
Authors: Sarah Shaver, MD, Tony Mathew, MD, and Dylan Beams, MS3 (EM Resident Physicians and Medical Student, UTSW, Dallas, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
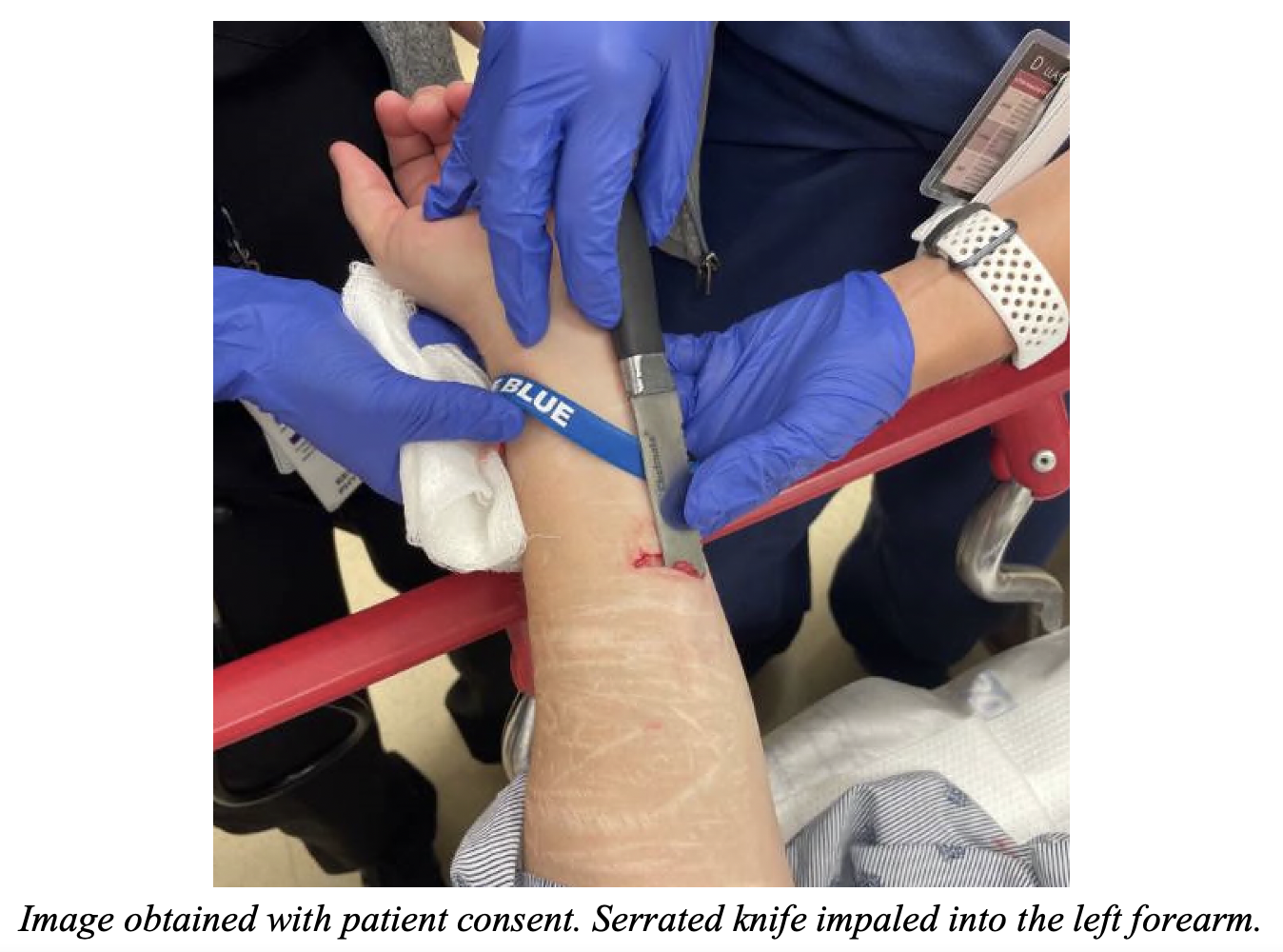
A 60-year-old female presents to the ED with an impaled object in her arm. She reports stabbing herself in the left arm as an act of self-harm, prior to calling EMS. She reports pain and scant bleeding from the injury site. She left the object in her arm due to fear that removing it would cause more injury. The object was wrapped in gauze by EMS, and she was transported to the ED.
On initial assessment on arrival vital signs are BP 150/90, HR 86, RR18, SpO2 96% on RA. She is alert and oriented, talking in complete sentences, bilateral breath sounds are clear, and she has 2+ pulses in the upper extremities. Under extensive gauze wrapping, there is a large, serrated knife impaled in the distal aspect of the left flexor forearm. It is superficial and can be easily palpated along the skin. There are no other injuries identified on primary and secondary surveys. Her left arm as a 2+ radial pulse, along with brisk capillary refill, intact sensory and motor function to distal hand and fingers.
