
Authors: Saran S. Pillai, MBBS (@sspillai01, EM Resident Physician, University of Kentucky) and Christopher N. Belcher, MD (EM Attending Physician, University of Kentucky, Department of Emergency Medicine) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
“What do you call an IV contrast shortage? A baby formula milk shortage for adults.”
– Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula).
Introduction
The lack of contrast media in the year 2022 had a substantial worldwide influence, resulting in a diminished supply of iodinated contrast media (ICM) utilized in medical imaging techniques. The principal factor contributing to the scarcity was the temporary closure of a GE Healthcare manufacturing facility in Shanghai, China, as a result of a COVID-19-induced lockdown.1 The shortage in supply posed difficulties for hospitals that significantly depend on GE Healthcare as their supplier, which encompassed approximately 50% of hospitals in the United States (US).2 In response to the constrained availability of contrast media, emergency medicine (EM) and radiology departments were compelled to enact modifications in their imaging techniques. The scarcity also underscored the susceptibility of the healthcare supply chain and the necessity for proactive approaches to alleviate such interruptions in subsequent instances. The primary aim of this article is to examine the clinical insights derived from scarcity and its consequences.
Background and Context
Contrast-enhanced computed tomography (CECT) is of paramount importance in the emergency department (ED) due to its indispensable role in facilitating precise diagnostic outcomes. CECT is preferred over non-contrast (NC) computed tomography (CT), as the intravenously administered contrast aids in highlighting active bleeding and vascular disruptions in trauma, vascular abnormalities, tumors, infections/inflammatory processes and their complications, vascular pathology, distinguishes between solid masses and fluid collections, identifies coronary artery disease through CT coronary angiography (CTCA), identifies ischemic pathology including stroke and bowel ischemia, and is necessary for the CT angiography (CTA) diagnosis of pulmonary embolism (PE).
CT scans have become an integral part of the ED diagnostic process, serving as a diagnostic tool to aid in determining appropriate disposition, risk assessment, and guiding admission decisions.3 A study of CT use trends in the ED has shown increasing use of CTs by almost 60% from 2005 to 2013.3 EDs have also been increasingly supporting primary care providers in the US by helping with diagnostic workups that cannot be performed in physician offices.
