
Author: Jackie Nguyen, MD (EM Resident Physician, UTSW – Dallas, TX); Joshua Kern, MD (Assistant Professor of EM/Attending Physician, UTSW – Dallas, TX) // Reviewed by: Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY) and Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 55-year-old male with a history of HTN and DM presents to the ED for a rash of 2-day duration. He reported mild URI symptoms for 4 days preceding the rash with myalgias and subjective fevers for which he has been taking naproxen. He notes the rash began as small painless, erythematous papules but has progressed to larger, tender bullae. The rash began on his trunk and has spread to his face and bilateral upper extremities. Vital signs include T 101.2F, BP 110/67, HR 109, RR 18, SpO2 of 99% on room air. On physical exam, a rash appears as shown below affecting approximately 20% of total body surface area (TBSA), and with gentle rubbing, skin sloughing is noted.

What is the diagnosis and the approach to management?
Answer: Steven-Johnson Syndrome (SJS)/Toxic Epidermal Necrolysis (TEN)
Definition
- Potentially fatal cutaneous reaction characterized by epidermal blistering and necrosis leading to skin sloughing over extensive areas of the body, typically affecting mucocutaneous sites.1, 2
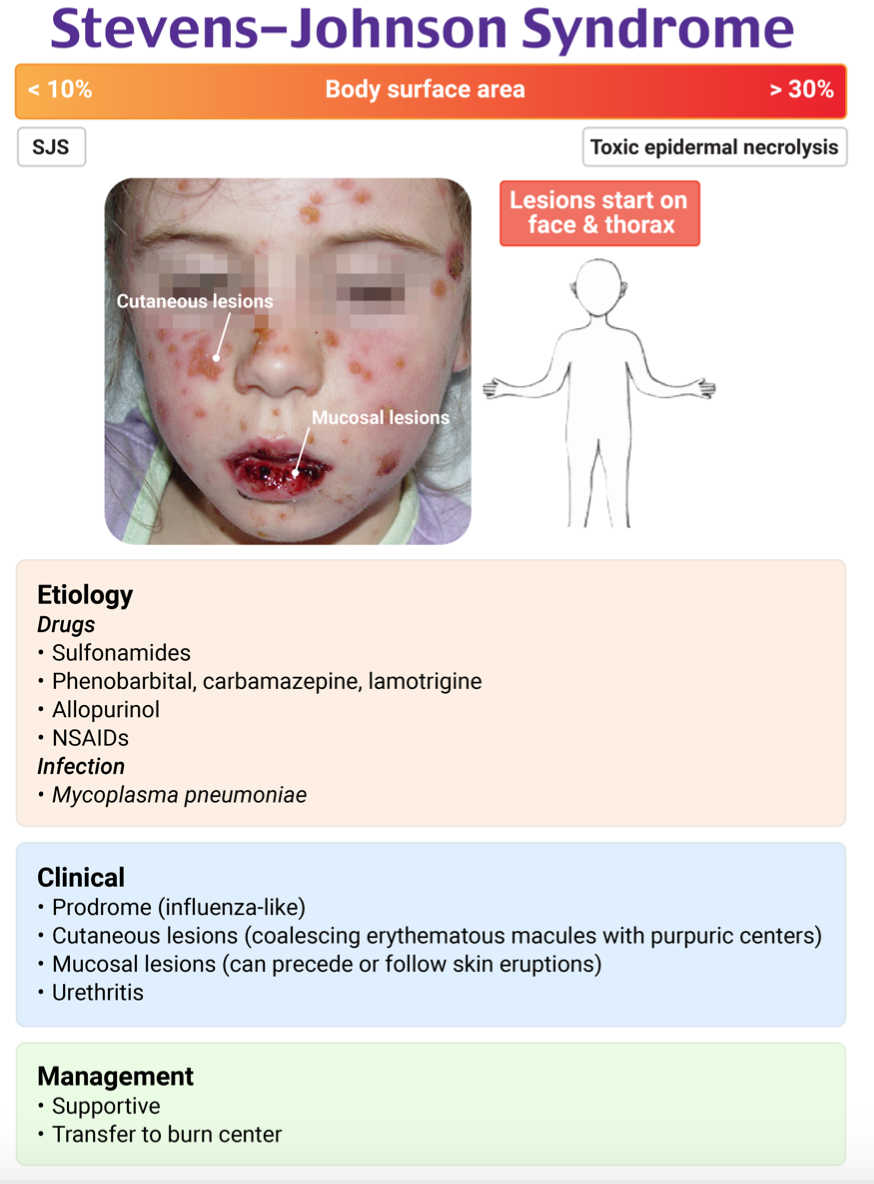
- SJS and TEN occur on a spectrum of the same disease and are based on the extent of total body surface area (TBSA) affected:
- SJS: affecting <10%
- SJS + TEN overlap: affecting 10% to 30%
- TEN: affecting >30%
Epidemiology
- Within the U.S., the incidence of SJS/TEN is estimated to be 1.58 to 2.26 cases per million people.3
- Although the incidence is reported to be low, SJS/TEN carries a high mortality rate of about 4.8%-24% for SJS and 14.8%-49% for TEN.4-6
- Affects individuals of any age, but there is a higher incidence in women with a female to male ratio of 2:1.
