
Author: Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) & Justin Bright, MD (@JBright2021)
A 62 year-old male presents by EMS with several episodes of emesis and a fever of 100.5oF. He has been feeling worse over two days and has not been able to eat. He has a past history of COPD, HTN, and DM with several recent hospitalizations for COPD exacerbations. His initial VS reveal tachycardia, fever, and tachypnea. He meets criteria for SIRS. You begin treatment for pneumonia and COPD exacerbation. His wife appears one hour later and mentions that he has been unable to take his oral medications due to his vomiting, one of them being his oral steroid that he has been taking for over one month.
A 38 year-old female presents with dyspnea and low grade temperature of 100.6oF. She is tachypneic and has some slight chest pain worse with deep breaths. She is visiting a friend and traveled by plane. Chest Xray reveals a right side consolidation, and ECG shows sinus tachycardia. You provide 1L of NS and some antibiotics for what you think is pneumonia, and she improves.
Background
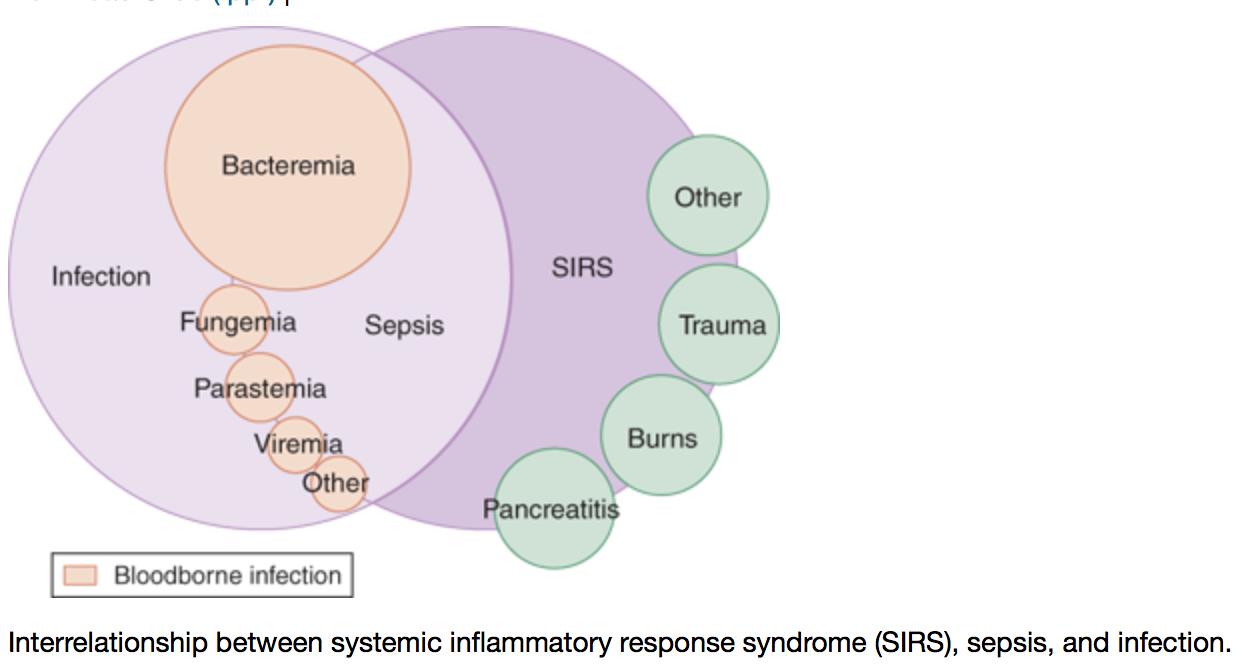
SIRS and sepsis are common clinical entities. A wide range of estimates for prevalence exists, with 300 to 1000 cases per 100,000 persons per year. Once a septic patient is admitted, more than half will require at least step down unit care or greater. Sepsis syndromes consist of a continuum, with varying definitions. The definition of SIRS includes: HR > 90 bpm, RR > 20 or PaCO2 < 32, temperature < 36oC or > 38oC, and a WBC count < 4 x 109 cells/L or > than 12 x 109 cells/L or > 10% bands. Two or more of these equals SIRS, and two or more with a source of infection equals sepsis.1,2 Unfortunately these criteria are non-specific, and the criteria alone do not provide a diagnosis or predict outcome. However, associated organ dysfunction does predict worse outcome.
