
Author: Filipp Chesnokov, MD (EM Resident Physician, UTSW EM Residency) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 74-year-old male with past medical history of hypertension, hypercholesterolemia, chronic obstructive pulmonary disease, and 60 pack-year smoking history presents to the emergency department with a month of intermittent back pain localized between the scapulae. Review of systems is notable for hoarseness of voice and dysphagia of approximately same duration. Physical exam is remarkable for hypertension and decreased breath sounds throughout all lung fields.
What is your differential diagnosis for this patient? What tests would you order?
Background
A thoracic aortic aneurysm (TAA) is a pathologic dilation of a segment of the thoracic aorta by at least 50% when compared to normal expected diameter. This dilation involves all three layers of the vessel wall, consisting of intima, media, and adventitia.1 The normal aortic diameter varies with location, age, gender, and body habitus of patient.
Aneurysms can be classified by location within the aorta and morphology. Fusiform aneurysms involve the entire circumference of the aorta and are spindle shaped. Saccular aneurysms form an outpouching involving only a portion of the circumference.2 TAAs represent approximately 10% of all aortic aneurysms with estimated annual incidence rate of 5.9 per 100,000 persons.2,3

Etiology
Aneurysms of ascending aorta often result from the fragmentation of elastic fibers and loss of smooth muscle cells, a process known as medial degeneration.2 The underlying cause of medial degeneration is unknown but may be related to aging and chronic hypertension.4 Aneurysms of the aortic arch and descending aorta are most often associated with atherosclerosis.5 Although once the most common cause of ascending aneurysm, syphilis is now uncommon in developed countries. Syphilitic aneurysms can affect any part of the aorta but are most common in the ascending aorta and aortic arch.4 Traumatic aneurysms occur just distal to the origin of the left subclavian artery at the site of the ligamentum arteriosum, which acts as an anchor during sudden deceleration.
Despite the correlation between certain types of aneurysms and their anatomic location, the etiology of non-genetically mediated aneurysms is likely multifactorial. Risk factors for developing TAA include hypertension, atherosclerosis, smoking, chronic obstructive pulmonary disease, increased body mass index, male gender, older age, bicuspid or unicuspid aortic valves, and family history.6
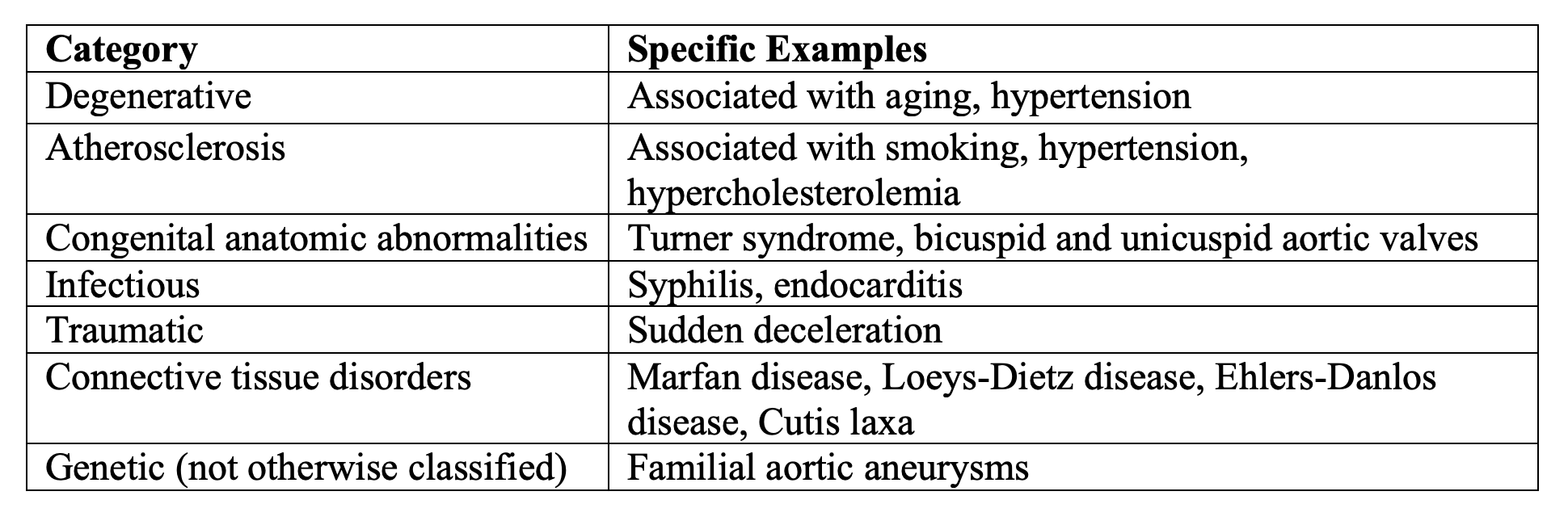
Genetic conditions associated with TAAs can be categorized as syndromic vs. non-syndromic conditions. The former includes conditions such as Marfan syndrome, Loeys-Dietz syndrome, Ehlers-Danlos syndrome, aneurysm-osteoarthritis syndrome,Turner syndrome, and cutis laxa with aneurysm. The latter includes bicuspid aortic valve with aneurysm and familial aortic aneurysm.7 Another method of categorizing genetic and non-genetic conditions associated with TAAs is provided in the following table:
Presentation
Most TAAs are asymptomatic at time of discovery; however, an enlarging TAA can compress adjacent tissues and structures leading to symptoms such as cough, shortness of breath, chest pain, dysphagia, and hoarseness.2 Involvement of the ascending aorta may present as congestive heart failure due to development of aortic regurgitation. Compression of the vena cava may lead to superior vena cava syndrome (edema of upper extremities, neck, and face).2 Complications of TAA include aortic dissection and rupture, which can present with sudden onset chest pain, hypotension, and shock.11
Diagnosis
Often, TAAs are diagnosed incidentally on chest radiographs with findings such as widened mediastinal silhouette, calcified outline of dilated aorta, enlarged aortic knob, or tracheal displacement.

