
Authors: Sameer Desai, MD (EM Attending Physician, University of Kentucky); Omar Abbas Ahmed Malik, MBBS (Patients’ Aid Foundation, Jinnah Postgraduate Medical Center) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine in St. Louis); Marina Boushra, MD (EM-CCM Attending Physician, Cleveland Clinic Foundation); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case:
A 39-year-old male is brought in by EMS with a sudden-onset severe headache that started shortly before arrival. He says it is the worst headache he has ever experienced and reports associated neck pain. His GCS is 15 and his neurological examination is without focal abnormality. A non-contrast head computed tomography (CT) demonstrates a diffuse hyperdensity consistent with subarachnoid hemorrhage (SAH). His blood pressure (BP) is 220/120 mmHg. What are the next best steps in BP management for this patient?
I. Introduction:
Neurologic emergencies are common in the Emergency Department (ED), and blood pressure management is critical to immediate management. This article will discuss blood pressure goals and preferred pharmacotherapy for non-traumatic ischemic and hemorrhagic strokes.
II. Ischemic Strokes:
Ischemic stroke is characterized by a blockage of a blood vessel in the brain. BP management in ischemic stroke necessitates striking a delicate balance between maintaining sufficient pressure for cerebral perfusion and minimizing the risk of hemorrhagic transformation, which is significantly increased with high blood pressure.
The BP targets for patients with ischemic strokes depend on the available therapeutic options. The American Heart Association/American Stroke Association (AHA/ASA) recommends maintaining BP below 185/110 mmHg in eligible patients undergoing thrombolytic therapy or endovascular intervention [1]. Following thrombolysis or endovascular therapy, the recommended blood pressure goal is below 180/105 mmHg to prevent hemorrhagic complications [1]. For patients with ischemic strokes who are not candidates for thrombolytic or endovascular therapy, the targets are not as clearly defined. Current guidelines do not recommend acute treatment of hypertension in these patients unless extreme (SBP > 220 mmHg or DBP > 120 mmHg), or another indication is present (e.g. hypertensive emergency, need for thrombolytic administration) [1]. When acute treatment is indicated, cautious BP lowering is suggested (~15% in the first 24 hours) [1-6]. Care should be taken to avoid rapid or frequent fluctuations in blood pressure, which may be better achieved through administering long-acting medications or titratable drips rather than push-dose boluses of short-acting medications when available [1-6]. Optimal blood pressure targets for patients with pre-existing hypertension are still unknown, with some studies suggesting that aggressive blood pressure lowering may not be beneficial and could even be harmful in this patient population who may have become dependent on higher cerebral perfusion pressures [3,6].
A. Hemorrhagic Conversion of Ischemic Stroke:
Hemorrhagic conversion of ischemic stroke, a rare but serious complication, occurs when the ischemic tissue bleeds into the surrounding brain parenchyma. This can worsen neurological deficits and significantly increase mortality. The management of blood pressure in this condition is controversial and depends on several factors, such as the size and location of the hemorrhage, the presence of symptoms, and the risk of re-bleeding or hematoma expansion. According to some sources, the recommended blood pressure target for patients with hemorrhagic conversion is less than 160 mmHg systolic blood pressure or less than 110 mmHg mean arterial pressure. These targets can be achieved by using short-acting, titratable intravenous medications such as beta-blockers or nicardipine [1]. However, other sources suggest that the optimal blood pressure target is not well established and may vary depending on the individual patient’s characteristics and the type of hemorrhagic transformation [7]. It is important to monitor the blood pressure closely and adjust the treatment accordingly, keeping in mind the principles of maintaining adequate cerebral perfusion and preventing further bleeding. Aggressive blood pressure lowering should be avoided to prevent additional brain damage from ischemia [1, 4,6]. In addition to blood pressure control, management strategies should include anticoagulation reversal, neurosurgical consultation, and treatment and prevention of known complications. If the patient is taking anticoagulants, reversal agents immediately should be administered to minimize bleeding risk and hematoma expansion. In some cases, surgical evacuation of the hematoma or procedures to relieve intracranial pressure may be necessary; early neurosurgical consultation in patients with hemorrhagic conversion is recommended. Finally, anticipating and addressing known complications such as seizures, increased intracranial pressure, or cerebral edema with appropriate measures, including antiepileptic drugs or osmotic agents, is essential for improving patient outcomes.
