Authors: Joseph Blackwell, MD (Emergency Medicine Resident, Carolinas Medical Center, Charlotte, NC) and Kathryn T. Kopec DO (Emergency Medicine Attending, Medical Toxicologist, Carolinas Medical Center, Charlotte, NC) // Reviewed by: Cynthia Santos, MD (@Cynthia Santos, MD); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)

Background
Anti-dysrhythmics have classically been an overwhelming topic for medical students and residents, secondary to the quantity and their varying clinical effects. An anti-dysrhythmic agent is used to treat abnormal cardiac rhythms, and the first classification system for these drugs was the Vaughan-Williams classification in 1970 (1). It is important to note that since then there has been an increase in the number of anti-dysrhythmic agents, improved understanding of the mechanism of actions of these agents, recognition that many of these agents cross class lines, and there are other anti-dysrhythmic drugs that are used that do not fall into one of these four classes (2). In order to adequately understand the different classes and mechanism of action of anti-dysrhythmics, one must re-familiarize themselves with the cardiac conduction cycle:
Figure 1: Action Potential of Cardiac Myocyte

There are five phases to the cardiac myocyte conduction cycle 1.
Phase 0: Depolarization – opening of voltage-gated fast Na+ channels leading to influx of Na+.
Phase 1: Overshoot – Na+ channels close and K+ leaves the cell.
Phase 2: Plateau – Ca2+ influx stabilizes the cell against the K+ efflux.
Phase 3: Repolarization – Ca2+ influx stops and K+ efflux increases.
Phase 4: Resting – Active transport of Na+, K+, Ca2+ against electrochemical gradients.
Figure 2: ECG complex
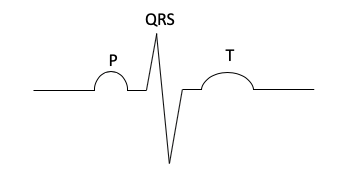
Phase 0 and 1 correlate to the QRS interval seen on the ECG.
Phase 2 and 3 correlates to QTc interval seen on the ECG (3).
With this understanding, we can now attempt to de-mystify the anti-dysrhythmics.
Vaughan- Williams Classification:
Class I – Sodium Channel Blockers
Class IA:
• Examples: Disopyramide, quinidine, procainamide
• Mechanism of Action: Block the fast-acting sodium channels resulting in increased action potential duration and decreased conduction through myocardium.
• Uses: Ventricular tachycardia; recurrent atrial fibrillation and flutter.
• Toxicity: Sinus bradycardia, asystole, PR/QRS/QT prolongation, decreased contractility, and hypotension (4,5). Pulmonary edema can be seen with quinidine overdose secondary to alpha antagonism (5).
• Pearl: When treating ventricular dysrhythmias secondary to class IA anti-dysrhythmics, do not use other IA or IC agents as they may worsen toxicity (4).
Class IB:
• Examples: Lidocaine, tocainide, mexiletine
• Mechanism of Action: Weak sodium channel blockers that result in decreased action potential duration.
• Uses: Monomorphic ventricular tachycardia secondary to toxicologic etiology and post-MI dysrhythmia.
• Toxicity: Bradycardia, hypertension, heart block, nodal and ventricular dysrhythmias, QRS prolongation, and seizures (6).
Class IC:
• Examples: Flecainide, propafenone
• Mechanism of Action: Strong sodium channel blockers that have no effect on action potential duration.
• Uses: Refractory ventricular dysrhythmias and supraventricular tachycardias.
• Toxicity: Seizures, CNS depression, hepatotoxicity, QRS/QT prolongation, pulmonary edema, metabolic acidosis, hypokalemia, hypotension (7).
Class II – Beta-Blockers:
• Examples: Metoprolol, esmolol, atenolol, carvedilol
• Mechanism of Action: Decrease slope of phase 4 depolarization leading to prolonged repolarization at the AV node (8).
• Uses: Atrial fibrillation, atrial flutter, long term maintenance with CHF, routine post-MI drug regiments.
• Toxicity: Intraventricular conduction delay, bradycardia, hypotension, and bronchospasm, especially in patients with asthma or COPD.
• Pearls: Propranolol can cause QRS prolongation secondary to sodium channel blockade and can also cause seizures as it is highly lipid soluble and may cross the blood-brain barrier (9).
