvement.
- Non-surgical injury is same as stable injury, in addition with close follow up to make sure new symptoms do not arise.
- Consult orthopedic spine surgeon or neurosurgeon if neurological deficits are present.
- Unstable Injuries
- Immediate surgical intervention is necessary to repair and immobilize the injured site.
- Follow up with orthopedic spine surgeon or neurosurgeon for longitudinal care.
Disposition:
- Patients should be referred to orthopedic spine surgeon or neurosurgeon if stable or minor potentially unstable.
- Patients may also be referred to physical therapy if necessary.
- If surgery is performed, admission and follow up with the surgeon is recommended.
Pearls:
- Determining the mechanism of injury early will help guide proper management.
- Neurological exam is necessary to assess for deficits.
- Diagnosis includes imaging.
- If injury is deemed unstable, immediate stabilization and surgical intervention is required.

A 27-year-old man was brought into the emergency department via EMS after being stabbed. On exam, the patient has a 2 cm stab wound to the left side of his back, just medial to the midline of T7. He is unable to move the left lower extremity, but his sensation is intact. He can move the right lower extremity but is unable to feel pain or temperature changes in that leg. He has normal rectal tone. What spinal cord syndrome is present?
A) Anterior cord syndrome
B) Brown-Séquard syndrome
C) Conus medullaris syndrome
D) Posterior cord syndrome
Answer: B
Brown-Séquard syndrome, one of the three most common incomplete spinal cord lesions, results from a penetrating injury to the spine or, more rarely, a cervical spine lateral mass fracture. This mechanism results in a hemisection of the spinal cord. It involves the dorsal column, corticospinal tract, and spinothalamic tract unilaterally. Exam findings include ipsilateral loss of motor function, vibration, and positional awareness, with contralateral loss of pain and temperature sensation.
CT remains the imaging modality of choice for the emergent evaluation of spinal injuries in trauma. However, it does not provide detailed information about the specific neurologic changes associated with Brown-Séquard syndrome. MRI provides a more detailed visualization of the spinal cord and surrounding structures to allow for the identification of abnormalities causing the syndrome.
Treatment involves initial stabilizing of the spine, managing pain, addressing associated injuries, and performing emergent neurosurgical consultation. Medications, rehabilitation, and assistive devices are the mainstays of treatment. Surgical intervention may be considered for cases with structural compressions or spinal instability. Most patients will regain ambulation and contralateral motor function. The prognosis depends on the extent and location of the injury, the individual’s overall health, and the effectiveness of treatment.