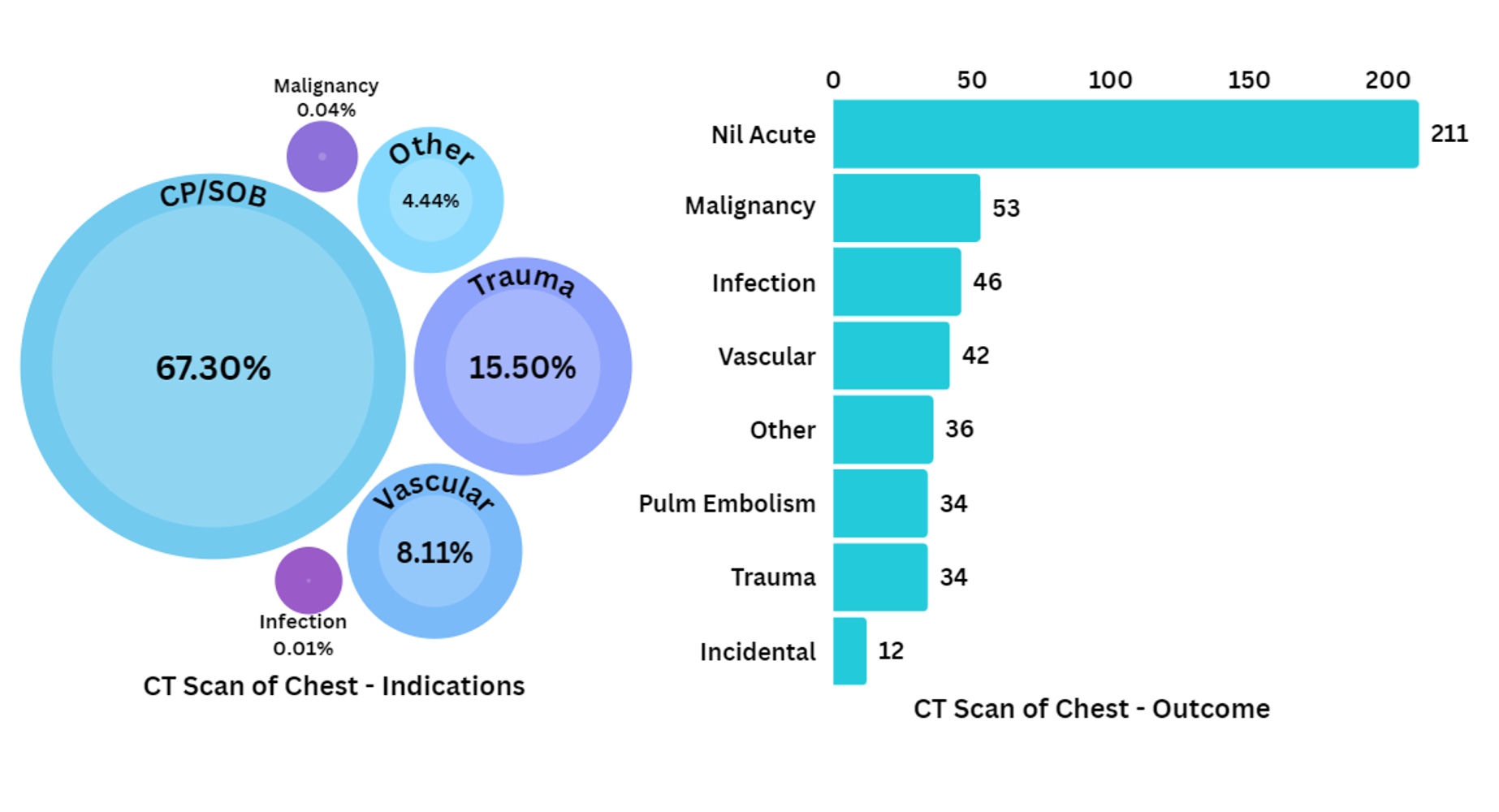
Figure 1. Relative proportions of reported diagnostic indications versus clinical outcomes in a retrospective analysis of all CT imaging in 3 EDs over 1 year at an academic center.4



The Contrast Media Shortage of 2022
The ICM shortage in 2022 had significant implications for EM, since making time-sensitive medical and surgical diagnoses required modification in the setting of limited contrast reserves. Hospitals served by GE Healthcare were warned in April 2022 of an 80% order fulfillment shortage of both Omnipaque (Iohexol) and Visipaque (Iodixanol) which accounted for 50% of the US market and 75% of the Australian market share of contrast used in CT scans, interventional radiology, and the cardiac catheterization lab.5,6 By May 2022, GE had reopened the Shanghai plant by following local covid work protocols, enabling more workers to return back and boosted output at the Shanghai plant from 0% to 60%. Production levels increased steadily back to baseline, achieving normal supply levels in February 2023.7
The iodinated contrast scarcity underscored the need for cooperation among healthcare systems, hospitals, and manufacturers to tackle weaknesses in the supply chain and formulate backup strategies, which can be applied to future supply shortages impacting EM.
Clinical Lessons Learned
Practical strategies for optimizing contrast media utilization
On May 6, 2022, the Committee on Drugs and Contrast Media of the American College of Radiology (ACR) issued a statement proposing guidelines for healthcare professionals to address the anticipated scarcity of contrast media.8 In response to the ongoing scarcity, an increased number of recommendations were released by leaders in the field, with a tier-based categorization of indications for contrast use in the setting of the impending shortage.11
Table 1. Risk mitigation strategies proposed by ACR during an iodinated contrast shortage for CT scans.

Preparation9
Hospitals had to prepare for the impending contrast shortage as soon as potential shortage news occurred. In most cases, the radiology team functioned as the main decision-maker playing a key role in drafting institutional protocols. At many institutions, pharmacy was responsible for centralized inventory management, conversion of single use vials to multiuse etc., while Information technology (IT) helped manage communications about the shortage.10
Use of Existing Data: Hospitals used electronic medical records and purchasing data to establish accurate historical ICM consumption rates. This information helped predict how long current ICM inventories would last.