A great deal of literature exists on sepsis and providing state of the art care in the ED. As EM physicians, we pride ourselves on resuscitating sick patients, and we are well aware that septic patients can rapidly decline clinically. Finding the source and providing appropriate antibiotics, adequate preload with IV fluids, and vasopressors if necessary are key components. The SIRS criteria are our first line of defense in the early identification of sepsis. But, it is important to recognize that just because a patient has multiple SIRS criteria, they may not actually be septic.
Many conditions mimic sepsis by meeting criteria for SIRS. If these conditions are not considered, there is potential for increased mortality and morbidity. These conditions include: pulmonary embolism (PE), adrenal insufficiency, diabetic ketoacidosis (DKA), pancreatitis, anaphylaxis, bowel obstruction, hypovolemia, colitis, vasculitis, toxin ingestion/overdose/withdrawal, and medication effect. These mimics are a common cause of misdiagnosis in the ED. All of these clinical conditions produce symptoms and signs that meet SIRS (fever, elevated WBC, tachypnea, decreased distal perfusion, low urine output, confusion, end-organ malfunction).
Why do these conditions mimic sepsis? It all comes down to the pathophysiology. Sepsis ultimately results from a complex interaction of pro-inflammatory, anti-inflammatory, activated complement system, and coagulation mediators that in association with detector and signaling markers, trigger a host response. Initiators (microbes, trauma, hypoxia, ischemia, toxins) cause local tissue damage, which release local pro- and anti-inflammatory markers. Proinflammatory signalers include TNF, IL-1, and IL-6, while anti-inflammatory markers include IL-4, IL-10, IL-11 and soluble TNF receptors. These are designed to function and contain at a local level. If the initiators overwhelm the local response, the mediators affect multiple systems in the body: dermal, cardiovascular, gastrointestinal, renal, neurologic, hematologic/coagulopathic, pulmonary, and endocrine.3,4 All of these mimics have a similar endgame: triggering a systemic reaction that looks just like sepsis.
This post will take a step-by-step approach on how to avoid misdiagnosis and catch these mimics.
Approach:
Resuscitate first and ask questions later. A patient with a sepsis mimic will look just like a true septic patient with fever, tachycardia, tachypnea, and change in WBC. As such, your initial efforts should focus on resuscitating first. Go through Airway, Breathing, Circulation, Disability/D-stick, Exposure, FAST exam/fetus (if the patient is female, is she pregnant?). Obtain IV access, attach monitors, and be prepared to provide supplemental O2.
Once the primary survey has been completed, then use the history and exam. A careful history and exam from head to toe can allow you to target your resuscitation and management to the clinical condition. Always think sepsis first, especially in the immunocompromised and elderly patient.
The first task is to search for a potential source in the setting of SIRS: The LUCCASSS mnemonic will assist the search for source: lung (pneumonia), urine (cystitis/pyelonephritis), cardiac (endocarditis), CNS (meningitis, encephalitis), abdominal (abscess, cholecystitis), spine (osteomyelitis, abscess), skin (cellulitis, IV line/PICC infection), and septic arthritis. History, physical exam, laboratory data, and imaging can usually pinpoint the source of sepsis. Utilizing chest Xray, urinalysis/urine dipstick, physical exam (HEENT, cardiac, lung, abdomen, GU, and skin), and history will likely provide a diagnosis, but a systematic approach should be followed.2
For a detailed look on sepsis and its sources, see a prior post at:
If no source is found, carefully evaluate the patient again while continuing resuscitation, using history and physical exam to evaluate for the following clinical entities that will meet SIRS criteria.
