
Original podcast posted on PEM Currents – Hosted by Brad Sobolewski (@PEMTweets) and co-authored by Dennis Ren (@DennisRenMD)
This podcast series by PEM Currents is a co-production with the Emergency Medical Services for Children Innovation and Improvement Center (EMSC IIC), whose mission is to minimize morbidity and mortality of acutely ill and injured children across the emergency continuum.
The emDOCs.net team is very happy to collaborate with PEM Currents and EMSC IIC to further disseminate this 5-part podcast series focusing on agitation in children and adolescents.
![]()
Podcast: Play in new window | Download (Duration: 19:53 — 27.3MB)
Subscribe: Apple Podcasts | Google Podcasts | RSS
Pharmacologic Management
In episode 1 of this series, we discussed differentiating organic vs psychiatric causes of agitation in children. In episode 2, we discussed non-pharmacologic management of agitation including physical restraints. Now it is time to review pharmacologic management.
When we think of managing agitated patients we think of medicines – but that shouldn’t be our first option. However, medications can be adjuncts to non-pharmacologic means to help keep agitated children safe from harm. This podcast episode is all about age-appropriate pharmacologic management strategies for agitated children.
After listening to this episode you will be able to:
- Discuss the medications commonly used to treat acute agitation in children and adolescents
- Discuss the different routes of administration to safely administer these medicines
General strategies
There is no perfect medication option for every scenario, and the true efficacy of the various options is unknown in children. You should always follow your local practice guidelines and recommendations as well as adhere to approved medications in your facility. If a patient has a PRN on their med list do that!
Route of administration
If the patient is cooperative, offer oral medications first. This can give the patient a sense of some control. I liken an anxiolytic or agitation med to taking medicine for pain – “we are not drugging you” we want to help you feel better. Holding down and giving a “shot” is traumatic. Many drugs have oral forms – some rapid dissolving (olanzapine) that can be quite effective.
Intramuscular (IM) is an option for the combative patient or patient who refuses to take oral medications, and who cannot be calmed using non-pharmacological means. It is incredibly important to assure that the patient and staff follow local practices to stay safe and avoid unanticipated injuries. You should be familiar with dosing, onset, and what monitoring is needed following an IM shot – because absorption is not instantaneous.
Let’s move on to a discussion of individual classes of drugs.
Antipsychotics
First generation/typical
Developed in the 1950s, including serotonin-dopamine antagonists and multi-acting receptor-targeted antipsychotics. These phenothiazine derivatives have varying degrees of dopamine, histamine, and cholinergic receptor antagonism – which accounts for their side effects and antiemetic properties.
- Haloperidol (Haldol) – 0.5-5 mg PO; 0.05-0.15 mg/kg IM (up to 5 mg/dose)

- Chlorpromazine (Thorazine) – 0.55 mg/kg/dose (PO/IM)
- Droperidol – 0.03-0.07 mg/kg/dose (IM/IV)
- Has a FDA Black Box warning in 2001 citing concerns of QT prolongation and torsades de pointes (TdP). Some dispute this evidence – 9 cases of TdP over a 30 year period, all in doses higher than 5mg,
- Grownup ED docs love them some droperidol
- A systematic review of the effectiveness and safety of droperidol for pediatric agitation in acute care settings –
- This study had Six articles that met inclusion criteria: two in the prehospital setting, one in the emergency department, and three in the inpatient hospital setting. The articles included a prospective observational study, three retrospective observational studies, and two case reports.
- Overall time to sedation was less than 15 minutes
- Less than 1 in 5 needed a second dose
- Adverse events included dystonic reactions and transient hypotension
- One patient had proloned QTc and another transient respiratory depression – both had medical comorbidities
- Before you go using droperidol know that these studies also were assessed to have a high risk of bias
- Further data is needed – but I know that not mentioning droperidol would be a conspicuous omission even if the data is limited in children
Second generation/atypical
Developed in the 1980s are dopamine partial agonists. These include the following:
- Aripiprazole (Abilify), Asenapine (Saphris), Olanzapine (Zyprexa), Quetiapine (Seroquel), Risperidone (Risperdal), Ziprasidone (Geodon)
Most common side effects include akathisia, sedation, headache nausea, vomiting, weight gain, and changes ot liver function, and arrely cardiac conduction abnormalities (long QTc)
Some of these drugs are useful in acute agitation:
![]()
The ODT form of zyprexa is generally safe and effective
![]()
![]()
Benzodiazepines
Sedation via GABA enhancement
- Lorazepam – 0.05-0.1 mg/kg/dose (PO/IM/IV)
- Midazolam – 0.25-0.5 mg/kg/dose PO; 0.2-0.3 mg/kg IN; 0.1-0.15 mg/kg/dose IM
Generally safe and effective in children – some experts recommend these as first line treatment options AVOID in delirium, autism spectrum disorder, history of paradoxical reaction, or AVOID within 1 hour IM olanzapine
Side effects: respiratory depression if administered with an antipsychotic, disinhibition, delirium
Antihistamines
Sedation via histamine effect on cortical neurons
- Diphenhydramine – 1 mg/kg/dose (PO/IM)
- Hydroxyzine (atarax) similar dosing to Diphenhydramine
AVOID in delirium and intoxication, or history of paradoxical reaction
Side effects: QTc prolongation, disinhibition
Ketamine
Dissociative anesthetic
Rapid onset due to high bioavailability, which can also be given IV / IM / IN
No QT prolongation issues
Safe even in overdose (important when you aren’t sure of patient weight)
Respiratory depression if given too rapidly or overdose patient (RSI) (rarely, may see laryngospasm which is a bit more likely with IM, as is vomiting)
Avoid in schizophrenia
Clonidine
Alpha 2 central agonist – it’s like actively pushing the brakes on stimulatory output
A lot of kids are on this on a daily basis and may have it as PRNs or at night
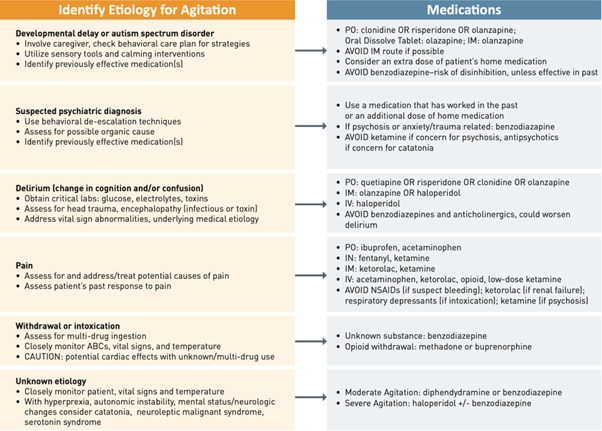
Deciding the right medication
First ask – why is the patient agitated?
