Welcome back to Small Talk. Every first Wednesday of the month we will release high yield PEM content written by PEM talent from around the country. We hope you enjoy these reviews. Comments, questions, accolades or concerns: feel free to reach out to Joe Ravera, MD (pemgemspod@gmail.com).
Author: Joe Ravera MD (@pemuvm1, Director of Pediatric Emergency Medicine, Assistant Professor of Surgery, Division of Emergency Medicine, University of Vermont Medical Center) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
At first, Lyme disease can seem daunting- there are myriad clinical syndromes and patients can even be minimally symptomatic or asymptomatic. In areas with high prevalence of the causative agent, Borrelia Burgdorferi, which is found in deer ticks, providers are typically accustomed to recognizing the symptoms particularly in the warmer months. However, with climate change, a more interconnected world, and long incubation periods- Lyme may be coming to an area near you! As such, providers in all areas should be familiar with some of the more common syndromes, which diagnostic tests are available, and how to appropriately treat and disposition patients from the emergency department. The aim of this review is not to make you Lyme expert but give you key points for diagnostic dilemmas.
We Just Found a Tick on my Kid – Will They Get Lyme?
Many EM doctors in New England have fielded this question from friends and family via text or call. In this case, the first question is not does the tick carry Lyme but how long has the tick been on. It is astronomically rare to transmit Lyme if the tick has been on for less than 36 hours. Although the argument “if they have this tick, they may have another” is commonly cited, current guidelines recommend against prophylaxis for a tick on less than 36 hours as the chance of transmission from that tick is essentially zero.1 If the family does routine tick checks and it was not there yesterday, they are in the clear (for that tick). Interestingly, in most cases of confirmed Lyme there is no recollection of a tick bite.
If the tick was on for more than 36 hours or the time is unknown the next question becomes is there a chance this tick carried Lyme. In most of New England Lyme is hyperendemic and it’s assumed that all ticks carry it, however the CDC website can provide more accurate information in your practice location. Typically, we do not try to speciate the tick as there can be very subtle differences- to paraphrase Dr. McCoy from Star Trek “I’m a doctor not an entomologist”.
If after these questions we have a confirmed tick on for longer than 36 hours in an endemic area prophylaxis is recommended doxycycline 4.4 mg/kg PO X 1, is safe effective at reducing the chance of transmission.1
That’s Funny My Kid’s Knee Is Swollen
Acute monoarticular arthritis in children has a broad differential and includes Lyme, an incident presentation of an inflammatory arthritis or the most concerning, acute pyogenic septic arthritis from a bacterial infection (usually staph or strep). While there are some clinical differences in presentation, particularly from this author’s experience, Lyme arthritis can produce impressive effusions, but the children typically do not appear ill, are afebrile, and able to bear limited weight. However, given the clinical overlap and concern for missing a more serious diagnosis of septic arthritis an arthrocentesis is often considered. Unfortunately sticking a needle in the joint to help evaluate for septic arthritis is not as straight forward as one would imagine. The procedure (especially in a knee) is typically not difficult, but the interpretation of the result can be. Several studies have attempted to codify risk but unfortunately there is no reliable synovial cell count that can distinguish acute septic arthritis from Lyme arthritis.2 If the gram stain is positive, that is, of course, helpful, but often times the gram stain will be negative even in septic arthritis.