- 100-fold risk increase in individuals with HIV; ≥2-fold risk increase in an individual with active malignancy especially hematological ones; increase risk noted in those with systemic lupus erythematosus.3
Pathophysiology
- Not yet fully elucidated, however, thought to be multifaceted.7-9
- Believed to be T-cell mediated with activation of natural killer cells and cytotoxic T lymphocytes that induce widespread apoptosis keratinocytes and mucosal cells by release of death mediators (TNF-α, granzyme, granulysin, Fas-Fas ligands, perforins, etc.).
- Appears to be impacted by genetic factors.
- Increased risk with specific HLA types and polymorphisms of CYP2C19
- Results in partial to full-thickness necrosis of the epidermis.
- Most common trigger is medication.8, 9
- Typically within the first three weeks of initiating treatment and with systemic drugs that have long half-lives.
- Radiation therapy, rapid medication introduction, and high doses of medications increase the risk.
- Over 200 medications implicated with SJS/TEN onset – most common include:

- Infections are the next most common trigger.8-10
- More often in children.
- Mycoplasma, HSV, EBV, CMV, coxsackievirus, and COVID-19 are implicated.
- Vaccination and graft-versus-host disease are implicated in a small number of cases.
- In up to 15-30% of cases, no trigger is identified.
Clinical Presentation
- Can have preceding prodromal symptoms one to three days prior to rash onset.1-3, 8, 11
- Influenza-like symptoms – fever (>38˚C or >100.4˚F), malaise, cough, myalgias, headaches, eye pain, and sore throat.
- Fever can persist throughout the entire course.
- Rash typically manifests first centrally on the face and/or trunk and then will extend to extremities in a symmetrical pattern; soles and palms may be involved although less commonly.
- Initially diffusely purpuric and/or erythematous macular rash can appear with a targetoid appearance and often with ill-defined borders.
- Rash will evolve to coalesce into larger erythematous areas with large flaccid bullae.
- Bullae will begin to slough for ~1-3 days leaving denuded, weeping skin with positive Nikolsky sign noted on examination.
- Skin can be exquisitely tender to palpation, some out of proportion.
- Nails and eyebrows can be lost as well.
- ~90% of cases will have mucocutaneous involvement, most often affecting the oral, genital, and/or ocular sites.
- Most commonly affects oral mucosa leading to mucositis and stomatitis.
- Ocular involvement most commonly results in conjunctival hyperemia, significant conjunctivitis with purulent discharge, and pain; in more severe cases, it can result in anterior uveitis, panophthalmitis, corneal erosions, and blindness from corneal inflammation.
- Genital lesions can result in urethritis and genital erosions with long-term sequelae such as urinary retention and labial/vaginal adhesions.
- Overall, the acute course takes ~8-12 days before re-epithelialization will begin which generally lasts 2-4 weeks.
Extra-mucocutaneous manifestations
- Can have sloughing of bronchial epithelium leading to cough, pneumonia, hypoxemia, and dyspnea.1-3
- Can have sloughing of the GI epithelium leading to dysphagia and odynophagia from esophageal ulcers and diarrhea, melena, intussusception, and bowel ulceration/perforation from small bowel and colon involvement.
Complications
- With the extensive loss of epidermis, the risk of acute complications of impaired barrier function include:8, 9, 11
- Massive fluid and protein loss resulting in dehydration, malnutrition, electrolyte derangements, and potentially shock in severe cases.
- Extensive epidermal loss resulting in hypothermia.
