
Author: David Cisewski, MD (@dhcisewski, EM Resident Physician, Icahn School of Medicine at Mount Sinai) and Lillian Wong, MD (Elmhurst Hospital Center, Department of Emergency Medicine, Elmhurst, NY) // Edited by: Jamie Santistevan, MD (@jamie_rae_EMdoc – EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD (@MPrizzleER – Assistant Professor of Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center); and Brit Long, MD (@long_brit – EM Attending Physician, San Antonio, TX)
Welcome to this edition of ECG Pointers, an emDOCs series designed to give you high yield tips about ECGs to keep your interpretation skills sharp. For a deeper dive on ECGs, we will include links to other great ECG FOAMed!

(Image courtesy of wikicommons)
The Case:
A 59-year-old male with a past medical history of hypertension, diabetes, coronary artery disease (previous LAD stent placement), hepatocellular carcinoma and cholecystectomy presents to the ED with shortness of breath and diffuse abdominal pain. The patient denies chest pain but has noted difficulty taking deep breaths due to the abdominal discomfort. Additionally, the patient notes 2 episodes of non-bloody, non-bilious vomiting over the previous 24 hours. The patient’s last bowel movement was 12 hours prior to arrival, and he is not passing gas.
The patient’s initial vital signs on arrival include a blood pressure of 104/81 mmHg, heart rate 111 beats per minute, temperature of 37.9 °C, and a respiratory rate of 14 breaths per minute (oxygen saturation 96% on 100% FiO2).
On physical examination the patient appears distressed and slightly diaphoretic. The lungs are clear to auscultation bilaterally. Heart sounds reveal a normal S1/S2. The abdomen is moderately distended, diffusely tender to palpation, and tympanic with decreased bowel sounds. Initial ultrasonographic assessment shows no evidence of free fluid in the abdomen. Bedside transthoracic echocardiogram (TTE) demonstrates no pericardial effusion, an estimated left ventricular ejection fraction (LVEF) of 55%, and no regional wall motion abnormalities (RWMA).
An initial ECG is performed which shows ST-segment elevations with an upward shift preceding the QRS complexes in the inferior leads II and aVF (Fig. 1).

Figure 1. There are ST-segment elevations with an upward shift preceding the QRS complexes in the inferior leads II and aVF
The beside telemetry monitor displays a rhythm consisting of a continuous ST-segment elevation pattern associated with an upsloping preceding the QRS complex (Fig. 2).