III. Intracerebral hemorrhage (ICH):
ICH is the second most common cause of stroke, following ischemic stroke, but accounts for a disproportionate amount of cerebrovascular mortality and morbidity [8]. This includes intraparenchymal hemorrhage and subarachnoid hemorrhage (SAH). Injury to brain parenchyma occurs via hematoma expansion and perilesional edema as well as secondary excitotoxic and inflammatory injury from the breakdown of the blood-brain barrier[8]. Major risk factors for spontaneous ICH include older age, hypertension, and the use of antithrombotic (antiplatelet and anticoagulant) therapy [8]. The goals of initial treatment include preventing hemorrhage expansion, monitoring for and managing elevated intracranial pressure, and managing other neurologic and medical complications.
Neuroimaging with head CT or magnetic resonance imaging (MRI) is mandatory to confirm the diagnosis of ICH and to exclude ischemic stroke and stroke mimics as alternative causes to symptoms [8]. CT angiography may be performed along with a non-contrast head CT to help identify an underlying vascular cause to the ICH [8]. Acute imaging also provides information about the severity of the hemorrhage, the risk of expansion of bleeding, and the underlying cause of the ICH. Predictors of hemorrhage growth associated with neurologic deterioration include a shorter time from symptom onset to initial imaging, initial ICH volume, antithrombotic medication use, and imaging signs of ICH heterogeneity on non-contrast CT or focal contrast extravasation on CT angiography [8].
Poor blood pressure management can worsen the outcome of hemorrhagic stroke by increasing the risk of hematoma expansion, cerebral edema, and ischemia [8-14]. However, lowering blood pressure too aggressively or too early may also have harmful effects, such as reducing cerebral perfusion, impairing autoregulation, and inducing hypoperfusion [8,9,11]. The current guidelines for blood pressure management in hemorrhagic stroke are based on the results of several large randomized trials, including the INTERACT-2, ATACH-2, and SCAST trials [8,11,14,15]. These trials have shown that blood pressure lowering is safe and may improve functional outcomes in patients with hemorrhagic stroke, especially in those with intracerebral hemorrhage (ICH) and systolic blood pressure of 150-220 mmHg [11,14,15]. The AHA/ASA guidelines recommend that in patients with ICH and systolic blood pressure of 150-220 mmHg, blood pressure should be lowered to a target of 140 mmHg within the first 24 hours of symptom onset, using short-acting, titratable intravenous medications such as beta-blockers or calcium channel blockers [8]. In patients with systolic blood pressure of ≥220 mmHg, blood pressure should be reduced by 15% in the first hour, using continuous intravenous infusion and frequent blood pressure monitoring to avoid large fluctuations, and then maintained at 180 mmHg or less until 24 hours after onset [8].
A. Aneurysmal SAH and Delayed Cerebral Ischemia:
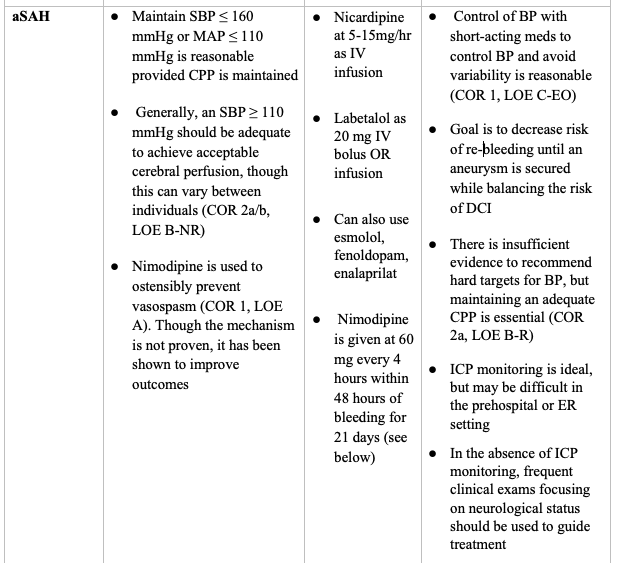
SAH secondary to aneurysm rupture is an important category of intracerebral hemorrhage for which studies have shown that blood pressure management can be slightly more liberal to maintain adequate cerebral perfusion pressure [19]. The current guidelines recommend a blood pressure target of SBP ≤ 160 mmHg or MAP ≤ 110 mmHg, provided there is no evidence of compromise of cerebral perfusion pressure [16-18]. An SBP ≥ 110 mmHg should typically be adequate to achieve acceptable cerebral perfusion, though this can vary between individuals [16-18].