- Long-term epidermal complications include dystrophic nails, skin hyper-/hypopigmentation, pterygium, and anonychia.
- Secondary infection of denuded skin leading to bacteremia, hypercatabolic state, and sepsis.
- Sepsis is the leading cause of death with Pseudomonas aeruginosa and MRSA being the commonly isolated pathogens. Candida, Acinetobacter, and Stenotrophomonas are less commonly isolated.
- Multi-organ injury leading to liver failure, acute tubular necrosis, and renal failure.
- Genital involvement can result in urethral strictures, vaginal stenosis, adhesions, and atrophic vaginitis.
Diagnosis
- Diagnosis is primarily clinical, based on history, through physical examination including of the oral mucosa and genitals, timeline, presence of a known trigger, the appearance of the rash, and potential prodrome.2, 7, 8
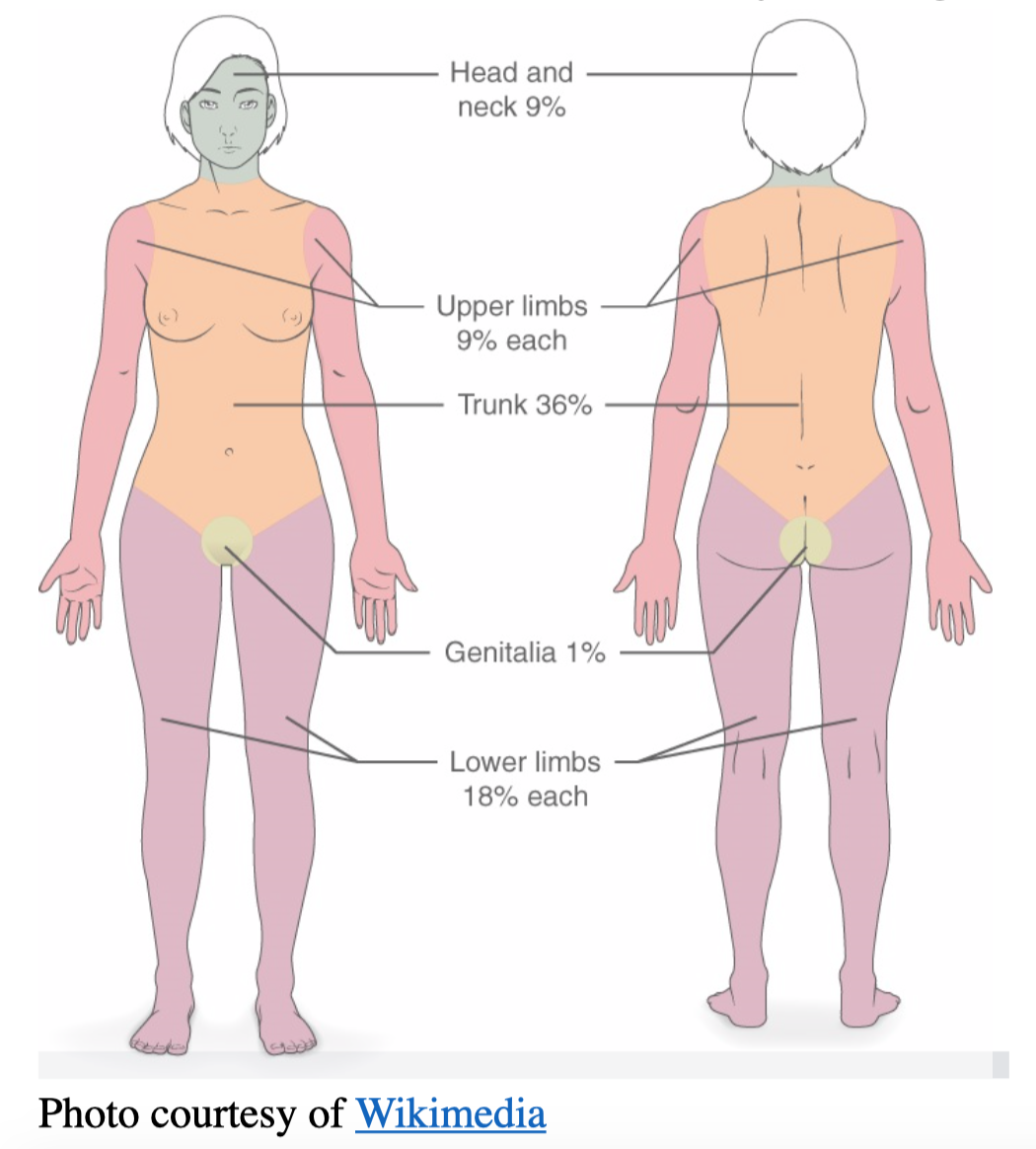
- Calculate the extent of only blistering/denuded areas similar to burns TBSA%.