Signs of Sepsis:
Fever is a cardinal sign of inflammation and infection; however, fever does not equal infection. Cytokines induce a febrile response, mediated by the hypothalamus. Most, but not all, diseases causing true sepsis are associated with temperatures greater than 102oF.5 This is excluding elderly and immunosuppressed patients, where a temperature of 99/100 is often a true fever.6 Per an older review by Cunha, a normal host (i.e. not elderly, uremic, immunosuppressed), with a temperature of less than 102oF or greater than 106oF is usually noninfectious. On the other hand, hypothermia is a clue to bacteremia and true sepsis.5
Hemodynamic effects of septic shock include decreased peripheral resistance with increased cardiac output and tachycardia in the early stages, or distributive shock (also with anaphylaxis, pancreatitis, etc.). Later stages demonstrate findings of hypovolemic shock with increased resistance, lower cardiac output, and cooler peripheral extremities with poor capillary refill. These findings are not specific for sepsis unfortunately.3-5
Laboratory data are also not specific for sepsis, just like the hemodynamic effects. Stress causes an increased WBC count with left shift. Even coagulopathic derangements occur in this systemic inflammatory state that is not sepsis. Fibrin split products, fibrinogen, coagulation panel will not help in differentiating mimics from true sepsis. Leukopenia and thrombocytopenia are more suggestive of sepsis, but they are not definitive. C-reactive protein (CRP) and procalcitonin (PCT) have been studied for use in sepsis, but again, they are not specific for sepsis. Lactic acid elevation and base excess/deficit are commonly used for resuscitation, but they will not pinpoint the cause of shock.4,5
In summary, relying on SIRS, hemodynamic effects, and laboratory data will not definitely diagnose sepsis unless a source is found. What mimics should you evaluate for, and what history and physical exam findings can assist you differentiating these conditions from sepsis?
Anaphylaxis: This deadly condition must be diagnosed quickly for adequate treatment. A simplified way to diagnose is with acute onset of illness and involvement of two organ systems (skin, mucosa, respiratory, hemodynamic, GI symptoms). A known exposure with hypotension also meets criteria. Full criteria are:

Diagnosis is easy when a patient presents with a known allergy and classic symptoms. However, they may present in distributive shock with no history. The numerous mediators released due to the allergen will cause a SIRS response that appears like sepsis, but fever should not be present. Examine for lingual/laryngeal edema, urticaria, and wheezing. Ask about allergic exposures. If present, provide IM epinephrine 1:1000 0.3ml in the lateral thigh. Epinephrine is the most important treatment.7,8
Aspiration: Aspiration pneumonitis is an inflammatory chemical injury of the tracheobronchial and lung parenchymal systems causing dyspnea, cough, and tachypnea. This is due to inhalation of gastric contents. Classically, aspiration injury/pneumonitis requires at least 20ml of contents with a pH < 2.5. These patients will present a systemic response to the respiratory inflammation due to the pneumonitis. Patients from a nursing facility, history of stroke, periodontal disease, elderly, and on chronic proton pump inhibitor therapy are predisposed to developing pneumonia. Check a chest Xray and look for these risk factors. If risk factors are present with fever and an infiltrate on chest Xray is present, strongly consider admission and antibiotics. However, if the patient has no fever in the setting of aspiration, hold on antibiotics.9,10
Adrenal insufficiency: These patients will present with abdominal pain, nausea/vomiting, diarrhea, weakness, fatigue, salt craving, and often hypotension. Blood pressure may be resistant to vasopressors. Ask the patient about prior steroid courses and known adrenal insufficiency. Evaluate for risk factors such as tuberculosis, chronic steroid use, and metastatic cancer. Risk factors from the history and laboratory findings such as hyponatremia, hyperkalemia, hypoglycemia, and hypercalcemia can assist in the diagnosis (primarily in primary insufficiency). Hydrocortisone in stress doses (100mgIV X1) is required if this is diagnosed.11
Please see a prior emDocs.net post on adrenal insufficiency and crisis: http://www.emdocs.net/adrenal-crisis-in-the-ed/
Bowel obstruction: These patients will often present with significant abdominal pain (which may be episodic), nausea, and vomiting. They may have experienced diarrhea due to emptying of stool distal to the point of obstruction. The large and small bowel can be obstructed by multiple processes. Evaluate the patient for prior abdominal/pelvic surgery, hernia, and prior obstructions. Complete a careful abdominal exam looking for hernia, peritoneal findings, abdominal distension (one of the most sensitive and specific physical exam findings), and masses. Obstruction can also contribute to dehydration.12 WBC count may be elevated, but elevations >20,000/mm3 with left shift is suspicious for infarction or peritonitis. Extreme leukocytosis >40,000/mm3 suggests mesenteric vascular occlusion.13 CT of the abdomen and pelvis is the best test for diagnosis, as plain Xrays have sensitivities in the range of 60%. US has recently demonstrated utility for diagnosis of bowel obstruction.14 Surgical consultation is required for true mechanical obstruction.