Determining Critical Supply Threshold: Hospitals determined the volume of contrast material required to provide the standard of care for all critical CECT examinations through the end of June 2022. This number served as a facility’s critical supply threshold at the current contrast usage rate for critical scans.
Establishing Conservation Benchmarks: Hospitals established additional benchmarks for conservation efforts by working backward from the critical supply threshold. These benchmarks were based on the projected days of remaining ICM supply and internal modeling of how specific reduction strategies would affect historical ICM usage rates.
The conservation strategies discussed during the first few months of contrast shortage included
- Direct Reduction
- Use of Alternative Contrast Agents
- Waste Minimization
- Change to NCCT
- Use of Alternative Imaging Modalities
- Deferment of Imaging
1) Direct Reduction
Several methods can be used to reduce the amount of contrast media used in CT imaging (Table 2).
Table 2. Direct methods used to reduce contrast media usage in CT imaging.9

2) Use of alternative contrast agents
Table 3. Alternative contrast agents.9,13

3) Switch to a NCCT scan
CECT has been long considered to outperform NCCT in acute trauma and acute abdominal emergencies and has thus been referred by ED physicians to rule out life-threatening emergencies. A necessity-based tier system with consideration for contrast availability was implemented by radiology departments during the contrast shortage (Table 4).
Table 4. Necessity-based system prioritizing CT contrast usage for emergent conditions (modified for ED-relevance).9,10,12,15

Orders for ICM in any indications other than Tier 1 needed prior authorization from radiology to discuss the need on a case-by-case basis. Some institutions developed a tier-based system for outpatient imaging as well which was updated in real-time.10
One of the significant changes brought about by the crisis was that clinicians began to review the necessity of contrast for CT scans. Clinicians were encouraged to question whether a NCCT provided an adequate answer to the clinical query. If there are no limitations linked to body habitus (i.e. lack of intra-abdominal fat), several of the clinical indications of CECT – most frequently abdominal pain and minor trauma – can be addressed with a NCCT with sufficient accuracy.16 In a study conducted by Millet et al. involving 401 consecutive patients aged 75 years or older who were admitted to the ED with acute abdominal symptoms, CECT provided additional relevant and accurate information in only 6.4% (n=14) of patients who underwent both unenhanced and enhanced CT scans. This additional information resulted in a change in management for 1.4% (n=3) of the study population.17 Other studies have demonstrated the lack of necessity for contrast CT studies for other indications including flank pain,18 appendicitis,19 diverticulitis,20 bowel obstruction21, and generalized non-traumatic abdominal pain.22
A single center retrospective study23 during the period of contrast shortage looking at the rate of missed acute diagnoses using NCCT abdomen and pelvis in 424 ED patients with abdominal pain, falls, or motor vehicle collision (MVC)-related trauma supports the adequacy of NCCT. Of the 96 patients (22.6%) who received follow-up imaging, NCCT was done in 28/96 and CECT in 22/96 of the patients. 97% (93/96) of cases had confirmation of the original report findings with only one clinically significant finding among the three missed findings (3/96).
At the same time, newer research has shown that the diagnostic safety despite withholding contrast in abdominal pain may actually be overstated. A retrospective study done in May 2023, by Shaish et al24 showed a 30 % reduction in accuracy of NCCT compared to CECT in a study done among 201 adult ED patients with abdominal pain. Patients underwent dual-energy contrast-enhanced CT and blinded interpretation by radiologists, following which digital subtraction of contrast using dual-energy techniques was done. Six different blinded radiologists from 3 institutions (3 faculty and 3 residents) interpreted the resulting unenhanced CT examinations. Overall accuracy of unenhanced CT was 70% (faculty, 68% to 74%; residents, 69% to 70%). This study had a number of limitations, particularly the fact that it is unclear how digital subtraction of contrast compares to true NCCT. However, until more research data is available on this, the results suggest that clinicians should use caution not to overly rely on NCCT to exclude serious intraabdominal pathology.