- Confirmation of the diagnosis is via skin biopsy performed by dermatology to exclude potential mimics like DRESS syndrome, erythema multiforme, toxic shock syndrome, etc.
- Labs can be obtained like CBC to evaluate for infection, CMP to evaluate electrolyte levels, renal function, and hepatic function, and blood cultures if indicated.
- Can be nonspecific and can demonstrate neutropenia, atypical lymphocytosis, anemia, lymphopenia, eosinophilia, electrolyte derangement, reduced GFR, transaminitis.
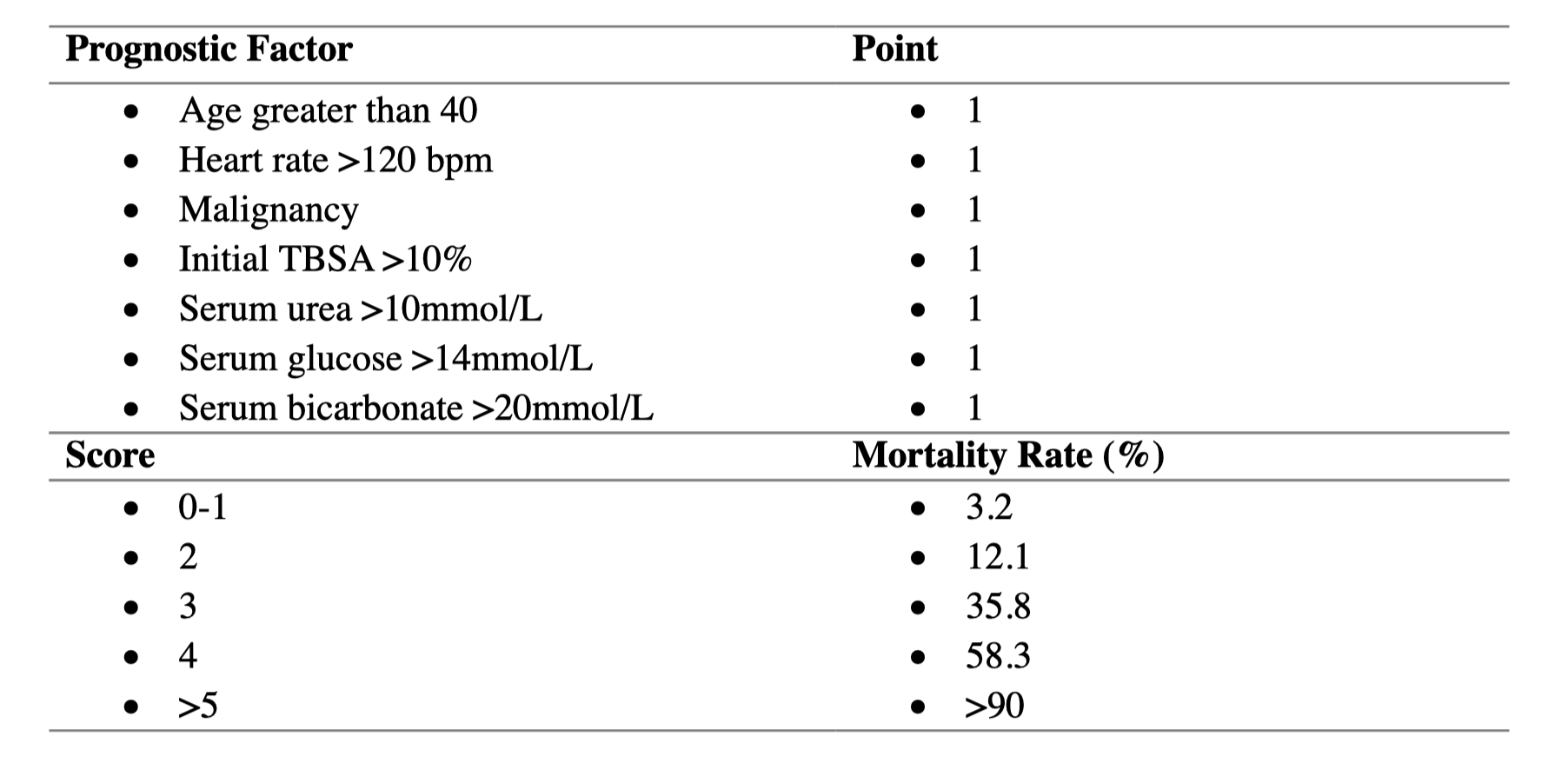
- Severity-of-Illness Score for Toxic Epidermal Necrolysis (SCORTEN)
- Validated and highly accurate for predicting in-hospital mortality for patients with TEN.12
- Should be calculated on Day 1 and Day 3.