Diabetic Ketoacidosis (DKA): Patients with DKA present with symptoms and signs similar to sepsis. They are often hypovolemic due to the osmotic diuresis from hyperglycemia. They will be acidotic from elevated ketones and lactate. Tachypnea and hyperpnea will be present in significant metabolic acidosis (respiratory compensation). Altered mental status, confusion, tachycardia are also often present. The major aspect of DKA is discovering what caused the patient to go into DKA. Infection, ischemia, noncompliance, drug abuse, PE, pancreatitis, bleeding, trauma, and many other causes can tip the patient into DKA. Infection is a common cause, including pneumonia and urinary tract infection. Take a complete history for infectious symptoms and for the exam, look at HEENT, lungs, abdomen, and skin. Obtain a urinalysis and chest Xray. Infection can be subtle in these patients. In the setting of DKA, it is likely better to provide empiric antibiotics for assumed infection. Ensure you resuscitate with IV fluids first, and insulin second.15,16
Please see two prior emDocs posts on DKA: 1) http://www.emdocs.net/myths-dka-management/ 2) http://www.emdocs.net/lyceum-bullets/
Heat Emergencies: These present as a continuum of disorders ranging from heat cramps and edema to heat stroke, which presents with altered mental status and temperatures often greater than 40oC (104oF). This deadly disease may present in two forms: nonexertional and exertional. The absence of sweat is not part of any diagnostic criteria. Ask the EMS providers, patient, and care providers about the scene, environment, patient activity, and medications (which can affect heat dissipation such as beta blockers, anticholinergics, antiparkinsonian agents, and sleep aids). Evaluate the patient for diaphoresis, and most importantly, obtain a core temperature. Rapidly cooling these patients to 39oC is essential in treatment. Removing the patient from the environment, cooled IV fluids, and either immersion cooling or evaporative cooling will decrease morbidity and mortality.17,18
Hypovolemia: Any form of fluid depletion can cause tachycardia and tachypnea, meeting SIRS criteria. Hypovolemia itself can also cause systemic inflammation, increasing WBC and causing temperature elevation. Look for signs of external fluid loss such as hemorrhage and trauma, diarrhea, GI bleeding, vomiting, and insensible losses (tachypnea and hyperpnea). The elderly patient with a medication change, especially diuretics, can drastically affect fluid balance and lead to dehydration. Examine the mucous membranes, turgor, capillary refill, distal peripheral pulses, and vital signs (tachypnea and tachycardia are great markers for hypovolemia and dehydration). If tolerant of oral intake, begin PO fluids. IV fluids can be beneficial to replace fluid quickly.19,20
Pulmonary Embolism (PE): The majority of these patients will fail PERC for PE, as many will present with tachycardia. However, using Wells/Geneva/clinical gestalt can assist you. Evaluate the patient for signs/symptoms concerning for PE/DVT, recent travel history, prior history of thrombosis, family history of thrombosis, history of cancer, shortness of breath with pleuritic chest pain, tachypnea, and leg swelling. These patients may have fever, often low grade. Evaluate the chest Xray for signs of PE such as Westermark sign, Hampton’s hump, and atelectasis, even though these findings are insensitive.21,22 If the patient is moderate to high risk, strongly consider ordering the CT.
