Authors: Katie Lupez, MD (@KatieLupez, EM Resident Physician, Carolinas Medical Center) and Michael Runyon, MD, MPH (Professor of EM, Carolinas Medical Center) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW/Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC)
Case
A 21-year-old female presents with fever one week after returning from Uganda, where she participated in a college service trip to an orphanage. She has had no symptoms other than a fever for the past few days. Vitals: HR 100, BP 120/80, T 102° F, RR 15. The patient is well appearing, and the physical examination reveals no rash, clear lungs, a soft and non-distended abdomen with mild splenomegaly, and no focal neurological findings.
Perspective
- Approximately three percent of international travelers contract an illness requiring medical attention with isolated fever being most common presentation.1
- These patients are at a high risk of misdiagnosis and delayed treatment due to the relative rarity of tropical diseases in high-income countries.
- It is imperative that the EM physician undertakes a systematic approach to evaluating these patients.
- We must be able to rapidly and accurately identify potentially communicable diseases, immediately initiate any indicated treatment and isolation measures, and determine the optimal patient disposition.
Initial Assessment
- Our initial assessment should include reviewing the patient’s vital signs and overall appearance.
- Promptly recognize life threats requiring immediate intervention, such as airway, breathing, or circulatory compromise, and resuscitate appropriately.
- Keep a broad differential that includes tropical diseases.
- If at all suspicious for a communicable disease, isolate the patient early and use the appropriate level of personal protective equipment to ensure your safety and that of your staff and other patients.
HPI
- Placing the patient’s fever in perspective of an epidemiological link will help guide your differential diagnosis.
- Begin with open-ended questions, eventually narrowing down to identify the patient’s specific chief complaint, duration of complaint, and associated symptoms.
- The travel history should include:
- all destinations visited
- the day-to-day itinerary and duration of travel
- any pre-travel vaccinations or prophylaxis (including specific drugs, doses, and dates of treatment, including any missed or delayed doses)
- travel exposures: arthropod, bird, exotic pet, and livestock exposures, types of foods consumed, piercings/tattoos obtained, IV drug use, sexual encounters or any healthcare exposure or treatment abroad
- A thorough evaluation of the patient’s past medical history is important to help further delineate their potential susceptibility to certain diseases.
Physical Exam
- A detailed physical exam will help solidify your diagnosis.
- Vital signs: note any relative bradycardia (heart rate lower than would otherwise be expected given the degree of fever) and remember recent antipyretic use can mask fever.
- Skin: ensure that the patient is fully unclothed and examine for any evidence of bites, jaundice, pallor or rash with specific rashes to consider including petechiae and rose-colored spots.