Figure 2. Bedside telemetry monitor displaying persistent ST-segment elevations with an upsloping preceding the QRS complex.
As the resident evaluating the patient you say to yourself, “these are ST-segment elevations….. should I activate the cath lab?”
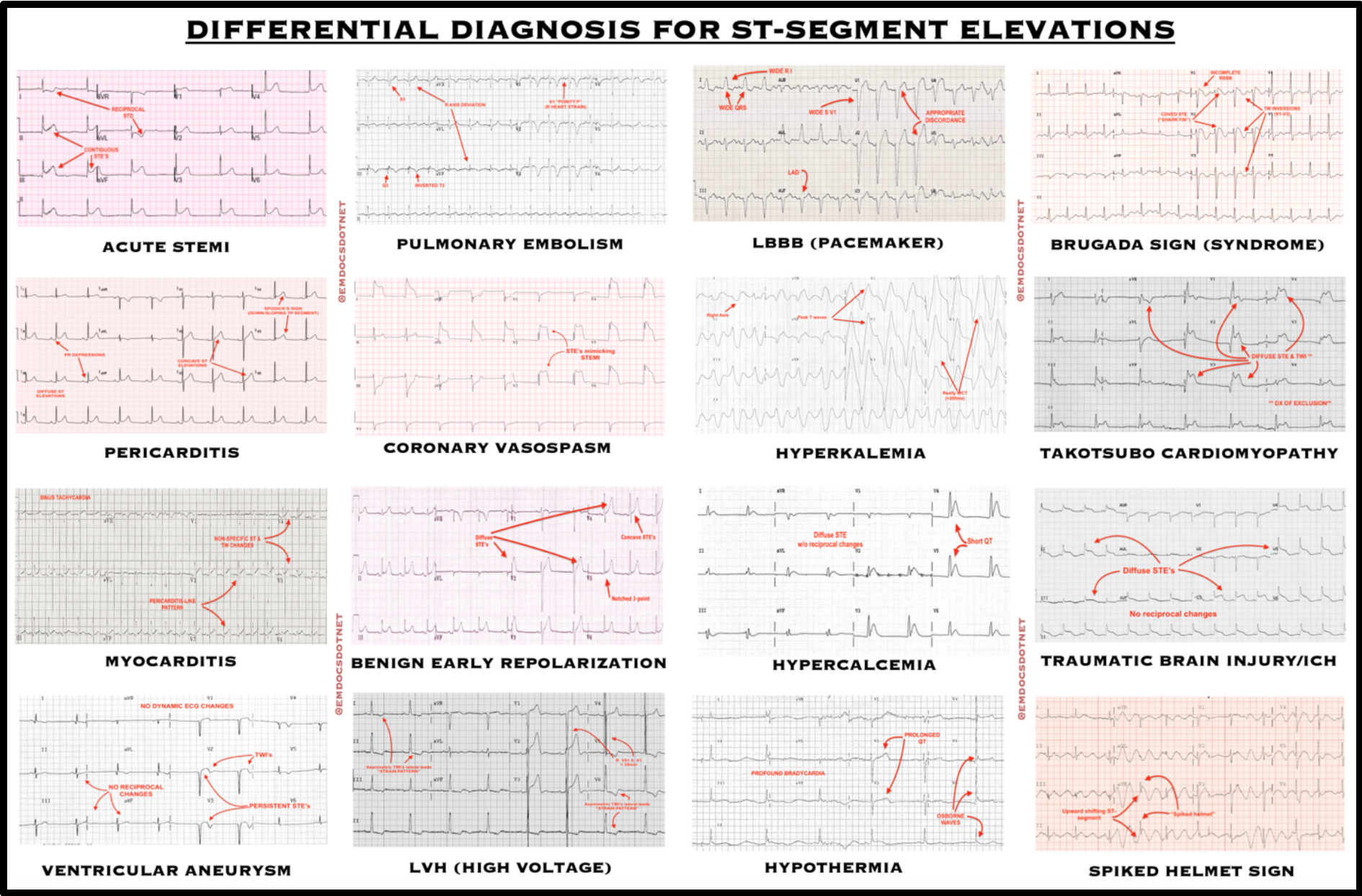
Not necessarily. Although STEMI should always be at the forefront of every differential, ‘not all the ST elevates is an MI’. Of note, there are over a dozen items that should be included in the differential when considering the differential diagnosis for ST-segment elevations. Along with acute STEMI, these include pericarditis/myocarditis, ventricular aneurysm, pulmonary embolism, coronary artery vasospasm, benign early repolarization (BER), left ventricular hypertrophy (LVH/high voltage), left bundle branch block (LBBB)/pacemakers, hyperkalemia, hypercalcemia, hypothermia, Brugada syndrome, Takotsubo cardiomyopathy, traumatic brain injury, and the “spiked helmet” sign (Fig. 3).
Differential Diagnosis for ST-Segment Elevations: ECG findings corresponding to the various underlying pathologies associated with an ST-segment elevation differential diagnosis.
Are there clinical clues I should be considering when assessing a patient with ST-segment elevations?
It is important to note that an ECG is most useful when considering the complete clinical picture. Understanding the patient’s history, symptoms, and presentation can assist in identifying the underlying pathology. See Table 1 for a listing of the classic presentations, key ECG characteristics, and expected workup corresponding to the various underlying pathologies associated with an ST-segment elevation differential diagnosis.
Table 1. Differential Diagnosis ST-Segment Elevations: Classic presentation, key ECG characteristics, and expected workup corresponding to the various underlying pathologies associated with an ST-segment elevation differential diagnosis.

Spiked helmet sign? That sounds a lot like our patient.
As described above, the “spiked helmet sign” is classically seen as an upward shifting ST-segment preceding the start of a QRS complex, predominantly in the inferior leads (II, III, and aVF) [1, 6, 11]. The name is derived from its resemblance to the pickelhaube (“pickaxe bonnet”), a military helmet popularized by King Frederick William IV of Prussia and later adopted by the German and Bavarian armies (Fig. 4) [6]. This ECG manifestation has been noted among critically ill patients in the intensive care setting with retrospective correlation to intraabdominal pathology [1,6]. Continuous “spiked helmet” electric complexes may also be noted on telemetry monitor (Fig. 4).

Figure 3. Spike Helmets: Kaiser Wilhelm II and troops (1915) wearing the pickelhaube (“pickaxe bonnet”). (Image source: WikiCommons)
Under what clinical context should I suspect the “spiked helmet” sign?
The “spiked helmet” sign has been associated with gastric dilatation [3], intestinal obstruction [2, 8], hepatobiliary inflammation (cholecystitis, hepatitis) [4,10], and pancreatitis [7]. Changes in heart position during gastric distention and an irritative effect on the heart by diaphragmatic elevation have all been suggested as underlying causes of the ST-elevations [5]. A pulsatile epidermal stretch resulting from increased intraabdominal pressure has also been a leading hypothesis [6,12]. Although these changes are seen predominantly seen among the inferior ECG leads (II, III, and aVF), presumably due to their proximity to the diaphragm which separates the heart from the intrabdominal pathology [6], similar ECG findings localized to the precordial leads (V1-V6) has been associated with intrathoracic pathology [12].