DCI is a significant cause of delayed morbidity and mortality in patients with aneurysmal SAH, most commonly occurring secondary to cerebral vasospasm [20]. DCI is defined as focal neurological impairment or a decrease of at least 2 points on the Glasgow Coma Scale lasting at least 1 hour that cannot be attributed to aneurysm occlusion or other causes using clinical assessment, CT /MRI scanning of the brain, and laboratory studies [16]. It manifests around 4-10 days post-SAH, and treatment should be started within 48 hours and continue for 21 days [16]. Meta-analyses of randomized trials of prophylactic nimodipine administered for SAH have consistently noted a benefit in odds of deficit and mortality [20-23].
IV. Summary:
Table I summarizes the current recommendations and the strength of evidence for blood pressure management in patients with non-traumatic ischemic and hemorrhagic strokes.
Table I: Blood pressure management in non-traumatic strokes:



V. Pearls and Pitfalls:
- BP management in ischemic strokes must strike a delicate balance between preventing ischemic conversion and maintaining adequate cerebral perfusion pressure to viable tissue.
- Significantly elevated BP can worsen ICH by causing continued or recurrent bleeding. Lowering the MAP may mitigate these risks and possibly improve outcomes.
- Rapid BP reduction could promote cerebral and systemic hypoperfusion. Reduce elevated BP slowly while monitoring for clinical deterioration to maintain adequate cerebral and systemic perfusion.
- Nimodipine has been shown to have morbidity and mortality benefits through the reduction of DCI in patients with aneurysmal SAH.
Case Resolution:
In addition to standard measures for resuscitation, the patient is started on a nicardipine drip to target an SBP < 160 mmHg and neurosurgery is urgently consulted. Neurosurgery takes the patient to surgery after the CT angiogram suggests aneurysmal rupture.
References:
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019; 50:e344.
- Leonardi-Bee J, et al; IST Collaborative Group. Blood pressure and clinical outcomes in the International Stroke Trial. Stroke. 2002 May;33(5):1315-20. doi: 10.1161/01.str.0000014509.11540.66. PMID: 11988609.
- Okumura K, et al. Effects of blood pressure levels on case fatality after acute stroke. J Hypertens. 2005 Jun;23(6):1217-23. doi: 10.1097/01.hjh.0000170385.76826.4a. PMID: 15894898.
- Oliveira-Filho J, et al. Detrimental effect of blood pressure reduction in the first 24 hours of acute stroke onset. Neurology. 2003 Oct 28;61(8):1047-51. doi: 10.1212/01.wnl.0000092498.75010.57. PMID: 14581662.
- Vlcek M, et al. Association between course of blood pressure within the first 24 hours and functional recovery after acute ischemic stroke. Ann Emerg Med. 2003 Nov;42(5):619-26. doi: 10.1016/s0196-0644(03)00609-7. PMID: 14581913.
- Castillo J, et al. Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome. Stroke. 2004 Feb;35(2):520-6. doi: 10.1161/01.STR.0000109769.22917.B0. Epub 2004 Jan 15. PMID: 14726553.
- Yaghi S, Willey JZ, Cucchiara B, Goldstein JN, Gonzales NR, Khatri P, Kim LJ, Mayer SA, Sheth KN, Schwamm LH; on behalf of the American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Quality of Care and Outcomes Research. Treatment and outcome of hemorrhagic transformation after intravenous alteplase in acute ischemic stroke: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2017;48:e343–e361. DOI: 10.1161/STR.0000000000000152.
- Greenberg SM, Ziai WC, et al. American Heart Association/American Stroke Association. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2022 Jul;53(7):e282-e361. doi: 10.1161/STR.0000000000000407. Epub 2022 May 17. PMID: 35579034.