- HEENT: look for conjunctivitis, lymphadenopathy, and nuchal rigidity.
- Cardiopulmonary: identify any focal crackles, diffuse wheezing, or murmurs.
- Abdominal exam: assess for tenderness in all quadrants, identify any hepatomegaly or splenomegaly, and assess for Murphy’s sign.
- Neuro: identify any altered mental status or focal neurologic findings.
- Special tests: consider performing specialized tests such as the Rumpel-Leede test.
- Rumpel-Leede (tourniquet test): This test assesses for capillary fragility that is classically suggestive of dengue, but can be associated with a wide variety of tropical diseases and has been recently associated with Chikungunya and Zika infections2. The test is performed after initially taking the patient’s blood pressure and then re-inflating the blood pressure cuff midway between the systolic and diastolic pressures, maintaining this pressure for approximately 5 minutes. After removing the cuff, the test is considered positive if you identify >10 petechiae per square inch within approximately 2 minutes of deflating the BP cuff as noted in Figure 1 below.3,4
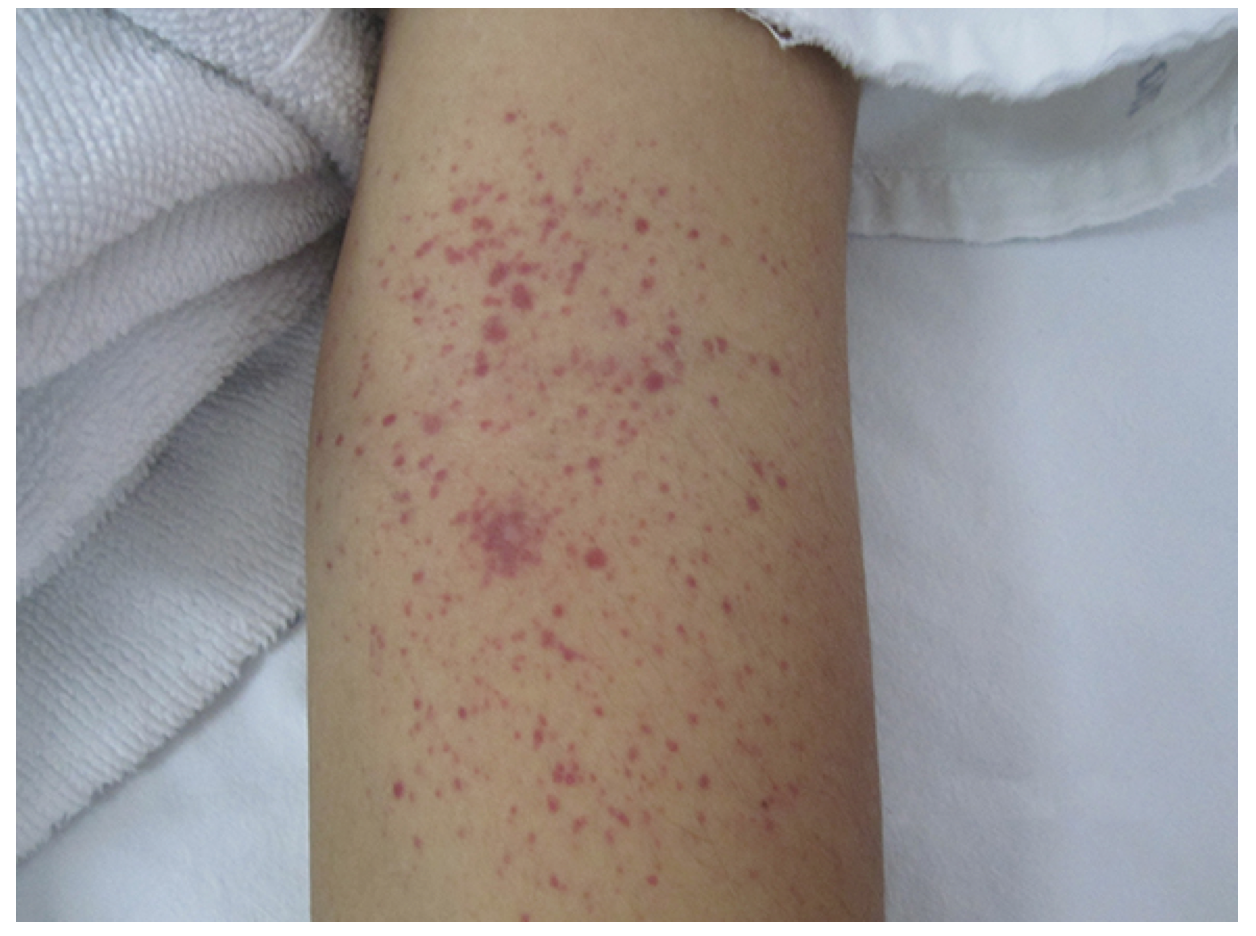
Figure 1.5 Rumpel-Leede Test
Diagnostic Testing
- Use your initial assessment, HPI, and physical exam to help guide your differential diagnosis and inform your diagnostic testing.
- In general, a CBC with diff, urinalysis/urine culture, and CMP will be the minimum work up in a returning traveler with fever.6
- Review your CBC for platelet count and absolute eosinophil count.
- Consider a CXR for patients with respiratory symptoms or abnormal cardiopulmonary examination findings.
- Consider stool examination for patients with diarrhea.
- Send blood cultures if patient’s fever remains undifferentiated or patient’s illness appears systemic.
- Consider rapid antigen detection tests for malaria, if available.
- Thick and thin blood smears should be sent also since in addition to identifying the presence of parasites, they can inform management by quantitating the parasitemia, and identifying the particular species. If the initial blood smear is negative, yet your suspicion remains high or the patient is immunosuppressed, send q12h smears for a total of three negative smears before ruling out malaria.
- Order serological testing (RT-PCR, ELISA, immunoassay) of the specific diseases you are concerned about
- It may not yield results quickly enough to impact ED decision-making, but may be important to assist admitting or outpatient team management.
- Order a UPT in all women of childbearing potential.
Plan
- Initiate isolation and appropriate level of personal protective equipment early.
- Clearly communicate your concerns and the potential threat to the clinical staff treating the patient.
- Resuscitate as needed
- Treat identified diseases
- Initiating early treatment can help prevent morbidity/mortality from rapidly progressing diseases such as falciparum malaria.
- Of note, many of these tropical diseases have no definitive treatment, but are managed by supportive care alone.