Figure 4. Spiked Helmet Sign. Upward sloping ST-segment preceding the start of the QRS complex; resembling the pickelhaube (military helmet).
What do I do when I see this “spiked helmet” sign?
To treat the spiked helmet is to treat the underlying cause. Gastric decompression with nasogastric tube placement has been repeatedly shown to resolve the ECG changes [5, 8, 9, 12].
Additionally, an urgent CT scan should be used to identify the underlying intraabdominal pathology. General surgery or the ICU is the typical endpoint for these critically ill patients.
Case conclusion
The astute ED provider recognized these inferior leads with an upward shifting ST-segment preceding the start of a QRS in the clinical setting of abdominal distention as the “spiked helmet” sign. Following analgesic administration, a nasogastric tube was placed and 650 cc of bilious gastric content was suctioned from the stomach, relieving the distention. Repeat ECG following gastric decompression demonstrated complete resolution of the ST-segment elevations in the inferior leads. A computer tomography (CT) of the abdomen and pelvis was performed, demonstrating dilated loops of small bowel >4.0 cm proximal to an intestinal obstruction with thickening of the small bowel. The patient underwent urgent laparotomy for severe small bowel obstruction secondary to prior surgical adhesions.
Main ECG Pointers:
- The differential diagnosis for ST-segment elevation is broad, including both intrathoracic and extrathoracic pathology
- Take into consideration the full history, physical exam, and clinical picture when assessing a patient with ST-segment elevations
- The “spiked helmet” sign – ST-segment elevations preceding the onset of the QRS complexes in the inferior leads – can be a key diagnostic clue to underlying intraabdominal pathology.
For more killer ECG FOAMed check out these posts:
- Littman, 2011 – The “Spiked Helmet” Sign: A New Electrocardiographic Marker of Critical Illness and High Risk of Death
- LITFL – Killer ECG Patterns
- ALiEM – Can’t Miss ECG Findings for the Emergency Medicine Provider
References:
- Agarwal, A., T. G. Janz and N. V. Garikipati (2014). “Spiked helmet sign: An under-recognized electrocardiogram finding in critically ill patients.” Indian J Crit Care Med 18(4): 238-240.
- Asada, S., T. Kawasaki, T. Taniguchi, T. Kamitani, S. Kawasaki and H. Sugihara (2006). “A case of ST-segment elevation provoked by distended stomach conduit.” Int J Cardiol 109(3): 411-413.
- Frais, M. A. and K. Rodgers (1990). “Dramatic electrocardiographic T-wave changes associated with gastric dilatation.” Chest 98(2): 489-490.
- Furuhashi, M., K. Uno, S. Satoh, K. Hoshikawa, E. Sakai, K. Tsuchihashi and K. Shimamoto (2003). “Right bundle branch block and coved-type ST-segment elevation mimicked by acute cholecystitis.” Circ J 67(9): 802-804.
- Herath, H. M., A. Thushara Matthias, B. S. Keragala, W. A. Udeshika and A. Kulatunga (2016). “Gastric dilatation and intestinal obstruction mimicking acute coronary syndrome with dynamic electrocardiographic changes.” BMC Cardiovasc Disord 16(1): 245.
- Littmann, L. and M. H. Monroe (2011). “The “spiked helmet” sign: a new electrocardiographic marker of critical illness and high risk of death.” Mayo Clin Proc 86(12): 1245-1246.
- Makaryus, A. N., O. Adedeji and S. K. Ali (2008). “Acute pancreatitis presenting as acute inferior wall ST-segment elevations on electrocardiography.” Am J Emerg Med 26(6): 734 e731-734.
- Mixon, T. A. and P. D. Houck (2003). “Intestinal obstruction mimicking acute myocardial infarction.” Tex Heart Inst J 30(2): 155-157.
- Patel, K., N. L. Chang, O. Shulik, J. DePasquale and F. Shamoon (2015). “Small Bowel Obstruction Mimicking Acute ST-Elevation Myocardial Infarction.” Case Rep Surg 2015: 739147.
- Ryan, E. T., P. H. Pak and R. W. DeSanctis (1992). “Myocardial infarction mimicked by acute cholecystitis.” Ann Intern Med 116(3): 218-220.
- Tomcsanyi, J., T. Fresz and B. Bozsik (2012). “ST elevation anterior “spiked helmet” sign.” Mayo Clin Proc 87(3): 309; author reply 309.
- Tomcsanyi, J., T. Fresz, P. Proctor and L. Littmann (2015). “Emergence and resolution of the electrocardiographic spiked helmet sign in acute noncardiac conditions.” Am J Emerg Med 33(1): 127 e125-127.





2 thoughts on “Spiked Helmet Sign: An Electrocardiographic Indication of Impending Doom”
Pingback: Nursing FOAMed Review #10 (March 25th - May2nd) - Code Blue LLC
Excellent review