Given the difficulty with interpretation of synovial cell count is there any other way to risk stratify these children? A recent publication from the Lyme research network looked at this questions and did come up with an algorithm to identify kids at low risk for a bacterial musculoskeletal infection (MSKI). They found that children with:
– Procalcitonin (PCT) level of less than or equal to 0.50 ng/mL
– C-reactive protein (CRP) level of less than or equal to 0.6 mg/dL
– A positive Lyme C6 EIA
were classified as low risk with no cases of missed MSKI. It should be noted this study was done in Lyme endemic areas with 61 percent (n=451) of the patients enrolled stratifying as low risk.3 Based on this study these children can likely be managed without an arthrocentesis and safely managed with Doxycycline 4.4 mg/kg/day orally divided twice daily (maximum 100 mg per dose) for 14 to 21 days.1
The Rarer Stuff: Neurologic Lyme and Lyme Carditis
Neurologic Lyme is a broad clinical entity and runs the gamut from meningitis, peripheral neuropathy and in rare cases encephalitis. Given the wide range of clinical presentations and overlap with other conditions, I think the most salient advice is to remember that Lyme is a possible causative agent and keep it in mind if there is an epidemiologic risk factor and send the appropriate serologies. With-in this spectrum the clinical entity that often provides the most difficulty is an isolated facial nerve (Bells) palsy. Bells palsy is less common in younger children and Lyme should strongly be considered in endemic areas. In certain areas up to a quarter of all Bell’s palsy cases have positive Lyme serologies4 and as suc diagnostics Lyme serologies should be sent in endemic areas.1 The question of a lumbar puncture often comes up and it should be noted that many children with Lyme associated Bells palsy will have evidence of meningitis on CSF analysis but the presences of this pleocytosis does not change management. In this authors opinion, well appearing children with Lyme associated bells palsy can have the lumbar puncture omitted and safely treated with doxycycline 4.4 mg/kg/day orally divided twice daily (maximum 100 mg per dose) for 14 to 21 days.1
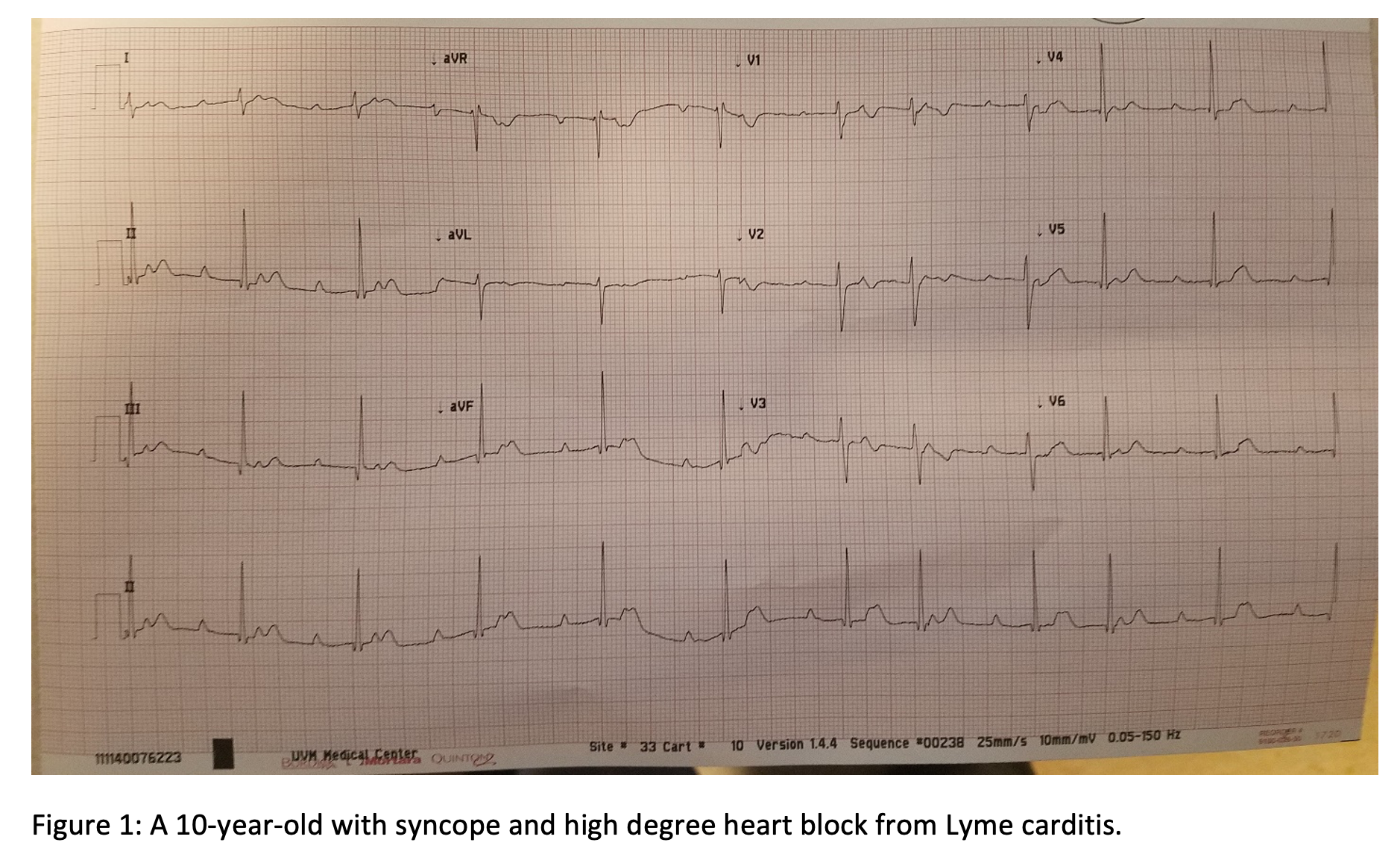
Lyme carditis is a rare but possibly underrecognized clinical entity. To give an idea of prevalence, one review from Maine analyzed 10 admitted cases over a decade at a major referral center.5 Lyme carditis in children is often diagnosed in reverse. Meaning the child comes in with presyncope or syncope and an EKG demonstrates a high order or complete heart block. Any child with this EKG findings (Figure 1) and a possible exposure should have Lyme serologies sent and consideration of empiric treatment.