4) Utilization of Alternative Imaging Technique
Table 5. Utilization of alternative imaging techniques.9,15,25–27

Changing protocols to US, MRI or other modalities may require increased staffing. Approval from insurance companies and third-party payers poses another challenge particularly when the only available alternative to CT is MRI.
Figure 2. Change in trend of ordering patterns during the first 14 days after implementation of ICM-conserving strategies compared with the preceding 12 months. Retrospective study done by Monash University in Melbourne (largest radiology department in Australia) (Average daily scans plotted).12 CECT – Contrast enhanced CT, CTPA – CT Pulmonary Angiography, Abdp – Abdomen and Pelvis, NCCT – Non contrast enhanced CT, VQ scan – Ventilation Perfusion Scan

5) Waste reduction
ICM waste reduction is a high-yield tactic for extending the current supply. Under standard operating protocols, residual contrast materials are usually wasted, according to current CDC and JC standards.27
In situations when reusing vials is not an option, practices should consider this and adjust dose regimens based on available vial volumes to prevent wastage. Normal CECT scans utilize iodinated contrast at 300 mg/mL concentrations with an average adult receiving 80–150 mL of contrast for most indications and pediatric age group patient receiving 1 mL/lb body weight.28 In the setting of severe shortage, any off-label use of single-use vials for more than one patient should be implemented in collaboration with pharmacists and compliance officers to preserve adherence to sterile standards. Aseptic tubing systems to preserve and repackaging in smaller aliquots were just a few of the several methods employed to cut down on contrast waste.29
6) Postponing imaging
Delaying imaging is an option in patients who are at low risk for life-threatening emergencies. However, this poses an inherent danger similar to the initial Covid-19 lock-down stages when patients were lost to follow-up and later presented with late-stage disease. Very few guidelines regarding the appropriateness of deferment are available but some institutions did create a tier-based system for outpatient imaging in the setting of severe contrast shortage.10
Communication and guidance
Interdisciplinary teams at each institution play a key role in developing protocols and guidelines for prioritizing and rationing contrast media based on the critical supply threshold. Guidance and recommendations provided by professional organizations, such as the ACR were crucial in optimizing contrast media usage.8 Electronic health record (EHR) interventions including order-based interventions and alerts were proven to reduce contrast utilization by reminding providers about the shortage as well as recommending alternative imaging modalities. A 12% reduction in CECTs performed was recorded after EHR interventions in a large health system encompassing 12 hospitals including academic and community medical centers.30 In our healthcare system, decisions regarding outpatient CECT postponement were mostly spearheaded by the radiology department in collaboration with other departments. An appeals process to the CMO-on-call also existed to evaluate specific cases that did not fit within the standard triage process. In all cases, providers were encouraged to discuss cases with the radiologist on-call regarding alternative imaging. The significance of effective communication and collaboration between emergency physicians, radiologists, and other healthcare providers during times of contrast media shortage cannot be understated.
Effectiveness conservation strategies
A systematic review reviewing “ICM shortage” and its effectiveness among 22 papers published based on the event found that the overall reduction of ICM usage in these studies ranged from 50-80%; reduction of CECTs performed ranged from 12-85%; and reduction of ICM volume per scan from 16-93%.6 The reduction of the number of CECTs performed contributed more to the overall result than any other intervention, followed by direct ICM dose reduction and deferment of diagnostic imaging.6,9
Patient Safety Considerations
Few studies have evaluated the impact of the contrast shortage on patient care or patient-centered outcomes due to deferment of imaging or changing protocols leading to delayed or missed diagnosis. More studies regarding the same need to be done. The only retrospective study from this period with regards to contrast use versus NCCT in acute abdominal emergencies showed a clinically significant outcome difference (admit vs discharge) in 1% of patients who underwent repeat scans for the same complaint (1/96)23. Protocols could establish strategies for mitigating patient safety concerns during shortages, including close monitoring and follow-up of patients who receive alternative imaging studies.
Take-Home Points:
- The 2022 contrast media scarcity sparked discussion of contrast necessity, conserving use, overuse in current protocols, and alternate imaging techniques.
- Reducing CECT performance, ICM dose reduction, and deferment of diagnostic imaging are strategies to combat contrast shortage.