Class III – Potassium Channel Blockers
• Examples: Amiodarone, ibutilide, sotalol, dronedarone
• Mechanism of Action: Bind the K+ channels responsible for phase 3 leading to delayed repolarization and resulting in an increased action potential duration and an increased effective refractory period (10).
• Uses: Management of ventricular tachycardia and fibrillation, atrial flutter and fibrillation.
• Toxicity: Bradycardia, heart block, hypotension, QT prolongation
• Pearls: Sotalol also has beta blocking effects (11, 12, 13).
Class IV – Calcium Channel Blockers
• Examples: Verapamil, diltiazem, amlodipine, nifedipine
• Mechanism of Action: Block L-type calcium channels on the vascular smooth muscle, cardiac myocytes, and cardiac nodal tissue leading to prolongation of phase 4 nodal action potential. Resulting in decreased pacemaker activity & increased conduction time and refractory period (14).
• Uses: Atrial fibrillation/flutter with or without RVR as well as AVNRT.
• Toxicity: Bradycardia, hypotension, hyperglycemia, dysrhythmia, cardiogenic shock, seizures.
• Pearls: The degree of hyperglycemia can be used as a marker for severity of ingestion and severe toxicity can be treated with high-dose insulin therapy (15).
Class V – Others
• Other medications such as: digoxin, adenosine, and magnesium can be considered a separate class of anti-dysrhythmics, however, that is a blog post for another day!
Key Take Home Points:
• Class I: Sodium channel blocking agents – monitor for prolonged QRS
• Class II: Beta-blocking agents – hallmark of toxicity is hypotension and bradycardia. Propranolol does have some sodium channel blocking effects, so beware of prolonged QRS
• Class III: Potassium channel blocking agents – acute toxicity is rare, but amiodarone can have lots of long-term effects. Sotalol also has beta-blocking effects
• Class IV: Calcium channel blocking agents – hallmark of toxicity is hypotension, bradycardia, and hyperglycemia
• Recognize that a lot of these drugs cross class lines and have more than one action or effect!
See related Toxcard “Cardiovascular Drug Effects on the Action Potential and ECG“
References:
1. Williams EV. A classification of antiarrhythmic actions reassessed after a decade of new drugs. The Journal of Clinical Pharmacology. 1984;24(4):129-147.
2. Lei M, Wu L, Terrar DA, Huang CL. Modernized classification of cardiac antiarrhythmic drugs. Circulation. 2018;138(17):1879-1896.
3. OpenStax, Anatomy and Physiology. OpenStax CNX. Jan 16, 2020 http://cnx.org/contents/14fb4ad7-39a1-4eee-ab6e-3ef2482e3e22@17.8.
4. Procainamide. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
5. Quinidine. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
6. Mexilitine. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
7. Flecainide. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
8. DeWitt CR, Waksman JC. Pharmacology, pathophysiology and management of calcium channel blocker and β-blocker toxicity. Toxicological reviews. 2004;23(4):223-238.
9. Beta Blocking Agents. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
10. Colatsky TJ, Follmer CH, Starmer CF. Channel specificity in antiarrhythmic drug action. mechanism of potassium channel block and its role in suppressing and aggravating cardiac arrhythmias. Circulation. 1990;82(6):2235-2242. doi: 10.1161/01.cir.82.6.2235 [doi].
11. Amiodarone. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
12. Ibutilide. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
13. Dronedarone. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.
14. Braunwald E. Mechanism of action of calcium-channel-blocking agents. N Engl J Med. 1982;307(26):1618-1627.
15. Calcium Antagonists. In: POISINDEX® System [database online]. Micromedex Solutions. Truven Health Analytics, Inc. Ann Arbor, MI. Available at: http://www.micromedexsolutions.com. Accessed January 21, 2020.






1 thought on “ToxCard: Vaughan-Williams Classification of Anti-Dysrhythmics”
Pingback: ePulse: Highlights of the week 24 April – 1 May 2020 – V E N T R I C L E