Transesophageal Echocardiography in Cardiac Arrest
By Stephen Alerhand MD
Resident Physician, Icahn School of Medicine at Mount Sinai
Edited by Alex Koyfman MD
“Cardiac arrest en route, ETA 5 minutes”, the voice on the other end of the ED phone states. “60 year-old male down for 10 minutes before EMS arrival. Unknown history, no signs of trauma.” The voice hangs up, and you tell the nurse to overhead-page your team for preparation.
The residents rush into the trauma bay. “What’s the call?” they ask.
“Cardiac arrest”, you respond without an air of looming anticipation or uncertainty in your voice. You know the drill and can seemingly visualize the subsequent sequence of events. The ACLS Protocol is but an ingrained reflex in your mind by now. IV, O2, monitor…chest compressions…shock, don’t shock…Epi, Calcium, Bicarb, D50, Insulin…check rhythm, pulse…H’s and T’s…
You have the team halt compressions and stick the ultrasound probe on the patient’s obese chest. The image quality of your transthoracic echocardiography (TTE) is limited, but you discern poor contractility of the heart and then later on cardiac standstill. Your intern asks you how the patient died. You cannot say for sure, and you may not end up knowing. But what if there was a way to better visualize the heart? What if you could see something on the ultrasound screen that triggered a specific and critical intervention?
According to the 2008 ACEP Ultrasound Guidelines, as well as Matt and Mike from the Ultrasound podcast, that emerging emergency ultrasound application is…Transesophageal echocardiography (TEE) in cardiac arrest.
Benefits of TTE
- Determine myocardial contractility and estimate ejection fraction
- Shown to predict negative outcome in those with true echocardiographic asystole upon ED presentation
- Detect critical pathology and direct resuscitative efforts
Disadvantages of TTE
- Inability to scan during chest compressions
- Poor image quality in obese and COPD patients
Benefits of TEE
- High-resolution images not affected by body habitus, emphysema, or subcutaneous air
- Placed into esophagus to give optimal distance and acoustic window for heart
- Constant visualization of the heart during chest compressions, cardioversion (probe is electrically isolated), and other procedures
- Left in place throughout resuscitation with minimal manipulation
- Shorter checks for pulse and cardiac activity
- Live feedback about quality of chest compressions and cardiac contractility
- Better detection of pericardial effusion, tamponade, myocardial rupture, pulmonary embolism, ventricular fibrillation, and other possible etiologies of cardiac arrest that often go missed and would otherwise call for rapid, specific intervention
- Can visualize and evaluate valves, vegetations, diastolic function, adult congenital heart disease, intracardiac masses
- Detail is close enough that right atria thrombi are commonly ruled out by TEE before AFib cardioversion
- Safe technique; most dangerous complication is esophageal perforation (0.03% complication rate)


Absolute Contraindications
- Perforated viscous, esophageal pathology or esophagectomy, UGI bleed or recent UGI surgery
Relative Contraindications
- Cervical spine disease, hiatal hernia, coagulopathy, prior chest radiation
Limitations of TEE
- Increased cost
- More training needed
- Introduction of air between probe and stomach if gastric decompression incomplete
- Mechanical and prosthetic valves will create shadowing and interference similar to that for TTE
Specific Applications of TEE in Cardiac Arrest
Blaivas, Michael. Transesophageal echocardiography during cardiopulmonary arrest in the emergency department. Resuscitation 78 (2008): 135-140.
Brief description of 6 applications described in this paper:
Case 1: TTE showed no cardiac motion. TEE did. Compressions halted, pressors started.
- 35M brought in by EMS undergoing CPR… TTE showed limited view but no cardiac motion. No pulses. TEE showed contraction w/ EF 15%. Thus compressions halted. Pressors started. Extubated and released days later.
Case 2: Monitor showed asystole. TEE showed V-fib and chest compression quality.
- 73 obese F p/w difficulty breathing and hypoxia. Developed tachypnea and decreased alertness. Intubated, then arrested. Monitor showed asystole. Poor images on echo showing cardiac standstill. TEE showed V-fib, thus shock applied. Eventually labs returned with K >9. Hyperkalemia meds given. Providers giving compressions rotated in based upon inadequate compressions on TEE. Eventually developed EF >50%.
Case 3: TTE showed standstill. TEE showed Vfib and thrombus. Given tPA.
- 73F p/w sudden-onset SOB, collapsed, intubated in field. ROSC prior to arrival. Echo showed cardiac standstill. Pulses present. Monitor showed heart beat. TEE showed cardiac standstill, thus CPR restarted. Then showed V-fib, thus patient shocked into ROSC. TEE also showed thrombus leaving RA and entering RV, thus given tPA bolus and started on Heparin.