- In acute ICM contrast shortages, a tier-based necessity system may preserve contrast for emergent studies such as stroke, hemodynamically unstable trauma, aortic dissection, AAA rupture, active GI bleed, PE, acute mesenteric ischemia, etc.
- A NCCT scan may be performed for diverticulitis, appendicitis, hernia, intestinal obstruction/perforation, and hemodynamically stable trauma patients.
- Alternative imaging studies may be considered in select cases after discussion with radiology depending on feasibility, time delay, and patient stability.
- Institutional interdisciplinary teams should develop protocols and guidelines for prioritizing and rationing contrast media in the event of future shortages.

References
- Abelson R. Patients Face Long Delays for Imaging of Cancers and Other Diseases. The New York Times. https://www.nytimes.com/2022/05/26/health/dye-contrast-scan-shortage.html. Published May 26, 2022. Accessed August 10, 2023.
- FDA reports shortage of GE contrast media for CT imaging | AHA News. Accessed August 10, 2023. https://www.aha.org/news/headline/2022-05-10-fda-reports-shortage-ge-contrast-media-ct-imaging
- Bellolio MF, Heien HC, Sangaralingham LR, et al. Increased Computed Tomography Utilization in the Emergency Department and Its Association with Hospital Admission. West J Emerg Med. 2017;18(5):835-845. doi:10.5811/westjem.2017.5.34152
- Retrospective Analysis of Emergency Computed Tomography Imaging Utilization at an Academic Centre: An Analysis of Clinical Indications and Outcomes. Canadian Association of Radiologists Journal. 2019;70(1):13-22. doi:10.1016/j.carj.2018.10.004
- ASNC update regarding iohexol and iodixanol. Accessed August 10, 2023. https://www.asnc.org/files/Vznt_MS_%20Iohexol-(Omnipaque)-and-iodixanol-(Visipaque)-solution_0522%20_update.pdf
- GE Healthcare update on iodinated contrast media | GE News. Accessed August 10, 2023. https://www.ge.com/news/press-releases/ge-healthcare-update-on-iodinated-contrast-media
- Statement from the ACR Committee on Drugs and Contrast Media. Accessed August 10, 2023. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Contrast-Media-Shortage
- Allen LM, Shechtel J, Frederick-Dyer K, et al. Rapid Response to the Acute Iodinated Contrast Shortage During the COVID-19 Pandemic: Single-Institution Experience. Journal of the American College of Radiology. 2022;19(7):836-840. doi:10.1016/j.jacr.2022.05.005
- Cavallo JJ, Pahade JK. Practice Management Strategies for Imaging Facilities Facing an Acute Iodinated Contrast Media Shortage. Published online 2022. doi:10.2214/AJR.22.27969
- Thomas M. Grist, Cheri L. Canon, Elliot K. Fishman, Maureen P. Kohi, and Mahmud Mossa-Basha Short-, Mid-, and Long-term Strategies to Manage the Shortage of Iohexol Radiology 2022 304:2, 289-293
- ACR Appropriateness Criteria®. Accessed August 10, 2023. https://www.acr.org/Clinical-Resources/ACR-Appropriateness-Criteria
- Amukotuwa SA, Jackson D, Bammer R. Impact of iodinated contrast media conserving interventions and lessons for the future. Published online 2022. doi:10.1111/1754-9485.13458
- Nadolski GJ, Stavropoulos SW. Contrast alternatives for iodinated contrast allergy and renal dysfunction: options and limitations. J Vasc Surg. 2013;57(2):593-598. doi:10.1016/j.jvs.2012.10.009
- Keefe NA, Desai KR, Kohi MP, Salazar GM. Mitigation Strategies for Interventional Radiology During a Global Contrast Media Shortage. Journal of Vascular and Interventional Radiology. 2022;33(9):1021-1024. doi:10.1016/j.jvir.2022.05.011
- Amukotuwa SA, Bammer R, Jackson DM, Sutherland T. Iodinated contrast media shortage: Insights and guidance from two major public hospitals. Journal of Medical Imaging and Radiation Oncology. 2022;66(7):946-956. doi:10.1111/1754-9485.13444
