
Authors: Carolina Camacho-Ruiz, MD and Mark Silverberg, MD (Kings County Hospital/SUNY Downstate Emergency Medicine Department) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
A 57-year-old male with past history of HTN, CAD, and cocaine abuse is brought in by EMS with a fever of 102 °F. Upon questioning, the family mentions decreased PO intake in the last week, decrease urinary output, cough, and several episodes of non-bilious, non-bloody emesis. The cough is productive and worsening. Vital signs upon arrival are 102.5 F, 120 bpm, 23 RR, BP of 120/60, and O2% 95. The patient is conversant but appears toxic. You decide to activate a sepsis code, start your 30 ml/kg IVF bolus, antipyretics, draw labs included in the sepsis protocol, and initiate broad-spectrum antibiotics.
Lab results demonstrate a lactate of 1.5 mmol/L. Clearly something is wrong; that result cannot be real, as the patient appears toxic. You decided to send it again, and this time it returns at 1.4 mmol/L. What could be going on?
Lactate production

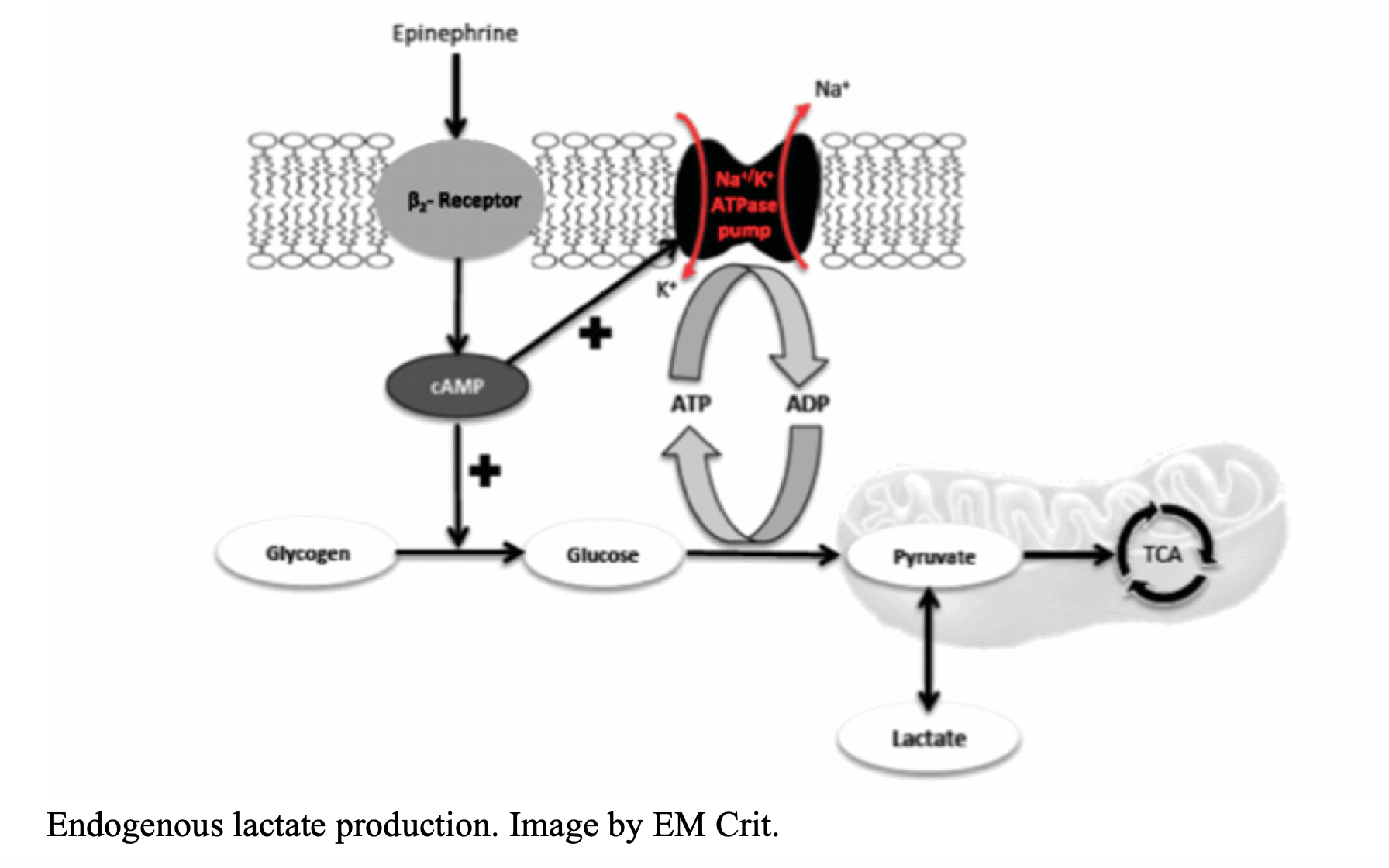
Our body is smart; we possess multiple compensatory systems that act under stress. In the past, lactate was thought to simply be the result of anaerobic metabolism, which occurs when compensatory mechanisms fail to correct an imbalance between tissue oxygen supply and demand. In other words, an increase in lactate was attributed to tissue hypoperfusion. As lactate increases, the patient’s risk of death increases. (1) But there is a new school of evidence that shows that lactate elevation in sepsis seems to be due to endogenous epinephrine stimulating beta-2 receptors. This is especially important in skeletal muscle cells. Adrenergic stimulation up regulates glycolysis, generating more pyruvate than can go to the TCA cycle (or Krebs cycle) in the cell’s mitochondria. This is an entirely aerobic process. (2) Lactate generation occurs because the TCA cycle is not able to keep up with the rapid rate of glycolysis and the metabolic needs of a body in acute decompensation. (3) The lungs and leukocytes may serve as additional sources of lactate. Evidence has demonstrated increases in lactate as a result of acute lung injury in the absence of tissue hypoxia. Furthermore, leukocytes, which are upregulated during sepsis, generate lactate during phagocytosis. (4) Thus, lactate is a measure of a stress response with serum catecholamines. Asthma, seizure, sepsis, exercise… all result in lactate generation.
But why is the lactate normal and my patient critically ill?
Clearance, excretion, and reabsorption