Incidental findings of TAAs on chest radiograph or echocardiographs should prompt further evaluation with computed tomographic angiography (CTA) with contrast or magnetic resonance angiography (MRA) with contrast.8 Invasive aortography was once the golden standard for evaluation of aortic pathology but is now limited to patients undergoing endovascular therapy or when other studies have failed to provide satisfactory results.2 TAAs are often associated with aneurysms in other locations. As many as 23% of patients with TAA will have concurrent abdominal aortic aneurysms. As such, the diagnosis of TAA warrants screening for additional aneurysms.9
Treatment
Treatment of small, asymptomatic TAAs focuses on blood pressure and heart rate control with beta blockers (BBs) such as propranolol, which help minimize the impact force of ejected blood against the aorta as well as shear stress. Evidence for the use of BBs is largely derived from studies of Marfan patients.10,11 Additional agents such as angiotensin-converting-enzyme inhibitors (ACEi) may be required to control blood pressure. The latest consensus guidelines on thoracic aortic disease provide a class I recommendation for administering antihypertensive therapy to all hypertensive patients with thoracic aortic disease and a class IIa recommendation for reducing blood pressure in patients with TAAs using BBs and ACEi to the lowest point that is tolerable by patient without adverse effects.1 There are no clear guidelines regarding emergency physician’s role in the initiation of TAA treatment, therefore consultation with cardiology or cardiothoracic surgery prior to initiation of medical treatment is advised.
Although, there is no data to support an optimal surveillance regimen, regular monitoring of aortic diameter with repeat imaging is recommended.1 Frequent surveillance at the time of initial diagnosis helps characterize the rate of aortic expansion. The average aneurysm expands 0.07 cm/year in the ascending aorta and 0.19 cm/year in the descending aorta.2 Accelerated aneurysmal expansion of greater than 0.5 cm/year in the ascending aorta or 1 cm/year in the descending aorta warrants operative repair.4 If the rate of expansion is slow, subsequent scans can be performed every 1-2 years.12
The decision to perform operative repair of TAAs depends on multiple factors including location of aneurysm, associated symptoms, rate of growth, and patient’s overall condition. Due to the significant morbidity and mortality associated with surgical repair of TAAs, surgical intervention is typically deferred until the risk of rupture/dissection begins to outweigh the risks of surgery. Patients who become symptomatic or have aortic root and/or ascending aorta diameter > 5.5 cm (less if patient has collagen disorder) are treated with operative placement of prosthetic graft. TAAs of the descending aorta with a diameter > 6 cm are routinely treated with endovascular grafting.4 It is important to note that symptomatic TAAs warrant repair regardless of their size as they are much higher risk for rupture and dissection.12

Prognosis
The clinical progression of TAA is continued expansion and eventual rupture. Rupture of TAAs is often fatal because the bleeding is rarely contained. TAAs associated with collagen disorders may expand at an accelerated rate. The risk of complication increases with the diameter of the aneurysm. The annual risk of rupture, dissection, and death for TAAs > 6 cm is 3.6%, 3.7%, and 10.8%, respectively.2 Other risk factors for TAA rupture include age (relative risk increased by factor of 2.6/decade), presence of pain, diastolic hypertension, and renal failure.13 Emergency medicine physicians should recognize that aortic disease is a lifelong condition that puts patients at risk of acute aortic syndromes (dissection, rupture, etc.) regardless of whether they are undergoing medical management or have received interventional therapy.1
In general, operative treatment of TAAs carries significant risk of morbidity and mortality including paraplegia, stroke, diffuse neurologic injury, and intellectual impairment. In comparison to abdominal aneurysm repair, morbidity and mortality for TAAs is significantly higher due to factors such as the need for interrupted aortic arch flow (circulatory arrest) and/or disruption of the spinal arterial supply. An exception to the above statement is that the saccular TAAs, which do well with endovascular repair.2
Key Points
- Most often, patients with TAAs are asymptomatic.