Pancreatitis: Patients with pancreatitis will likely present with abdominal pain and nausea/vomiting. Pancreatic breakdown due to enzyme release will release numerous systemic inflammatory mediators, triggering SIRS. Patients may be fluid depleted due to third spacing of fluids and GI fluid loss. Pain and dehydration can cause low blood pressure, tachycardia, and tachypnea. A low-grade elevation in temperature may be present. Acute respiratory distress syndrome and pancreatic necrosis with infection are complications of pancreatitis. A history of pain in the epigastrium with vomiting, tenderness in the epigastrium, alcohol use/gallstone presence can all assist in the diagnosis. Diagnosis requires two of the following: characteristic abdominal pain, lipase level three times normal, and US or abdominal CT findings consistent with pancreatitis. Obtain a RUQ US to look for gallstones, obtain liver function tests, and ask carefully about alcohol (the two most common causes of pancreatitis in the U.S.). Fluid resuscitation is important for these patients, as is control of their pain and emesis.24,25
Intestinal ischemia: A reduction in intestinal blood flow causes ischemia, which releases the inflammatory mediators triggering SIRS. Colonic (large bowel) ischemia often affects the elderly. Close to 15% will develop gangrene of the colon, which is life threatening. This is most commonly due to non-occlusive disease (95% of cases), affecting the “watershed” areas of the colon (splenic flexure and rectosigmoid junction). Unfortunately these patients often have multiple comorbidities, which often clouds the clinical picture. These patients will present with rapid onset of cramping abdominal pain, usually with the urge to defecate. Bloody stools and/or diarrhea occur in 80%. Risk factors include aortoiliac surgery, prior coronary bypass, history of CAD/myocardial infarction, and dialysis. Three phases have been described: Hyperactive, Paralytic, and Shock (which may not occur). WBC count is often elevated, and diagnosis includes abdominal/pelvic CT. Treatment is supportive with IV fluids and bowel rest.25 Mesenteric (small bowel) ischemia can present with elevated lactate and WBC count. Tachycardia and tachypnea may also be present. The four types include arterial embolism, arterial thrombosis, venous thrombosis, and non-occlusive. This disease requires surgical consultation and anticoagulation.26
Thyroid disease: Thyrotoxicosis and thyroid storm are clinical syndromes with tachycardia, altered mental status, tremors, fever, GI symptoms, and often elevated WBC counts. These patients are often hemodynamically unstable. The Burch & Wartofsky Diagnostic Criteria can be utilized for diagnosis, with scores > 45 highly suggestive of thyroid storm. Evaluate the patient for prior thyroid disease, tremor, goiter, and lid lag. Vital signs will reveal warm peripheral extremities, wide pulse pressure, tachycardia, and elevated temperature. Mortality rates can reach 100% if left untreated, thus diagnosis is vital. Obtain labs for FT4 and TSH and begin treatment with cooling, beta blockade, inhibiting thyroid hormone release and synthesis, and peripheral conversion of thyroxine to triiodothyronine.27,28
Toxic ingestion/overdose: Many patients with ingestions/overdoses will present with SIRS criteria. The sympathomimetic toxidrome with tachycardia, hypertension, fever, diaphoresis, pupil dilation, and altered mental status can present just like meningitis and sepsis. Other toxins like salicylates (tachypnea, respiratory alkalosis but metabolic acidosis, altered mental status, tachycardia from dehydration), MDMA/Bath salts/Synthetic cannabinoids (sympathomimetic toxidrome), anticholinergics (febrile, tachycardia, dilated and nonreactive pupils, “pleasantly” altered mental status, with no diaphoresis) can all look like sepsis.29,30 Serotonin syndrome with altered mental status, hyperthermia, tachycardia, myoclonus (lower extremities more than upper extremities) is a clinical diagnosis, and the Hunter Toxicity Criteria Decision Rule can assist: Serotonergic agent plus spontaneous clonus, inducible clonus and agitation/diaphoresis, ocular clonus and agitation/diaphoresis, tremor and hyperreflexia, or hypertonia and fever and clonus.31
Malignant hyperthermia and neuroleptic malignant syndrome are other sepsis mimics. The most important aspect of differentiating these conditions is the history and exam. Question the patient about ingestion. Ask the care providers and EMS crew if there was ingestion, medications the patient takes, medications they have access to, what the scene was like, and how the patient was found. Always ask the elderly patient and family/care providers multiple times about medications, as the patient may have different medication lists. The elderly are high-risk patients for adverse medication effects and interactions due to their physiology, multiple medications, and comorbidities. Complete your exam focusing on mental status, pupils, diaphoresis (axillary, upper lip), abdomen, lungs, skin (warm/flushed/diaphoresis), reflexes, and clonus. Benzodiazepines are the treatment of choice for agitation, sympathomimetics, and serotonin syndrome. Providing IV fluids will help these often dehydrated patients. Remember, the elderly tachypneic “septic” patient may in fact be a salicylate overdose patient who requires bicarbonate infusion and urinary alkalinization. Be wary of intubating these patients, as any decrease in serum pH will increase salicylate concentration in the central nervous system. 32