Liver, kidney, and myocardium can all consume the increased lactate during times of stress. The rate of hepatic clearance increases linearly with the production of lactate, no matter the etiology of hyperlactemia. This increase in lactate breakdown can increase up to seven-fold. (5) In addition, mitochondria-rich tissues such as skeletal muscles, myocardium, and renal proximal tubule cells remove additional lactate by converting it to pyruvate. Another possible reason for a lower than expected lactate in a septic patient is that acidosis not only increases hepatic lactate metabolism, but it also increases lactate uptake and utilization by the kidney. Patients with significant liver disease or liver failure cannot clear lactate to the same extent normal patients can. This balance is disrupted with worsening acidosis, systemic infection, and cardiovascular collapse. (6-8)

Lactate as a substrate
When the body is not in shock, the mitochondria can metabolize lactate and use it as fuel. Lactate can be used as a source of energy in multiple organs in our body including the brain, heart, liver, kidney, and muscles when our normal aerobic metabolism fails us. The problem arises when the oxidative system shuts down due to inadequate oxygen supply compared to demand, iatrogenic causes, and drug induced causes. In this situation, the mitochondria will become a lactate producing, rather than consuming, tissue. (7,8)
Beta adrenergic blocking agents
Multiple studies suggest the production of lactate is multifactorial rather than only due to tissue hypoxia and tissue perfusion. One example is beta adrenergic stimulation contributing to increased lactate production. With this in mind, what about beta adrenergic blocking agents? A recent study mentions that the rise in lactate may be blunted in a septic patient using beta blockers such as metoprolol. (8-10)
Decreased lactate as endpoint for resuscitation
Lactate is a very complex molecule. It is a substrate, an energy source, and a marker of stress. (8) Due to the complex biochemistry of this molecule, it is difficult to classify a patient as sick or not sick just based in a lactate level. Lactate clearance is probably good, with a high negative predictive value for mortality, but it does not have a high positive predictive value. Aggressive resuscitation following the guidelines aiming at correcting the cause of shock and its detrimental effects should be our goal. Treating the patient with the isolated goal of decreasing the lactate levels is not ideal because lactate generation corresponds to a body necessity and response. Therefore, health care providers should treat the disease, not the lactate. Rather than focusing on a laboratory finding, clinicians must consider the whole clinical picture and patient status. Lactate should not be the only data point. Remember, lactate is a marker of stress response, similar to sinus tachycardia.