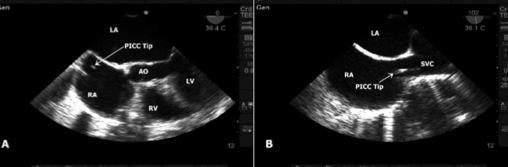
Case 4: TTE showed standstill. TEE showed PICC line catheter tip striking RA. PICC line pulled back.
- 45M receiving Abx through PICC line collapsed shortly after infusion. EMS found in V-fib, CPR started. No pulses. Echo showed standstill. TEE showed V-fib along with catheter tip in entrance to RA periodically striking wall. Thus PICC line pulled back.

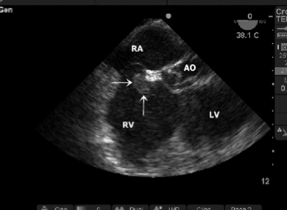
Case 5: TTE showed asystole. TEE showed no RV strain, but rather aortic dissection. TPA held, Thoracic Surg called in.
- 37M PMH DVT and PE 2/2 hypercoagulability disorder c/o cp. Arrested in ED. Echo showed asystole. No pulses. Presumptive diagnosis of PE made. TEE showed no RV strain or ventricular septal movement abnormalities, but rather proximal aortic dissection. TPA thus cancelled, Thoracic Surgery called in for aortic graft placement.
Case 6: TTE suggested acute PE. TEE showed chronic process. TPA held.
- 61F collapsed at home after c/o sob. Pulses lost en route, V-fib, shocked into PEA. Echo showed myocardial contractions with severely depressed function, RA and RV dilation, images limited 2/2 body habitus and emphysema. Monitor showed V-fib, patient shocked. TEE showed minimal R heart strain and no paradoxical movement of septum into LV, consistent w/ chronic RA and RV dilation. No thrombus seen. TPA held.
Performing TEE in Cardiac Arrest
- TEE probe inserted into esophagus, using laryngoscopy if needed


- Controls on handle allow manipulation of US beam for array of visual orientations of heart
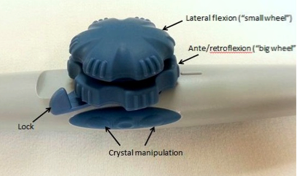

- Maximal penetrating depth of 19-20 cm, with high frequency
Further Reading
- Blaivas, Michael. Transesophageal echocardiography during cardiopulmonary arrest in the emergency department. Resuscitation 78 (2008): 135-140. (referenced above)
- Dawson, Matt. Mallin, Mike. Introduction to Bedside Ultrasound. Chapter 19 – Transesophageal Echo.
- Gruenewald, M. et al. Visual evaluation of left ventricular performance predicts volume responsiveness early after resuscitation from cardiac arrest. Resuscitation 82 (2011); 1553-1557.
- Klouche, K. et al. Echo-Doppler observations during cardiac arrest and cardiopulmonary resuscitations. Crit Care Med. 2000 Nov;28(11 Suppl):N212-3.
- Memtsoudis, SG. et al. The usefulness of transesophageal echocardiography during intraoperative cardiac arrest in noncardiac surgery. Anesth Analg. 2006 Jun;102(6):1653-7.
- Van der Wouw, Poll A. et al. Diagnostic accuracy of transesophageal echocardiography during cardiopulmonary resuscitation. J Am Coll Cardiol 1997;30:780-3.





2 thoughts on “Transesophageal Echocardiography in Cardiac Arrest”
Pingback: LITFL Review 160 - LITFL
Pingback: LITFL Review 160 • LITFL Medical Blog • FOAMed Review