- Determine disposition
- Disposition will greatly vary based on patient’s overall appearance, social situation, and treatment needs.
- If you feel the patient is appropriate for outpatient management, ensure good outpatient follow up.
- Use the resources below to identify geographical outbreaks and the clinical manifestations (i.e. during recent Ebola outbreaks in West Africa, most patients presented with fever and GI symptoms and only a minority had hemorrhagic manifestation7).
- CDC Yellow Book8
- GeoSentinel9
- WHO10
- If patient still remains undifferentiated, consider consulting your infectious disease colleagues from the ED.
Working Through Your Differential Diagnosis
Fever and Abdominal Pain
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment | ||
| Giardiasis | Worldwide | 1-3 weeks | Greasy stools, diarrhea | Stool ova and parasites | Metronidazole | ||
| Typhoid Fever | Southern Asia | 7-18 days | Rose colored spots | Blood cultures | Ciprofloxacin | ||
| Cholera | Africa, Southeast Asia, Caribbean | 2-3 days | Rice water stools | Clinical, rectal swab can be sent for lab dx | Aggressive rehydration, can consider doxycycline | ||
| Schistosomiasis (Katayama Fever) | Africa | 4-8 weeks | Hematuria, diarrhea | stool or urine parasites | Praziquantel | ||
| Liver Fluke | Clonorchiasis | Asia | 1 month | RUQ tenderness | CBC with diff, ultrasound, stool exam | Praziquantel or albendazole | |
| Fascioliasis | Africa, Middle East, South America | 6-12 weeks | nitazoxanide/triclabendazole | ||||
| Liver Abscess (Entamoeba) | India, Indonesia, Thailand, Mexico | 7-14 days | RUQ tenderness, watery or bloody diarrhea |
RUQ U/S, stool microscopy, PCR and serologic tests as needed |
Metronidazole ± iodoquinol | ||
| ETEC, norovirus, campylobacter, shigella, salmonella |
Worldwide | variable | diarrhea | if prolonged can consider stool examination and culture | supportive care if prolonged consider tx with ciprofloxacin |
||

Figure 211 Typhoid Fever Rose Colored Spots

Figure 312. Liver Abscess. Case courtesy of Dr Maulik S Patel, Radiopaedia.org, rID: 9335
Fever and Respiratory Symptoms
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment |
| MERS-CoV | Arabian Peninsula | 2-14 days | cough | specimen or serologic PCR | supportive care and isolation |
| Tuberculosis | Worldwide | 1-2 week | cough, hemoptysis, weight loss | CXR, sputum culture (+acid fast bacilli), NAAT | RIPE (rifampin, isoniazid, pyrazinamide, ethambutol) |
| Influenza | Worldwide, China (Avian flu) |
1-3 days | nonproductive cough, malaise, vomiting/diarrhea myalgias |
rapid identification test, RT-PCR, viral culture | early neuraminidase inhibitor isolation if avian flu suspected |
| Q fever | Africa and Middle East | 2-4 weeks | flu like illness, cough | indirect immunofluorescent assay | Doxycycline |
Fever and Jaundice
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment |
| Yellow Fever | Equatorial Belt | 3-6 days | black emesis, relative bradycardia | cbc, cmp, urinalysis, titers | supportive care |
| Hep A | Africa and Asia | 2-6 weeks | malaise, hepatomegaly | hepatitis panel | dose of monovalent hepatitis vaccine or IG |
| Hep B | Worldwide | 60-150 days | Supportive care | ||
| Hep C | Worldwide | 6-9 weeks | boceprevir and telaprevir | ||
| Hep E | Africa and Asia | 2-9 weeks | supportive care |
Fever and Arthralgia
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment |
| Dengue | Latin America, Southeast Asia | 4-8 days | petechiae, retro-orbital pain, epistaxis | RT-PCR, DENV immunoassay, ELISA | supportive care, avoid NSAIDs risk of hemorrhage |
| Zika | Africa, Asia, Latin America | 2 weeks | conjunctivitis, flu like illness | clinical dx, rRT-PCR | supportive care |
| Chikungunya | Africa, Asia, Latin America | 2-4 days | flu like illness, maculopapular rash | clinical dx, CHIKV IgM, viral culture | supportive care |
Fever and Hemorrhage
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment | |
| Viral | Ebola | West Africa | 2-21 days | flu like symptoms | RT-PCR | supportive care and isolation |
| Crimean-Congo | Africa/Eastern Europe | 1-13 days | headache, vomiting, conjunctivitis | ELISA, RT-PCR | supportive care, if severe ribavirin, isolation | |