What to do…
If the serum lactate is elevated and remains that way after your initial management, you need to consider several things. Don’t just flood the patient with more fluid!
1. If you are treating for sepsis, are you sure it’s actually sepsis? What about a mimic of sepsis? => Perform a focused exam and RUSH evaluation.
2. If this is sepsis, do you have source control? Have you provided antibiotics? Are you missing an additional source? => Consider your source and need for further control (ie, surgical)
3. Is there something else causing a high lactate? Do they have bowel ischemia or compartment syndrome? What about DKA or asthma? Are they on pressors? Does the patient have liver disease, preventing clearance? => Reassess the patient, consider their volume, and look for other causes.
Take Home Points
-The exact pathophysiology of an elevated lactate is likely multifactorial, patient-specific, and disease-specific.
-The patient can be extremely sick but not yet in multi-organ failure. Their kidneys and liver can be working to their maximum potential to clear the lactate but this will probably eventually fail. Be ready.
– Clinical judgment is not a number, and sepsis is not equal to elevated lactate. Our goal should be to treat the primary disease instead of a number which is a marker of multiple metabolic reactions, not only oxidative stress secondary to hypoxia.
– Beta blockers can decrease lactate production in septic patients. Beware.
References/Further Reading
- Casserly B, Phillips G, Schorr C, et al. Lactate Measurements in Sepsis-Induced Tissue Hypoperfusion: Results From the Surviving Sepsis Campaign Database. Critical Care Medicine, 2015;43(3).
- Qvisth V. Catecholamine Regulation of Local Lactate Production in Vivo in Skeletal Muscle and Adipose Tissue: Role of β-Adrenoreceptor Subtypes. The Journal of Clinical Endocrinology and Metabolism. 2008;93(1):240-246.
- Farkas J. Understanding lactate in sepsis & Using it to our advantage. PulmCrit (EM Crit). https://emcrit.org/pulmcrit/understanding-lactate-in-sepsis-using-it-to-our-advantage/. Accessed November 14, 2018.
- Suetrong B, Walley keith. Lactic Acidosis in Sepsis: It’s Not All Anaerobic. Contemporary Reviews in Critical Care Medicine. 2016;149(1):252-261.
- Phypers B. Lactate physiology in health and disease. Continuing Education in Anaesthesia Critical Care & Pain. 2006;6(3):128-132.
- Sterling SA, Puskarich MA, Jones AE. The effect of liver disease on lactate normalization in severe sepsis and septic shock: a cohort study. Clin Exp Emerg Med. 2015;2(4):197-202. Published 2015 Dec 28. doi:10.15441/ceem.15.025
- Chathman JC. Lactate – the forgotten fuel! The Journal of physiology. 2002;542.
- Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate levels. Mayo Clin Proc. 2013;88(10):1127-40.
- Vincent J-L, Quintairos e Silva A, Couto L, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. The value of blood lactate kinetics in critically ill patients: a systematic review. 2016;20(257).
- Contenti J, Occelli C, Corraze H, Lemoël F, Levraut J. Long-Term β-Blocker Therapy Decreases Blood Lactate Concentration in Severely Septic Patients. Critical Care Medicine. 2015;43(12).





2 thoughts on “Normal Lactate, but a Sick Patient… Lactate is Not Everything”
Lactate sucks! Recently did emergency laparotomy for infant with normal chemistry and NORMAL lactate. The whole of his intestine from mid duodenum to mid sigmoid was infarcted. And the lactate was normal.
Pingback: February FOAMed - FRCEM Success