While this is easy to pick up and treat the more difficulty question is do we screen for Lyme carditis with an EKG in patients with suspected or confirmed Lyme. IDSA has a weak recommendation at this time that only symptomatic children be screened, however the symptoms are broad and include dyspnea, edema, palpitations, lightheadedness, chest pain, and syncope.1 At the very least children should have these questions asked and an EKG should be considered. If there is evidence of first degree heart block but the PR is less than 300ms those patients can be managed with oral antibiotics and follow up to ensure resolution. Children are at higher risk for cardiac complication if the PR is greater that 300ms or there is higher degree heart block those children should be admitted with telemetry and treated with intravenous antibiotics (Ceftriaxone 50mg/kg).1
Summary and Recommendations
- Chemoprophylaxis after a tick bite is only recommended for endemic areas and a tick on for greater than 36 hours.
- In endemic areas, children at low risk for MSKI may be treated empirically for Lyme without an arthrocentesis.
- In endemic areas, well children with a facial nerve palsy and Lyme may be treated empirically without a lumbar puncture.
- Children with Lyme and symptoms of carditis should be screened with an EKG and the decision for treatment and hospitalization is based on the length of the PR or the presence of higher order block.
References
- Lantos PM, Rumbaugh J, Bockenstedt LK, et al. Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease. Clin Infect Dis. 2021 Jan 23;72(1):e1-e48.
- Deanehan JK, Nigrovic PA, Milewski MD, et al. Synovial fluid findings in children with knee monoarthritis in lyme disease endemic areas. Pediatr Emerg Care. 2014 Jan;30(1):16-9.
- Lyons TW, Kharbanda AB, Thompson AD et al.; Pedi Lyme Net. A Clinical Prediction Rule for Bacterial Musculoskeletal Infections in Children with Monoarthritis in Lyme Endemic Regions. Ann Emerg Med. 2022 Sep;80(3):225-234.
- Pacheco A, Rutler O, Valenzuela I, et al. Positive Tests for Lyme Disease and Emergency Department Visits for Bell’s Palsy Patients. J Emerg Med. 2020 Dec;59(6):820-827. doi: 10.1016/j.jemermed.2020.07.038. Epub 2020 Sep 22. PMID: 32978030.
- Shen RV, McCarthy CA, Smith RP. Lyme Carditis in Hospitalized Children and Adults, a Case Series. Open Forum Infect Dis. 2021 Mar 23;8(7)L:ofab140.