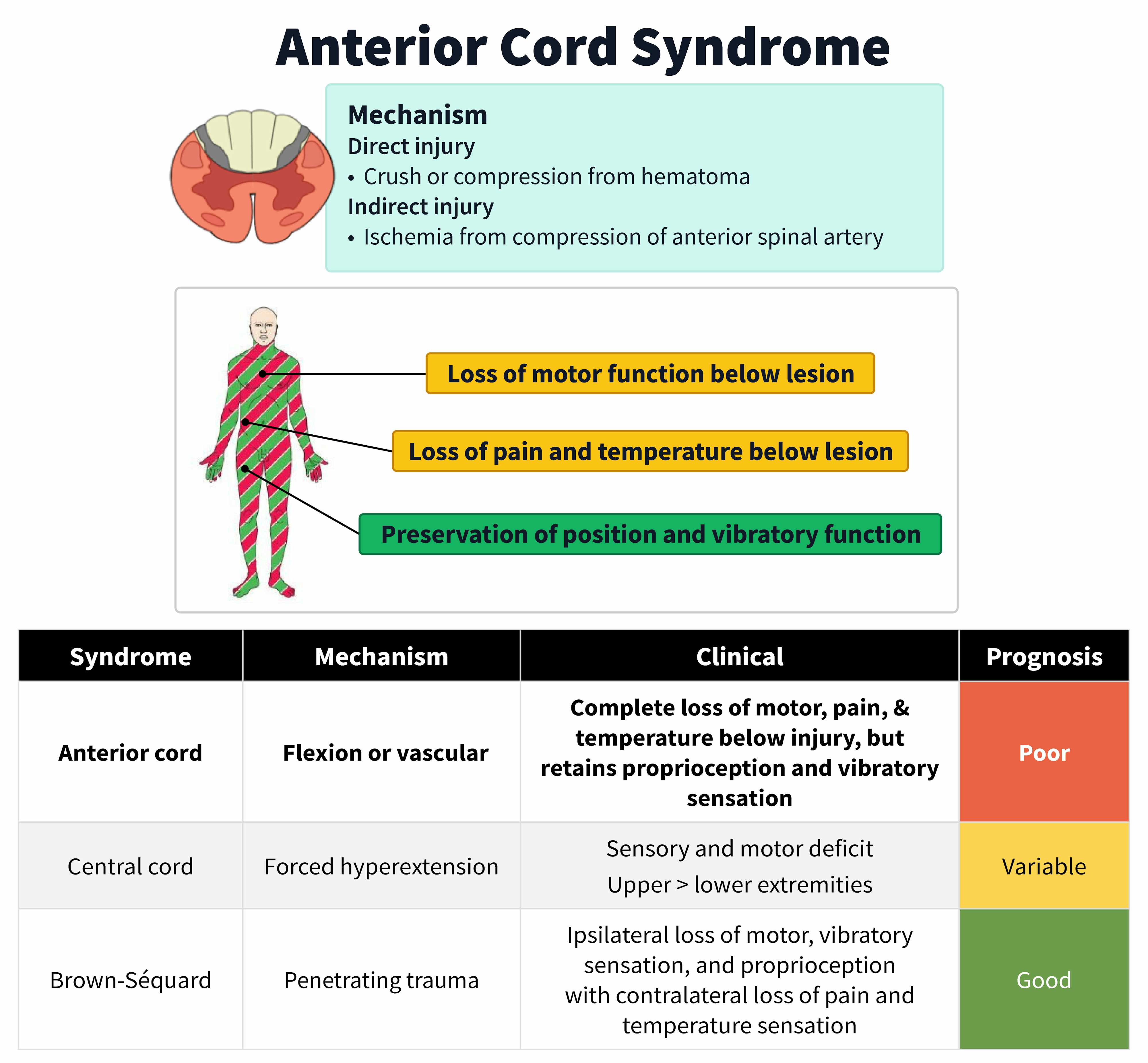
Anterior cord syndrome (A) presents with bilateral loss of motor function and pain and temperature sensation with intact tactile, position, and vibratory sensation. These findings are not consistent with the patient’s physical exam of unilateral weakness with contralateral pain and temperature sensation losses.
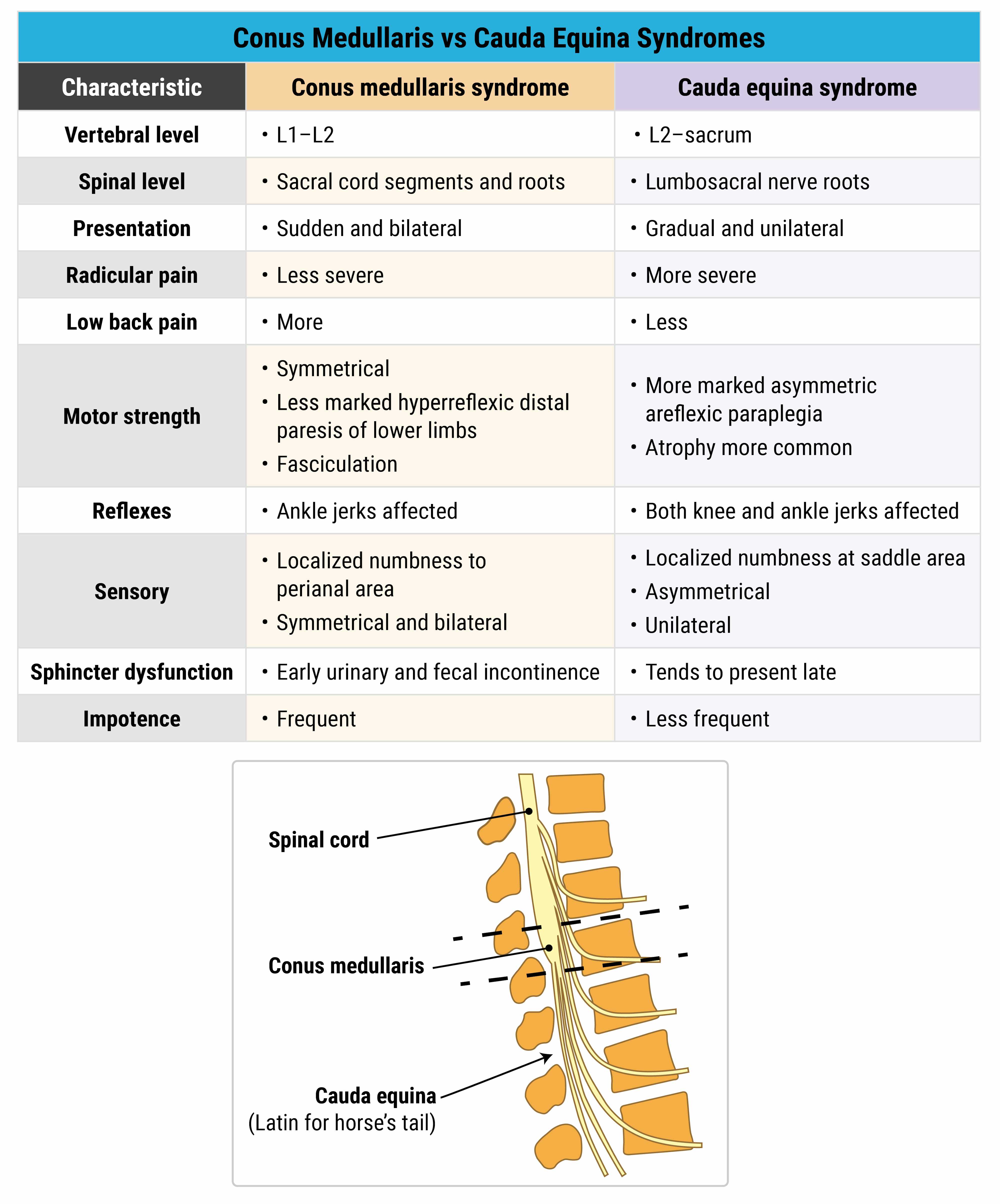
Conus medullaris syndrome (C) involves the vertebral level of L2 and the conus medullaris. Symptoms include flaccid paralysis of the bladder and rectum, saddle anesthesia, and impotence. Leg weakness may be mild if the lumbar nerves are spared. This patient has normal rectal tone and unilateral leg weakness, which is not a typical presentation of conus medullaris syndrome.
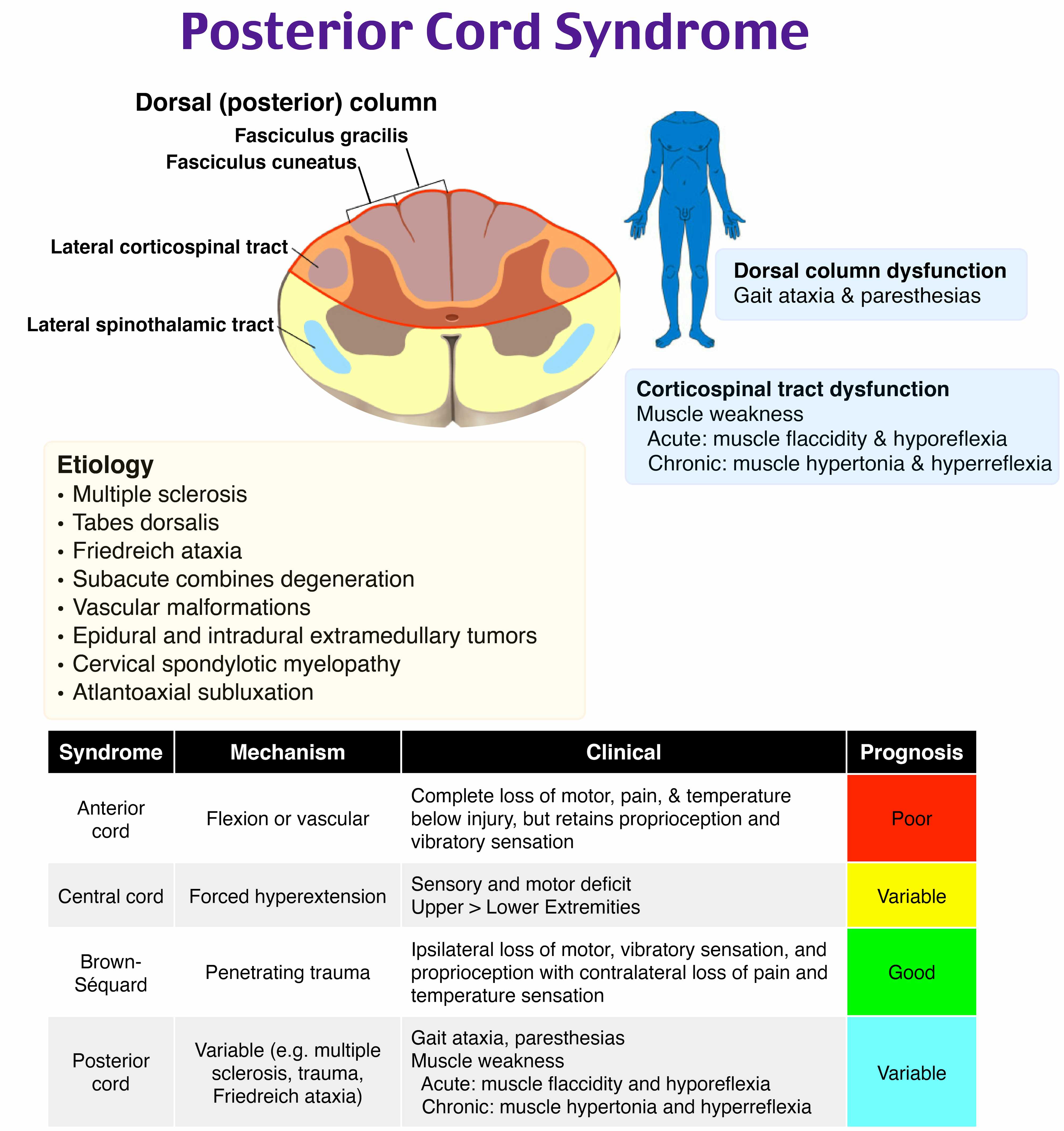
Posterior cord syndrome (D) features loss of proprioception and vibratory sensation, which may cause symptoms of ataxia and impaired body movements. Unlike other types of spinal cord injuries, posterior cord syndrome typically spares motor function and pain sensation. This patient has unilateral weakness, which is atypical of posterior cord syndrome.