- Developmental delay, autistic spectrum disorder, sensory processing disorder
- Psychiatric diagnosis
- Delirium
- Pain
- Withdrawal/intoxication
It is also important to assess the severity of the agitation as this can dictate which interventions are appropriate:
- Mild: subtle behaviours such as fidgeting, irritability, fixed stare
- Moderate: raising voice, yelling, pacing, head-banging, defensive stance
- Severe: combative, imminent risk to self or others
Always try to deescalate via non-pharmacologic means first – that’s why that was episode 2 and this is episode 3. Let’s look at management based on etiology:
As always follow local procedures and recommendations. Document what you gave and why, as well as the impact. More importantly, try non-pharmacologic means first – I cannot stress that enough.
Summary
All right, so that’s it for this episode. Hopefully you learned a bit more about how to safely chose a medication for acute agitation in children. The fourth episode in this series will shift gears and talk about safely transporting children to the ED via prehospital services.
Resources
- emDOCs.net Articles
- PEM Blog via Brad Sobolewski (@PEMTweets)
- EMSC IIC (Emergency Medical Services for Children Innovation and Improvement Center)
- EMSC IIC: Pediatric Education and Advocacy Kit (PEAK): Agitation
- EIIC/TREKK: Care of the Agitated Patient Algorithm
- EIIC/TREKK: Agitation Medication Dosing Recommendation Table
- EIIC: De-escalation Tips for Pediatric Agitation Infographic
- EIIC: Emergency Department Management of the Agitated Pediatric Patient Interactive Learning Module
- EIIC: Agitation in Neurodivergent Patients with Drs. Alice Kuo and Ilene Claudius Podcast
- EIIC: Safe Control of the Agitated Patient Webinar Series with Dr. Marianne Gausche-Hill
- New England EMSC: New England Regional Behavioral Health Toolkit
- For more info, please email km@emscimprovement.center or follow on Twitter @EMSCImprovement
- EMSC IIC: Pediatric Education and Advocacy Kit (PEAK): Agitation
Other Episodes in the Agitation Series
Episode 1: Differentiating organic versus psychiatric causes of agitation and altered mental status
Episode 2: Non-pharmacologic management of agitated children
Episode 3: Pharmacologic management of agitated children (Current)
Episode 4: Safe pre-hospital transport of the agitated child (Coming June 7, 2023)
Episode 5: Management of the child with mental health problems who is boarded in the Emergency Department (Coming June 14, 2023)
References
Gerson R, Malas N, Feuer V, Silver GH, Prasad R, Mroczkowski MM. Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry. West J Emerg Med. 2019 Mar;20(2):409-418. doi: 10.5811/westjem.2019.1.41344. Epub 2019 Feb 19. Erratum in: West J Emerg Med. 2019 May;20(3):537. Erratum in: West J Emerg Med. 2019 Jul;20(4):688-689. PMID: 30881565; PMCID: PMC6404720.
Foster AA, Saidinejad M, Duffy S, Hoffmann JA, Goodman R, Monuteaux MC, Li J. Pediatric Agitation in the Emergency Department: A Survey of Pediatric Emergency Care Coordinators. Acad Pediatr. 2023 Mar 21:S1876-2859(23)00091-8. doi: 10.1016/j.acap.2023.03.005. Epub ahead of print. PMID: 36948291.
Wong AH, Ray JM, Eixenberger C, Crispino LJ, Parker JB, Rosenberg A, Robinson L, McVaney C, Iennaco JD, Bernstein SL, Yonkers KA, Pavlo AJ. Qualitative study of patient experiences and care observations during agitation events in the emergency department: implications for systems-based practice. BMJ Open. 2022 May 11;12(5):e059876. doi: 10.1136/bmjopen-2021-059876. PMID: 35545394; PMCID: PMC9096567.
New A, Tucci VT, Rios J. A Modern-Day Fight Club? The Stabilization and Management of Acutely Agitated Patients in the Emergency Department. Psychiatr Clin North Am. 2017 Sep;40(3):397-410. doi: 10.1016/j.psc.2017.05.002. PMID: 28800797.





1 thought on “PEM Currents – Agitation in Children – Episode 3: Pharmacologic Management”
Pingback: Nerdfallmedizin.de - Nerdwoche am 11.06.2023