Withdrawal: Patients in withdrawal states, particularly from alcohol or benzodiazepines, can meet SIRS. These states can be deadly, but utilizing history and exam can diagnose withdrawal states. These patients may present with hypertension, tachycardia, tremor, GI symptoms, altered mental status, visual disturbances, and diaphoresis. Use a clinical scale to treat by symptoms (CIWA), and begin treatment with benzodiazepines.33
Vasculitis: These clinical entities are due to chronic, inflammatory, autoimmune disorders. Adverse drug/medication reaction, worsening of chronic illness, acute complication, and acute exacerbation will often meet criteria for SIRS through systemic inflammation. Many of the extra-articular and dermatologic conditions will result in major morbidity and mortality if not promptly diagnosed and managed. The vast majority of patients will have vague complaints such as fatigue, elevated temperature, diffuse pain, and weight loss. Vessel wall damage due to activation of the immune and complement systems are the predominant cause of morbidity and mortality. Your history will provide the keys to diagnose. Evaluate the patient for prior history, immunosuppressive medications, skin changes, and end organ damage. These patients are often on steroids or other immunosuppressive agents, so always consider infection. Also recognize that chronic steroid therapy can cause a baseline leukocytosis. If they have known disease, speak with their primary physician and rheumatologist.34-36
Please see prior a emDocs post of management of the patient with vasculitis: http://www.emdocs.net/the-emergency-medicine-approach-to-vasculitides/
There are many other conditions that can mimic sepsis such as anemia, myocardial ischemia, GI bleeding, spinal cord injury, and heart failure, so make sure to keep these in mind as well.5
Summary/Key Points:
The most important aspect of managing these patients is resuscitation first. Evaluate the ABCDEs. The history and exam are keys to finding the culprit, but always consider infection first. However, sepsis requires a source of infection. Don’t anchor on sepsis if no source is found. Reassess your differential and consider anaphylaxis, aspiration, bowel obstruction, colitis, hypovolemia, pancreatitis, PE, GI bleeding, heart failure, ACS, spinal cord injury, toxic overdose, medication effect, and vasculitis.
References/Further Reading:
- Elixhauser A, Friedman B, Stranges E. Septicemia in U.S. Hospitals, 2009. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb122.pdf.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 2013;41:580–637.
- Remick DG. Pathophysiology of Sepsis. Am J Pathol. 2007 May;170(5): 1435-1444.
- Canetnacci MH, King K. Severe Sepsis and Septic Shock: Improving Outcome in the Emergency Department. Emerg Med Clin N Am 2008;26:603–623.
- Cunha BA. Sepsis and its mimics. Intern Med 1992. 13:48-55.
- Samaras, N, Chevalley, T, et al. Older patients in the emergency department: a review. Ann Emerg Med 2010;56:261-269.
- Zilberstein J, McCurdy MT, Winters ME. Anaphylaxis. J Emerg Med 2014 Aug; 47(2):182
- Nowak R, Farrar JR, Brenner BE, et al. Customizing anaphylaxis guidelines for emergency medicine. J Emerg Med 2013 Aug; 45(2): 299-306.
- Marik, PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med 2001; 344:665-671.
- DiBardino DM, Wunderink RG. Aspiration pneumonia: a review of modern trends. J Crit Care. 2015 Feb;30(1):40-8.
- Tucci V, Sokari T. The clinical manifestations, diagnosis, and treatment of adrenal emergencies. Emerg Med Clin North Am. 2014; 32(2): 465-484.
- Jackson PG and Raiji M. Evaluation and management of intestinal obstruction. Am Fam Physician.2011 Jan 15;83(2):159-165.
- Salvator JV and Price TG. Bowel Obstruction and Volvulus. In: Tintinalli’s Emergency Medicine. 8th ed. New York: McGraw-Hill; 2015; (cited 2015).
- Hefny AF, Corr P, Abu-zidan FM. The role of ultrasound in the management of intestinal obstruction. J Emerg Trauma Shock. 2012;5(1):84-6.
- Perilli G, Saraceni C, et al. Diabetic ketoacidosis: a review and update. Curr Emerg Hosp Med Rep 2013;1:10-17.
- Savage MW, Datary KK, et al. Joint British Diabetes Societies guideline for the management of diabetic ketoacidosis. Diabet Med 2011 May;28(5):508-15.
- Yeo TP. Heat stroke: a comprehensive review. AACN 2014;15(2):280-93.