| Lassa | West Africa | 3-16 days | severe sore throat | ELISA, RT-PCR | supportive care, if severe ribavirin, isolation | |
Fever and AMS
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment | |
| Encephalitis | Japanese | Asia | 5-15 days | nuchal rigidity, seizure | clinical dx, LP to r/o other causes, ELISA, RT-PCR | supportive care |
| West Nile | Africa, Middle East, Europe | |||||
Undifferentiated Fever
| Tropical Differential Diagnosis | Location | Incubation | Signs and Symptoms | Diagnostic Tests | Treatment | |
| Malaria | P. falciparum | Worldwide, predominate species in Africa | 7-30 days | malaise, nausea, vomiting, hepatosplenomegaly, mild jaundice, body aches |
Thick and thin smear, Rapid diagnostic test (antigen detection), PCR |
Atovaquone-proguanil, (can use chloroquine in sensitive regions) |
| P. malaria | South America, Africa, Asia | |||||
| P. knowlesi | Southeast Asia | |||||
| P. Ovale | Sub-Saharan Africa | Atovaquone-proguanil + Primaquine | ||||
| P. Vivax | Worldwide, predominate species outside of Africa | |||||
Case Conclusion
Her UPT is negative. Her CBC reveals a mild anemia with a Hgb of 11 g/dl. The rest of her CBC with differential, CMP, and urinalysis are within normal limits. A rapid malaria test is preformed and comes back positive. You send for a thick and thin smear. Her parasitemia level is approximately 2 percent, and the reader has identified the malaria species as P. falciparum. You reference the CDC yellow book, and based on her geographical area of travel you find this is most likely an area of chloroquine resistance and therefore prescribe atovaquone-proguanil. Based on your above work up you believe she does not meet criteria for severe malaria. After assessing her social situation, you feel she is a candidate for outpatient management of her uncomplicated malaria with close primary care follow-up.
Take Home Message
- Take a thorough history and perform a complete physical examination.
- Keep a broad differential including thinking through various tropical diseases pertinent to the patient’s travel history and examination findings.
- Rapidly identify transmissible diseases, institute appropriate isolation, PPE, treatment, and determine the optimal patient disposition.
References / Further Reading:
- Ryan ET, Wilson ME, Kain KC. Illness after International Travel. N Engl J Med. 2002;347(7):505-516. doi:10.1056/NEJMra020118.
- Kulkarni SA, Strobelt E, Sargsyan Z. Capillary Fragility in Zika Virus Infection. Am J Med. 2017;130(2):e59. doi:10.1016/j.amjmed.2016.10.008.
- Clinical Assessment. Available at: https://www.cdc.gov/dengue/training/cme/ccm/page73112.html.
- Wang K, Lee J. Rumpel–Leede Sign. N Engl J Med. 2014;370(1):e1. doi:10.1056/NEJMicm1305270.
- Dengue virus infection: Clinical manifestations and diagnosis – UpToDate. Available at: https://www.uptodate.com/contents/dengue-virus-infection-clinical-manifestations-and-diagnosis?source=search_result&search=tourniquet test&selectedTitle=1~150.
- VanRooyen MJ, Venugopal R. Chapter 156. World Travelers. In: Tintinalli JE, Stapczynski JS, Ma OJ, et al., eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: The McGraw-Hill Companies; 2011. Available at: accessmedicine.mhmedical.com/content.aspx?aid=6375223.
- Moole H, Chitta S, Victor D, et al. Association of clinical signs and symptoms of Ebola viral disease with case fatality: a systematic review and meta-analysis. J community Hosp Intern Med Perspect. 2015;5(4):28406. doi:10.3402/jchimp.v5.28406.
- 2016 Yellow Book Home | Travelers’ Health | CDC. Available at: https://wwwnc.cdc.gov/travel/page/yellowbook-home-2014.
- The International Society of Travel Medicine. Available at: http://www.istm.org/geosentinel.
- WHO | World Health Organization. WHO. 2017.
- Typhoid, Let’s win the war: Typhoid (Salmonella S Typhi) Fever- Causes, Symptoms, Diagnosis, Types. Available at: http://www.typhoid.co/2015/03/typhoid-symptoms-salmonella-typhi.html.
- Al G et. Radiopaedia Hepatic Abscess.





1 thought on “Fever in the Returning Traveler: Systematic ED Approach”
Pingback: Nerdfallmedizin.de - NERDfall Nr. 19 – Teil 2: Dengue-Fieber