- Symptoms of TAA are often non-specific and may include cough, shortness of breath, chest pain, dysphagia, voice changes, congestive heart failure, and superior vena cava syndrome.
- CTA with contrast and MRA with contrast are the imaging modalities of choice for the diagnosis of TAA.
- Diagnosis of TAA warrants screening for other types of aneurysms such as abdominal aortic aneurysm.
- Symptomatic TAAs warrant urgent repair regardless of size.
- Management of asymptomatic aneurysms that do not meet criteria for surgical repair should focus on control of hypertension with beta blockers.
References/Further Reading
- WRITING GROUP MEMBERS, Hiratzka LF, Bakris GL, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121(13). doi:10.1161/CIR.0b013e3181d4739e
- LeMaire SA, Gopaldas RR, Coselli JS. Thoracic Aneurysms and Aortic Dissection. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. eds. Schwartz’s Principles of Surgery, 10e New York, NY: McGraw-Hill; 2015. http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=980§ionid=59610864. Accessed November 04, 2018.
- Gasper WJ, Rapp JH, Johnson MD. Blood Vessel & Lymphatic Disorders. In: Papadakis MA, McPhee SJ, Rabow MW. eds. Current Medical Diagnosis & Treatment 2019 New York, NY: McGraw-Hill; http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=2449§ionid=194437470. Accessed October 24, 2018.
- Gupta N, Matta EJ, Oldham SA. Cardiothoracic Imaging. In: Elsayes KM, Oldham SA. eds. Introduction to Diagnostic Radiology New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=1562§ionid=95876454. Accessed November 04, 2018.
- Creager MA, Loscalzo J. Diseases of the Aorta. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds.Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill. http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=2129§ionid=192030457. Accessed October 24, 2018.
- Castellano JM, Kovacic JC, Sanz J, Fuster V. Are we ignoring the dilated thoracic aorta?: Castellano et al. Annals of the New York Academy of Sciences. 2012;1254(1):164-174. doi:10.1111/j.1749-6632.2012.06493.x
- Regalado ES, Guo D, Milewicz DM. Thoracic Aortic Aneurysms and Acute Aortic Dissections. In: Murray MF, Babyatsky MW, Giovanni MA, Alkuraya FS, Stewart DR. eds. Clinical Genomics: Practical Applications in Adult Patient Care, 1e New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=1094§ionid=61900414. Accessed November 04, 2018.
- acr.org. (2018). American College of Radiology ACR Appropriateness Criteria® Suspected Thoracic Aortic Aneurysm. [online] Available at: https://acsearch.acr.org/docs/3102329/Narrative/ [Accessed 4 Nov. 2018].
- DeFreitas MR, Quint LE, Watcharotone K, et al. Evaluation for abdominal aortic aneurysms is justified in patients with thoracic aortic aneurysms. The International Journal of Cardiovascular Imaging. 2016;32(4):647-653. doi:10.1007/s10554-015-0807-7
- Shores J, Berger KR, Murphy EA, Pyeritz RE. Progression of Aortic Dilatation and the Benefit of Long-Term β-Adrenergic Blockade in Marfan’s Syndrome. http://dx.doi.org/10.1056/NEJM199405123301902. doi:10.1056/NEJM199405123301902
- Ladouceur M, Fermanian C, Lupoglazoff J-M, et al. Effect of Beta-Blockade on Ascending Aortic Dilatation in Children With the Marfan Syndrome. American Journal of Cardiology. 2007;99(3):406-409. doi:10.1016/j.amjcard.2006.08.048
- Elefteriades JA, Olin JW, Halperin JL, Ziganshin BA. Diseases of the Aorta. In: Fuster V, Harrington RA, Narula J, Eapen ZJ. eds. Hurst’s The Heart, 14e New York, NY: McGraw-Hill; http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=2046§ionid=176565488. Accessed November 04, 2018.
- Kleinschmidt D, Plestis K, Housits P. Indications and surgical strategy for thoracic aortic aneurysm repair. Journal of the American Academy of PAs. 2010;23(2):44–49.





1 thought on “Thoracic Aortic Aneurysms: Pearls and Pitfalls”
Pingback: Aortic Emergencies with George Wills at #stemlynsLIVE • St Emlyn's