Treatment
- Remove known or suspected offending agent.8, 9
- Earlier removal of the offending agent is associated with decreased mortality (OR, 0.69 per day); offending agents with long half-lives are associated with increased mortality risk (OR 4.9).13
- Immediate transfer to burn service or centers, if available, as delays demonstrate higher mortality.14, 15
- Non-adhesive silver-releasing dressings are first line although no proven benefit when compared to other local dermatological therapies.
- Air-fluidized beds, which contain ceramic microspheres that are set into motion using warm air to simulate movement, demonstrate faster re-epithelialization rates and lower complications rates including infections.
- Debridement is controversial with some studies demonstrating improved outcomes and others noting further disruption of the epidermis/dermis with worsening scarring and pigmentation complications.5, 16
- Hydrotherapy with whirlpool may be beneficial.16
- Wounds often will be dressed with biological membranes.
- UK guidelines recommend debridement for >30% TBSA with clinical deterioration, epidermal detachment progression, delayed healing, or wound infections.17
- Supportive care8, 9, 16-18
- High caloric enteral feeding, if possible, rather than parenteral nutrition which has been demonstrated to have higher fatality rates.
- Topical antibiotics and/or occlusive ointments to reduce the risk of secondary infection and provide barrier function.
- Isolation at room temperature with a temperature of 82.4 to 89.6°F (28 to 32°C) and sterile handling are recommended to prevent hypothermia and infection.
- Fluid replacement is essential with the first 24 hours requiring 2 mL/kg/TBSA (%) affected then titrating to maintain a urine output of 0.5 to 1 mL/kg/hour.
- Empiric antibiotic therapy is NOT recommended with some evidence demonstrating it reduces survival.
- Pain control is key as condition and wound care can be extremely agonizing.
- Obtain an ophthalmology consult for ocular involvement.
- Adjunct therapies
- Glucocorticoid effectiveness is controversial.
- Literature suggests steroids increase bacterial infection rates and slow reepithelization, but when initiated early may decrease ocular involvement.14, 19
- Immunoglobulins (IVIG) currently have no clear proven benefit.20
- Cyclosporine demonstrates faster healing times and lower mortality rates although studies have been small, open-labeled, and non-blinded.21
- Glucocorticoid effectiveness is controversial.
- Monitor closely for worsening rash, developing infection/sepsis, or extra-cutaneous developments.
Prognosis
- Recurrence is rare in adults but has been documented with drug re-exposure.22, 23
- Higher rates of recurrence in children indicate vulnerability from genetic predisposition and other factors.24
Pearls
- Consider SJS/TEN when a patient is presenting with blistering rash and fever in the setting of new medication usage or recent viral illness.
- The rash will often have mucous membrane involvement and there can be extra-cutaneous manifestations.
- Medications to support suspicion include the following: NSAIDs, anticonvulsants, sulfa-derived, ß-lactams, antigout, contrast agents, and antiretrovirals.
- Cease medications suspected to be causative immediately and admit to a burn center if possible.

A 40-year-old man presents to the ED reporting fever, myalgias, and a diffuse rash. He recently began taking carbamazepine for trigeminal neuralgia. His vital signs are T 99.9°F (37.7°C), HR 108 bpm, BP 135/85 mm Hg, RR 14/min, and SpO2 100% on room air. On examination, he has a rash that covers approximately 10% of his body surface area and mucosal blistering. Which of the following findings most suggests a diagnosis of Stevens-Johnson syndrome?