References:
- Evan Mah Bs (Kin), Brent Burbridge M. Spine fracture. Undergraduate Diagnostic Imaging Fundamentals. September 30, 2017. Accessed June 23, 2023. https://openpress.usask.ca/undergradimaging/chapter/spine-fractures/.
- VandenBerg J, Cullison K, Fowler SA, Parsons MS, McAndrew CM, Carpenter CR. Blunt Thoracolumbar-Spine Trauma Evaluation in the Emergency Department: A Meta-Analysis of Diagnostic Accuracy for History, Physical Examination, and Imaging. J Emerg Med. 2019;56(2):153-165. doi:10.1016/j.jemermed.2018.10.032
- Charles YP, Steib JP. Management of thoracolumbar spine fractures with neurologic disorder. Orthop Traumatol Surg Res. 2015;101(1 Suppl):S31-S40. doi:10.1016/j.otsr.2014.06.024
- Kumar S, Kumar P, Patralekh MK, Srinivasan R, Agarwal A, Boruah T. Fracture-dislocation of the thoracolumbar spine without neurological deficit: a report of two cases and literature review. Spinal Cord Ser Cases. 2020;6(1):67. Published 2020 Jul 29. doi:10.1038/s41394-020-0315-4
- Tian F, Tu LY, Gu WF, et al. Percutaneous versus open pedicle screw instrumentation in treatment of thoracic and lumbar spine fractures: A systematic review and meta-analysis. Medicine (Baltimore). 2018;97(41):e12535. doi:10.1097/MD.0000000000012535
- Samelson EJ, Hannan MT, Zhang Y, Genant HK, Felson DT, Kiel DP. Incidence and risk factors for vertebral fracture in women and men: 25-year follow-up results from the population-based Framingham study. J Bone Miner Res. 2006;21(8):1207-1214. doi:10.1359/jbmr.060513
- Itodo OA, Flueck JL, Raguindin PF, et al. Physical activity and cardiometabolic risk factors in individuals with spinal cord injury: a systematic review and meta-analysis. Eur J Epidemiol. 2022;37(4):335-365. doi:10.1007/s10654-022-00859-4
- Waxenbaum JA, Reddy V, Futterman B. Anatomy, Back, Thoracic Vertebrae. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 8, 2022.
- Waxenbaum JA, Reddy V, Futterman B. Anatomy, Back, Lumbar Vertebrae. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 1, 2022.
- Whitney E, Alastra AJ. Vertebral Fracture. In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 3, 2023.
- Joaquim AF, Patel AA, Schroeder GD, Vaccaro AR. A simplified treatment algorithm for treating thoracic and lumbar spine trauma. J Spinal Cord Med. 2019;42(4):416-422. doi:10.1080/10790268.2018.1433267
- Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: An overview. Indian J Orthop. 2015;49(1):72-82. doi:10.4103/0019-5413.143914
- Inaoka T, Ohashi K, El-Khoury GY, Singh H, Berbaum KS. Clinical role of radiography for thoracic spine fractures in daily practice in the MDCT era: a retrospective review of 255 trauma patients. Jpn J Radiol. 2012;30(8):617-623. doi:10.1007/s11604-012-0097-0
- Esmailiejah AA, Abbasian M, Bidar R, Esmailiejah N, Safdari F, Amirjamshidi A. Diagnostic efficacy of clinical tests for lumbar spinal instability. Surg Neurol Int. 2018;9:17. Published 2018 Jan 25. doi:10.4103/sni.sni_359_17

{kind=link}
{kind=link}
{kind=link}