- Divani AA, et al. Blood Pressure Variability Predicts Poor In-Hospital Outcome in Spontaneous Intracerebral Hemorrhage. Stroke. 2019 Aug;50(8):2023-2029. doi: 10.1161/STROKEAHA.119.025514. Epub 2019 Jun 20. PMID: 31216966.
- Zhang Y, et al. Blood pressure and clinical outcome among patients with acute stroke in Inner Mongolia, China. J Hypertens. 2008 Jul;26(7):1446-52. doi: 10.1097/HJH.0b013e328300a24a. PMID: 18551022.
- Manning L, et al.; INTERACT2 investigators. Blood pressure variability and outcome after acute intracerebral haemorrhage: a post-hoc analysis of INTERACT2, a randomised controlled trial. Lancet Neurol. 2014 Apr;13(4):364-73. doi: 10.1016/S1474-4422(14)70018-3. Epub 2014 Feb 13. PMID: 24530176.
- Ohwaki K, et al. Blood pressure management in acute intracerebral hemorrhage: relationship between elevated blood pressure and hematoma enlargement. Stroke. 2004 Jun;35(6):1364-7. doi: 10.1161/01.STR.0000128795.38283.4b. Epub 2004 Apr 29. PMID: 15118169.
- Sakamoto Y, et al.; SAMURAI Study Investigators. Systolic blood pressure after intravenous antihypertensive treatment and clinical outcomes in hyperacute intracerebral hemorrhage: the stroke acute management with urgent risk-factor assessment and improvement-intracerebral hemorrhage study. Stroke. 2013 Jul;44(7):1846-51. doi: 10.1161/STROKEAHA.113.001212. Epub 2013 May 23. PMID: 23704107.
- Qureshi AI, et al.; ATACH-2 Trial Investigators and the Neurological Emergency Treatment Trials Network. Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage. N Engl J Med. 2016 Sep 15;375(11):1033-43. doi: 10.1056/NEJMoa1603460. Epub 2016 Jun 8. PMID: 27276234; PMCID: PMC5345109.
- Hankey G. J. (2011). Lowering blood pressure in acute stroke: the SCAST trial. Lancet (London, England), 377(9767), 696–698. https://doi.org/10.1016/S0140-6736(11)60163-3
- Connolly ES, et al. Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711-1737. doi:10.1161/STR.0b013e3182587839
- Diringer MN, et al.; Neurocritical Care Society. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care. 2011 Sep;15(2):211-40. doi: 10.1007/s12028-011-9605-9. PMID: 21773873.
- Wijdicks EF, et al. The effects of treating hypertension following aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 1990;92(2):111-7. doi: 10.1016/0303-8467(90)90085-j. PMID: 2163791.
- van Gijn J. Subarachnoid haemorrhage. Lancet. 1992 Mar 14;339(8794):653-5. doi: 10.1016/0140-6736(92)90803-b. PMID: 1347345.
- William S. Dodd, et al. Pathophysiology of Delayed Cerebral Ischemia After Subarachnoid Hemorrhage: A Review; 30 Jul 2021; Journal of the American Heart Association. 2021;10:e021845; https://doi.org/10.1161/JAHA.121.021845
- Barker FG 2nd, Ogilvy CS. Efficacy of prophylactic nimodipine for delayed ischemic deficit after subarachnoid hemorrhage: a metaanalysis. J Neurosurg. 1996 Mar;84(3):405-14. doi: 10.3171/jns.1996.84.3.0405. PMID: 8609551.
- Feigin VL, et al. Calcium antagonists in patients with aneurysmal subarachnoid hemorrhage: a systematic review. Neurology. 1998 Apr;50(4):876-83. doi: 10.1212/wnl.50.4.876. PMID: 9566366.
- Dorhout Mees et al. Calcium antagonists for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev. 2007 Jul 18;2007(3):CD000277. doi: 10.1002/14651858.CD000277.pub3. PMID: 17636626; PMCID: PMC7044719.
- American Heart Association. Applying Class of Recommendations and Level of Evidence to Clinical Strategies, Interventions, Treatments, or Diagnostic Testing in Patient Care.; 2019. Accessed July 19, 2023. https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines/tables/applying-class-of-recommendation-and-level-of-evidence