A) Eosinophilia
B) Exfoliative bullae
C) Nikolsky sign
D) Target lesions
Answer: D
Stevens-Johnson syndrome (SJS) is a severe immune complex-mediated, exfoliative hypersensitivity dermatitis that lies in the spectrum from erythema multiforme major to toxic epidermal necrolysis (TEN). It typically involves < 10% of the total body surface area, whereas toxic epidermal necrolysis usually involves > 30%. The characteristic target lesions of erythema multiforme are present, as well as mucosal involvement, which may help differentiate Stevens-Johnson syndrome from other widespread dermatoses. It is potentially life-threatening and may lead to multiorgan damage, and mortality and morbidity correlate with the degree of epidermal detachment. Ophthalmologic involvement is present in approximately 70% of cases. Precipitants include drugs (e.g., sulfonamides, anticonvulsants), malignancies, and infections (e.g., herpes simplex virus, Mycoplasma). Patients may present with other systemic symptoms such as fever, malaise, myalgias, and arthralgias. Patients may have diffuse burning or pruritus before the skin lesions appear. Management includes identification and removal or discontinuation of the offending agent, supportive care, hydration, wound management, and prevention of infection. Transfer to a dedicated burn center may be indicated for expert wound care. Ophthalmologic consultation is recommended for ocular involvement. Systemic corticosteroids may provide temporary symptomatic relief but do not affect the outcome or duration of the illness and may make patients more susceptible to infection.
Eosinophilia (A) is seen in drug rash with eosinophilia and systemic symptoms (DRESS syndrome), a diffuse skin condition that typically causes a coalescing, nonblanching rash often mistaken as Stevens-Johnson syndrome (SJS) or sometimes measles. Eosinophilia does not suggest SJS. Exfoliative bullae (B) and Nikolsky sign (C) are more suggestive of toxic epidermal necrolysis than SJS. SJS is not a bullous dermopathy. Nikolsky sign is seen when the epidermis separates from the dermis with lateral rubbing pressure to the skin. Although a positive Nikolsky sign can be seen in SJS, it is a nonspecific finding and can be seen in other conditions.
Further FOAMed
- http://www.emdocs.net/stevens-johnson-syndrome-and-toxic-epidermal-necrolysis-mimics-differential-diagnosis-and-initial-management/
- http://www.emdocs.net/emdocs-net-podcast-episode-8-sjs-ten-mimics-rapid-hand-exam-penile-injuries/
- https://litfl.com/stevens-johnson-syndrome-and-toxic-epidermal-necrolysis/
- https://coreem.net/podcast/episode-162-0-stevens-johnson-syndrome-toxic-epidermal-necrolysis/
References
- Cardon ZE, Kaide CG, Bischof JJ. Stevens Johnson Syndrome – “Steven Who? And Why I Should Care About His Johnson?”. In: Kaide CG, San Miguel CE, eds. Case Studies in Emergency Medicine: LEARNing Rounds: Learn, Evaluate, Adopt, Right Now. Springer International Publishing; 2020:547-558.
- Hasegawa A, Abe R. Recent advances in managing and understanding Stevens-Johnson syndrome and toxic epidermal necrolysis. F1000Res. 2020;9doi:10.12688/f1000research.24748.1
- Oakley; AM, Krishnamurthy K. Stevens Johnson Syndrome. National Institute of Health. Accessed September 16, 2022. https://www.ncbi.nlm.nih.gov/books/NBK459323/
- Hsu DY, Brieva J, Silverberg NB, Silverberg JI. Morbidity and Mortality of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in United States Adults. J Invest Dermatol. Jul 2016;136(7):1387-1397. doi:10.1016/j.jid.2016.03.023
- Nizamoglu M, Ward JA, Frew Q, et al. Improving mortality outcomes of Stevens Johnson syndrome/toxic epidermal necrolysis: A regional burns centre experience. Burns. May 2018;44(3):603-611. doi:10.1016/j.burns.2017.09.015
- Harr T, French LE. Stevens-Johnson syndrome and toxic epidermal necrolysis. Chem Immunol Allergy. 2012;97:149-66. doi:10.1159/000335627