- Narita C, Clements W, Varma D. Assessing the necessity of intravenous contrast for computed tomography in the acute undifferentiated abdomen. Journal of Medical Imaging and Radiation Oncology. n/a(n/a). doi:10.1111/1754-9485.13559
- Millet I, Sebbane M, Molinari N, et al. Systematic unenhanced CT for acute abdominal symptoms in the elderly patients improves both emergency department diagnosis and prompt clinical management. Published online 2016. doi:10.1007/s00330-016-4425-0
- Agarwal MD, Levenson RB, Siewert B, Camacho MA, Raptopoulos V. Limited added utility of performing follow-up contrast-enhanced CT in patients undergoing initial non-enhanced CT for evaluation of flank pain in the emergency department. Emerg Radiol. 2015;22(2):109-115. doi:10.1007/s10140-014-1259-4
- Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review – PubMed. Accessed August 12, 2023. https://pubmed.ncbi.nlm.nih.gov/19733421/
- Tack D, Bohy P, Perlot I, et al. Suspected acute colon diverticulitis: imaging with low-dose unenhanced multi-detector row CT. Radiology. 2005;237(1):189-196. doi:10.1148/radiol.2371041432
- Vernuccio F, Picone D, Scerrino G, et al. Intravenous Contrast Agent in Abdominal CT: Is It Really Needed to Identify the Cause of Bowel Obstruction? Proof of Concept. Published online 2019. doi:10.1155/2019/2350948
- Salameh S, Antopolsky M, Simanovsky N, Arami E, Hiller N. Use of Unenhanced Abdominal Computed Tomography for Assessment of Acute Non-Traumatic Abdominal Pain in the Emergency Department. Isr Med Assoc J. 2019;21(3):208-212.
- Calimano-Ramirez LF, Hernandez M, Singh A, et al. Quality assurance for non-contrast CT of the abdomen and pelvis during a period of supply chain disruption leading to iodinated contrast shortage in the emergency department setting. Published online 2023. doi:10.25259/JCIS_142_2022
- Shaish H, Ream J, Huang C, et al. Diagnostic Accuracy of Unenhanced Computed Tomography for Evaluation of Acute Abdominal Pain in the Emergency Department. JAMA Surg.2023;158(7):e231112. doi:10.1001/jamasurg.2023.1112
- Gopireddy DR, Virarkar M, Vulasala SSR, Caro D, Norse A, Rao D. Metrics-driven successful strategy by emergency and radiology driven task force to mitigate global CT contrast media shortage in a safety net hospital. Published online 2023. doi:10.25259/JCIS_116_2022
- Starekova J, Chu SY, Bluemke DA, et al. MR Angiography as the Preferred Test for Pulmonary Embolism During the Iodinated Contrast Media Shortage of 2022: A Single-Center Experience. AJR Am J Roentgenol. Published online June 21, 2023. doi:10.2214/AJR.23.29340
- Pepin EW, Unachukwu E, Schultz S, Ananthakrishnan L. Optimization of iodinated contrast media inventory management: effect of inventory diversification on waste reduction. J Am Coll Radiol. Published online August 3, 2023:S1546-1440(23)00544-6. doi:10.1016/j.jacr.2023.06.032
- Hartman, R.P., King, B. (2008). Contrast Media, Iodinated, Dose, and Administration. In: Baert, A.L. (eds) Encyclopedia of Diagnostic Imaging. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-35280-8_612
- Eibschutz LS, Gholamrezanezhad A. How low can we go? Strategies and recommendations to combat the iodinated contrast shortage. Emerg Radiol. 2022;29(5):925-928. doi:10.1007/s10140-022-02077-7
- Glazer DI, Lucier DJ, Sisodia RC, Sharma A, Gervais DA, Park L, Abbasi N, Hubbell HT, Kapoor N, Flores EJ, Saini S, Khorasani R. Electronic Health Record Order Entry-Based Interventions in Response to a Global Iodinated Contrast Media Shortage: Impact on Contrast-Enhanced CT Utilization. AJR Am J Roentgenol. 2023 Jan;220(1):134-140. doi: 10.2214/AJR.22.28143. Epub 2022 Aug 3. PMID: 35920705.