What is the next step in your evaluation and management?
Answer: This is an impaled foreign object. After completion of a thorough primary and secondary survey, evaluate the depth of injury and likelihood of deeper neurovascular injury. If the patient is stable, consider further imaging through x-ray, CT scan, or ultrasound. If the patient is unstable and no other source is identified, assume hemorrhagic source, begin resuscitation, and emergent OR evaluation should be pursued.
Background:
- Traumatic injuries are the leading cause of death in the U.S. for those between the ages of 1-44 years. Approximately 9.5% of traumatic injuries are due to penetrating trauma, most commonly gunshot wounds and stabbings. A minority of these penetrating injures are due to impaled objects, while these instances are rare, the exact number is unknown1-3.
- An impaled object is defined as a foreign body that penetrates and remain embedded within the body4.
- Impaled objects to the thorax or abdomen can result in significant morbidity and mortality, while impaled objects to the extremities typically have injuries limited to the site and trajectory of penetration3.
- Knives are the most frequently cited cause of hand tool trauma, with 8,250,914 knife-related injuries treated in U.S. EDs between 1990 to 2008 5,6.
Out of hospital management:
- The impaled object should be left in place and stabilized for transport to limit further movement or damage7.
- Patients impaled by large objects such as fence poles or large metal shrapnel may require the impaled object to be removed from the primary structure or cut to a smaller size for safe transportation. If this is the case, special care should be made to limit movement or heat by the tools used to cut the impaled object8.

- If an impaled object in an extremity results in severe hemorrhage, application of a tourniquet proximal to the site of injury should be considered9.
- Complex impalements are those which the impaled object is limiting extrication and transport of the patient. These are unique, individualized, situations in which decisions to remove the patient from the impaled object to allow for transportation and care should be made between the EMS team and an experienced physician7,10.
Pathophysiology:
- The impaled object has the risk of causing significant injury, which is dictated by the type of object, mechanism of injury, and location of penetration.
- Injuries due to impaled objects in the extremities result in the risk of nerve, vascular, or bony injury.
- Injuries due to impaled objects in the thorax may lead to significant vascular, cardiac, or pulmonary injury.
- Injuries due to impaled objects in the abdomen may result in significant vascular, hollow, or solid viscera injury.
- If there is vascular injury, the impaled object may hide injury or hemorrhage due to its ability to tamponade the wound3,10.
- In addition to the risk of hemorrhage, vascular injuries can also result in ischemia and necrosis if blood flow is impeded, or a compartment syndrome in the setting of venous injury and congestion9.
Evaluation:
- All patients should undergo a full trauma evaluation, including initial primary and secondary survey.
- Full exposure of the patient is crucial to evaluate for any other injuries, particularly in the presence of a distracting injury such as an impaled object9.
- Full neurovascular exam to evaluate sensation, strength, and adequate blood flow should be performed in the case of extremity involvement.
- Special, expeditious care should be given to the evaluation for signs of significant vascular injury.
- Hard signs of vascular injury include pulsatile bleeding, absent distal pulses, expanding hematoma, and a bruit or thrill9.
- Soft signs of vascular injury include non-expanding hematoma, history of pulsatile bleeding prior to arrival, and neurologic deficit9.
- Once the patient is stabilized, radiographic evaluation can assist with consultation of the appropriate surgery colleagues as needed3,10.
- X-Rays, CT angiography, or ultrasound are typically the modality of imaging used to evaluate for potential deep injuries, particularly bone or blood vessel injury9.
- Unstable patients should be taken to the OR for emergent wound exploration and repair1.
Treatment:
- Patient who are unstable with significant bleeding require emergent resuscitation with blood products.
- Impalement injuries will typically require removal of foreign body, wound exploration, and wash out in the OR3,4,10,.
- Infection prevention is essential, including appropriate wound debridement and wash out, tetanus prophylaxis, and prophylactic antibiotics, such as cefazolin10.
Follow up:
- Patients should be sent home on a course of prophylactic oral antibiotics.
- Complications due to vascular injury can occur, including the development of pseudoaneurysm and AV fistulalization, and patients should be closely monitored for these6.
Pearls:
- Impaled objects resulting in penetrating injuries can be potentially life or limb threatening depending on the location, depth, and involved neurovascular structures.
- EMS should leave the impaled object in place while in the field and during transport to the ED.
- These patients should be treated as trauma patients, and emergency clinicians must perform a thorough primary and secondary survey to ensure all wounds and injuries are identified.
- The majority of impaled objects will require removal in the OR, and all unstable patients due to impaled objects should be expeditiously taken to the OR. Stable patients can first undergo further imaging and evaluation to identify the extent of injury3.