- Panpruk R, Puangsricharern V, Klaewsongkram J, et al. Clinical parameters and biological markers associated with acute severe ocular complications in Stevens-Johnson syndrome and toxic epidermal necrolysis. Scientific Reports. 2021/10/12 2021;11(1):20275. doi:10.1038/s41598-021-99370-1
- Cheng L. Current Pharmacogenetic Perspective on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Front Pharmacol. 2021;12:588063. doi:10.3389/fphar.2021.588063
- Schneider JA, Cohen PR. Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Concise Review with a Comprehensive Summary of Therapeutic Interventions Emphasizing Supportive Measures. Adv Ther. Jun 2017;34(6):1235-1244. doi:10.1007/s12325-017-0530-y
- Aulakh S, Arora R, Sarangal R, Chopra D. Increased Predisposition of SJS TEN in COVID-19 Patients, Presenting as Post COVID Complication: Report of Two Cases. Indian Dermatology Online Journal. 2022;13(2):237-239. doi:10.4103/idoj.idoj_510_21
- Frantz RHSAAMKSJS, Toxic Epidermal Necrolysis ARoD, Management. Medicina. 2021;57(9). doi:10.3390/medicina57090895
- Koh HK, Fook-Chong S, Lee HY. Assessment and Comparison of Performance of ABCD-10 and SCORTEN in Prognostication of Epidermal Necrolysis. JAMA Dermatology. 2020;156(12):1294-1299. doi:10.1001/jamadermatol.2020.3654
- Garcia-Doval I, LeCleach L, Bocquet H, Otero XL, Roujeau JC. Toxic epidermal necrolysis and Stevens-Johnson syndrome: does early withdrawal of causative drugs decrease the risk of death? Arch Dermatol. Mar 2000;136(3):323-7. doi:10.1001/archderm.136.3.323
- McCullough M, Burg M, Lin E, Peng D, Garner W. Steven Johnson Syndrome and Toxic Epidermal Necrolysis in a burn unit: A 15-year experience. Burns. 2017/02/01/ 2017;43(1):200-205. doi:https://doi.org/10.1016/j.burns.2016.07.026
- Palmieri TL, Greenhalgh DG, Saffle JR, et al. A multicenter review of toxic epidermal necrolysis treated in U.S. burn centers at the end of the twentieth century. J Burn Care Rehabil. Mar-Apr 2002;23(2):87-96. doi:10.1097/00004630-200203000-00004
- Papp A, Sikora S, Evans M, et al. Treatment of toxic epidermal necrolysis by a multidisciplinary team. A review of literature and treatment results. Burns. Jun 2018;44(4):807-815. doi:10.1016/j.burns.2017.10.022
- Creamer D, Walsh SA, Dziewulski P, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. J Plast Reconstr Aesthet Surg. Jun 2016;69(6):e119-e153. doi:10.1016/j.bjps.2016.01.034
- Koh HK, Chai ZT, Tay HW, et al. Risk factors and diagnostic markers of bacteremia in Stevens-Johnson syndrome and toxic epidermal necrolysis: A cohort study of 176 patients. J Am Acad Dermatol. Sep 2019;81(3):686-693. doi:10.1016/j.jaad.2019.05.096
- Tocco-Tussardi I, Huss F, Presman B. Microbiological findings and antibacterial therapy in Stevens–Johnson syndrome/toxic epidermal necrolysis patients from a Swedish Burn Center. Journal of Cutaneous Pathology. 2017;44(5):420-432. doi:https://doi.org/10.1111/cup.12894
- Roujeau JC, Bastuji-Garin S. Systematic review of treatments for Stevens-Johnson syndrome and toxic epidermal necrolysis using the SCORTEN score as a tool for evaluating mortality. Ther Adv Drug Saf. Jun 2011;2(3):87-94. doi:10.1177/2042098611404094
- Ng QX, De Deyn M, Venkatanarayanan N, Ho CYX, Yeo WS. A meta-analysis of cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis. J Inflamm Res. 2018;11:135-142. doi:10.2147/jir.S160964
- Lee HY, Tharmotharampillai T, Pang SM. Recurrence of Stevens-Johnson syndrome and toxic epidermal necrolysis in adults. Int J Dermatol. Apr 2017;56(4):e78-e79. doi:10.1111/ijd.13125
- Finkelstein Y, Macdonald EM, Li P, Hutson JR, Juurlink DN. Recurrence and Mortality Following Severe Cutaneous Adverse Reactions. JAMA. 2014;311(21):2231-2232. doi:10.1001/jama.2014.839
- Finkelstein Y, Soon GS, Acuna P, et al. Recurrence and outcomes of Stevens-Johnson syndrome and toxic epidermal necrolysis in children. Pediatrics. Oct 2011;128(4):723-8. doi:10.1542/peds.2010-3322





1 thought on “EM@3AM: Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis”
Pingback: Quiz 180, February 17th, 2022 – The FOAMed Quiz