- Bross MH, Nash BT Jr, Carlton FB Jr. Heat emergencies. Am Fam Phys 1994;50(2):389-96,398.
- Kolecki P. Hypovolemic shock. Emedicine: Medscape. http://emedicine.medscape.com/article/760145-overview. Accessed 14 September 2015.
- Sonnenblick M, et al. Diuretic-induced severe hyponatremia. Review and analysis of 129 reported patients Chest. 1993;103(2):601-606.
- Lapner ST. Clinical review: diagnosis and management of pulmonary embolism. BMJ 2013;346:f757.
- Tapson VF. Acute pulmonary embolism. N Engl J Med 2008; 358:1037-1052.
- Johnson CD. Clinical review: acute pancreatitis. BMJ 2014;349:g4859.
- Whitcomb DC. Acute pancreatitis. N Engl J Med 2006; 354:2142-2150.
- Theodoropoulou A and Koutroubakis IE. Ischemic colitis: clinical practice in diagnosis and treatment. World J Gastroenterol. 2008 Dec 28; 14(48): 7302–7308.
- Oldenburg WA. Acute mesenteric ischemia: a clinical review. Arch Intern Med. 2004;164(10):1054-1062.
- Vaidya B. Clinical review: diagnosis and management of thyrotoxicosis. BMJ 2014;349:g5128.
- Chiha M, Samarasinghe S, Kabaker AS. Thyroid storm: an updated review. J Intensive Care Med. 2015 Mar;30(3):131-40.
- Kolecki P. Sympathomimetic toxicity. Emedicine: Medscape. http://emedicine.medscape.com/article/818583-treatment. Accessed 14 September 2015.
- Ramnarine M. Anticholinergic toxicity. Emedicine: Medscape. http://emedicine.medscape.com/article/812644-overview. Accessed 14 September 2015.
- Buckley NA, Dawson AH, Isbister GK. Practice pointer: serotonin syndrome. BMJ 2014;348:g1626
- Pearlman BL, Gambhir R. Salicylate intoxication: a clinical review. Postgrad Med. 2009 Jul;121(4):162-8.
- Schuckit MA. Recognition and Management of Withdrawal Delirium (Delirium Tremens). N Engl J Med 2014; 371:2109-2113.
- Miller A, et al. An approach to the diagnosis and management of systemic vasculitis revised version with tracked changes removed. Clin Exp Immunol 2010 May;160(2):143–160.
- Suresh E. Diagnostic approach to patients with suspected vasculitis. Postgrad Med J 2006 Aug;82(970):483–488.
- Tsokos GC. Systemic Lupus Erythematosus. N Engl J Med 2011; 365:2110-2121.





5 thoughts on “Mimics of Sepsis: What do ED Physicians Need to Know?”
We must remember that we need only have a suspected source in order to start treating our septic patient. Far to often I see residents holding off on antibiotics because “we don’t have a source” yet the patient is an oncology patient, receiving chemotherapy and had abdominal surgery 1 month prior to their presentation to the ED, with a normal WBC count, clean urine and negative chest x-ray. (This is a recent example from my own department). With CMS making bundle compliance a must we should be following the recommendations as set out in order to care for our patients in the best way possible.
Not every patient with SIRS is septic but let us not miss any who are and keep the mortality rate low.
We must remember that we need only have a suspected source in order to start treating our septic patient. Far to often I see residents holding off on antibiotics because “we don’t have a source” yet the patient is an oncology patient, receiving chemotherapy and had abdominal surgery 1 month prior to their presentation to the ED, with a normal WBC count, clean urine and negative chest x-ray. (This is a recent example from my own department). With CMS making bundle compliance a must we should be following the recommendations as set out in order to care for our patients in the best way possible.
Not every patient with SIRS is septic but let us not miss any who are and keep the mortality rate low.
Thank you for the comment, and I completely agree. The whole clinical picture should be taken into account, especially with the patient with SIRS criteria. The vast majority of patients require antibiotics, as treatment can always be withdrawn. A high risk patient, such as the one you speak of, definitely requires broad-spectrum antibiotics. The sick, hemodynamically unstable patient with a great story for DKA or heat stroke should also receive empiric coverage.
Pingback: Laktat – Översikt – Mind palace of an ER doc
Pingback: Oncology Patient in Resus | Resuscitology.com